
The Effects of Omega-3 Fatty Acid on Vitamin D Activation in Hemodialysis Patients: A Pilot Study



Abstract
:1. Introduction
2. Results
2.1. Baseline Characteristics

{kind=link}
{kind=link}
| Cholecalciferol with Olive Oil (n = 7) | Cholecalciferol with Omega-3 FA (n = 8) | p-Value 1 | |
|---|---|---|---|
| Age (years) | 64.4 ± 8.5 | 60.0 ± 7.3 | 0.397 |
| Male, n (%) | 3 (42.9%) | 2 (25%) | 0.464 |
| DM, n (%) | 4 (57.1%) | 7 (87.5%) | 0.185 |
| 25(OH)D (ng/mL) | 10.2 ± 1.9 | 10.2 ± 4.0 | 0.613 |
| 1,25(OH)2D (pg/mL) | 24.1 ± 11.1 | 17.7 ± 8.2 | 0.336 |
| Total Cholesterol (mg/dL) | 155.3 ± 27.9 | 153.3 ± 21.0 | 0.694 |
| Triglyceride (mg/dL) | 158.4 ± 89.7 | 174.8 ± 90.3 | 0.732 |
| HDL (mg/dL) | 40.7 ± 4.7 | 48.9 ± 9.0 | 0.189 |
| LDL (mg/dL) | 90.6 ± 21.5 | 81.4 ± 19.0 | 0.463 |
| Glucose (mg/dL) | 86.7 ± 20.9 | 130.9 ± 58.1 | 0.152 |
| Calcium (mg/dL) | 8.7 ± 0.7 | 9.5 ± 1.1 | 0.189 |
| Phosphorus (mg/dL) | 5.0 ± 1.7 | 4.6 ± 1.7 | 0.694 |
| PTH (pg/mL) | 560.8 ± 236.5 | 325.9 ± 338.7 | 0.094 |
| BUN (mg/dL) | 66.3 ± 17.6 | 56.8 ± 15.8 | 0.336 |
| Creatinine (mg/dL) | 10.3 ± 3.0 | 9.6 ± 2.6 | 0.336 |
| Hemoglobin (g/dL) | 10.1 ± 1.0 | 10.9 ± 1.3 | 0.281 |
| Albumin (mg/dL) | 4.0 ± 0.2 | 3.9 ± 0.2 | 0.463 |
| CRP (mg/dL) | 1.2 ± 1.3 | 0.2 ± 0.1 | 0.014 |
| Iron (μg/dL) | 61.7 ± 12.3 | 81.3 ± 30.3 | 0.298 |
| TIBC (μg/dL) | 222.7 ± 26.7 | 241.4 ± 26.2 | 0.203 |
| Ferritin (μg/dL) | 305.0 ± 289.3 | 215.1 ± 91.6 | 0.908 |
| Calcium load (g/day) | 2354.9 ± 2023.1 | 2342.8 ± 1018.0 | 0.867 |
| Phosphate binder (%) | 5 (71.4%) | 8 (100.0%) | 0.104 |
| Vitamin D medication (%) | 4 (57.1%) | 2 (25.0%) | 0.205 |
| Cinacalcet medication (%) | 1 (14.3%) | 1 (12.5%) | 0.919 |
2.2. Diet Consumption Data
| Cholecalciferol with Olive Oil | Cholecalciferol with Omega-3 FA | |||
|---|---|---|---|---|
| Baseline | 12 Weeks | Baseline | 12 Weeks | |
| Kcal (kcal) | 1588.9 ± 435.9 | 1371.8 ± 685.2 | 1316.2 ± 383.1 | 1105.7 ± 521.6 |
| Animal protein (g) | 19.7 ± 11.9 | 21.3 ± 18.7 | 16.3 ± 6.8 | 17.6 ± 13.4 |
| Vegetable protein (g) | 26.9 ± 8.0 | 24.8 ± 12.5 | 24.4 ± 7.6 | 20.9 ± 11.4 |
| Animal lipid (g) | 12.9 ± 7.7 | 14.3 ± 11.8 | 9.5 ± 4.1 | 10.8 ± 8.1 |
| Vegetable lipid (g) | 10.6 ± 7.0 | 12.0 ± 8.9 | 8.6 ± 3.4 | 10.6 ± 4.6 |
| Carbohydrate (g) | 292.3 ± 64.6 | 236.3 ± 107.2 | 245.8 ± 64.6 | 189.8 ± 80.4 |
| Fiber (g) | 12.1 ± 4.9 | 13.0 ± 7.6 | 13.4 ± 4.2 | 12.1 ± 6.1 |
| Retinol (μg) | 108.6 ± 97.4 | 135.1 ± 77.6 | 67.5 ± 45.8 | 87.9 ± 40.6 |
| Niacin (mg) | 9.5 ± 3.6 | 9.2 ± 5.2 | 9.1 ± 3.1 | 7.6 ± 4.8 |
| Vitamin E (mg) | 9.5 ± 4.8 | 8.3 ± 4.9 | 8.4 ± 2.0 | 8.0 ± 3.9 |
| Cholesterol (mg) | 213.8 ± 154.3 | 237.7 ± 186.6 | 148.7 ± 73.5 | 236.0 ± 128.9 |
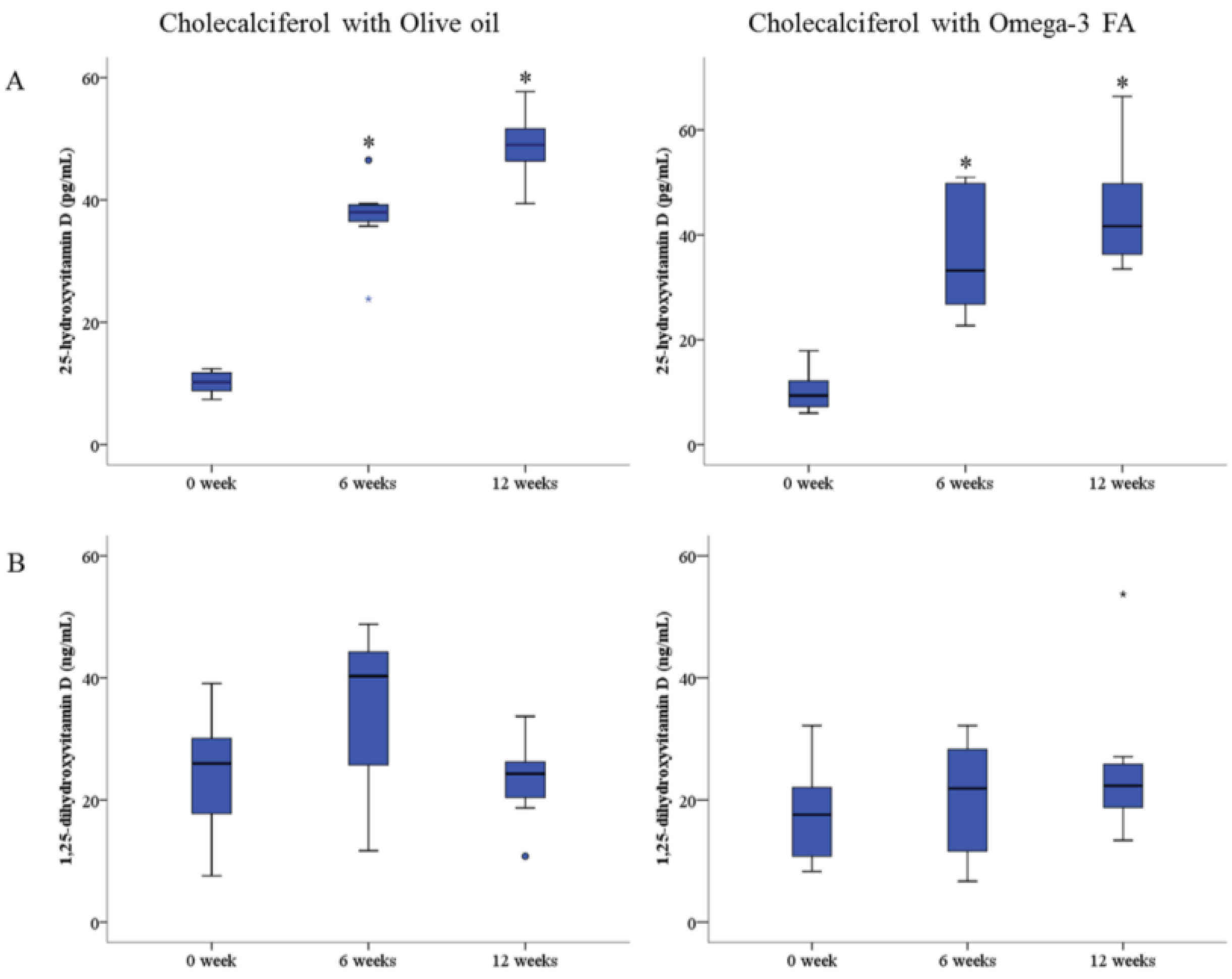
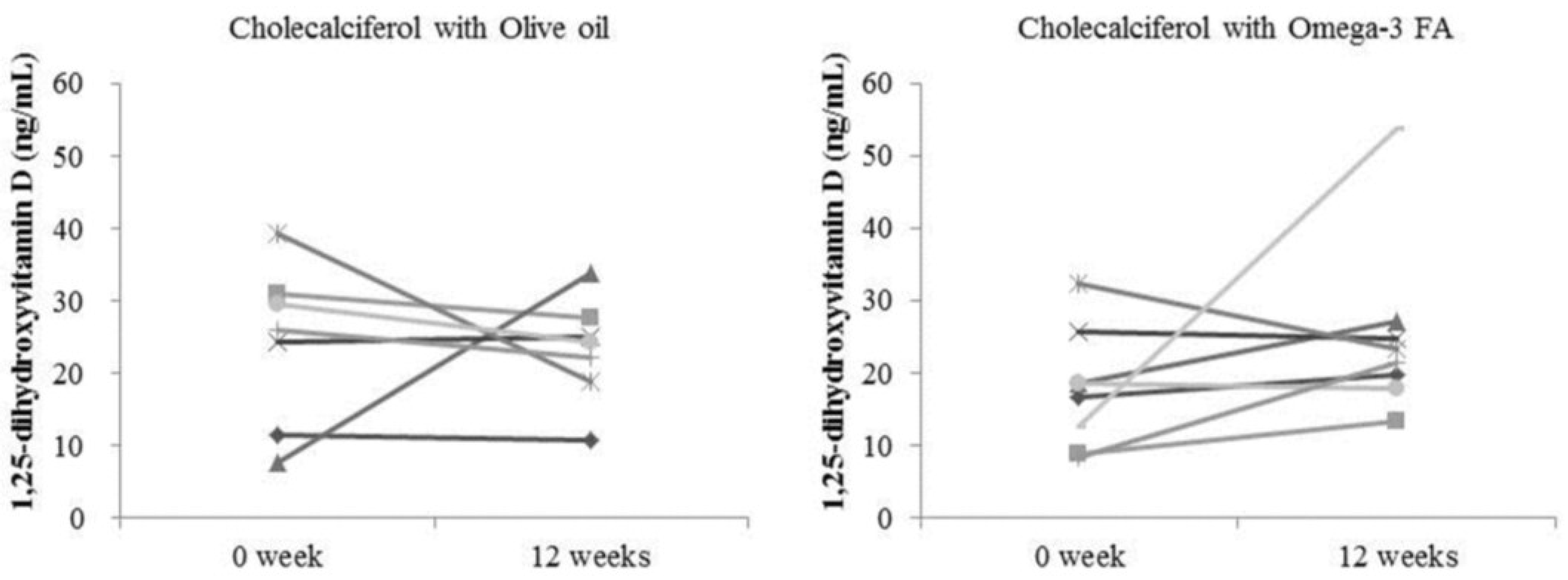
2.3. Changes in Biochemical Data
| Cholecalciferol with Olive Oil | Cholecalciferol with Omega-3 FA | |||
|---|---|---|---|---|
| Baseline | 12 Weeks | Baseline | 12 Weeks | |
| 25(OH)D (ng/mL) | 10.2 ± 1.9 | 48.9 ± 5.8 * | 10.2 ± 4.0 | 44.4 ± 10.8 * |
| 1,25(OH)2D (pg/mL) | 24.1 ± 11.1 | 23.2 ± 7.2 | 17.7 ± 8.2 | 25.1 ± 12.3 |
| 1,25(OH)2D/25(OH)D | 2.4 ± 1.1 | 0.5 ± 0.2 * | 1.8 ± 0.5 | 0.6 ± 0.3 * |
| Total Cholesterol (mg/dL) | 155.3 ± 27.9 | 159.7 ± 29.8 | 153.3 ± 21.0 | 139.0 ± 39.0 |
| Triglyceride (mg/dL) | 158.4 ± 89.7 | 123.3 ± 56.9 | 174.8 ± 90.3 | 156.0 ± 120.7 |
| HDL (mg/dL) | 40.7 ± 4.7 | 43.1 ± 5.5 | 48.9 ± 9.0 | 41.5 ± 6.5 * |
| LDL (mg/dL) | 90.6 ± 21.5 | 90.7 ± 26.0 | 81.4 ± 19.0 | 68.8 ± 28.6 * |
| Glucose (mg/dL) | 84.7 ± 20.9 | 84.1 ± 21.2 | 130.9 ± 58.1 | 128.4 ± 103.9 |
| BUN (mg/dL) | 66.3 ± 17.6 | 71.0 ± 19.7 | 56.8 ± 15.8 | 65.9 ± 14.1 |
| Creatinine (mg/dL) | 10.3 ± 3.0 | 10.9 ± 3.1 * | 9.6 ± 2.6 | 10.6 ± 1.7 |
| Hemoglobin (g/dL) | 10.1 ± 1.0 | 10.3 ± 0.7 | 10.9 ± 1.3 | 11.0 ± 1.1 |
| Albumin (mg/dL) | 4.0 ± 0.2 | 4.2 ± 0.2 | 3.9 ± 0.2 | 3.9 ± 0.2 |
| CRP (mg/dL) | 1.2 ± 1.3 | 0.9 ± 1.0 * | 0.2 ± 0.1 | 0.7 ± 1.5 |
| Fetuin-A (μg/dL) | 185.7 ± 31.9 | 180.3 ± 31.9 | 220.8 ± 49.9 | 223.4 ± 67.8 |
| FGF-23 (pg/mL) | 1737.2 ± 2344.8 | 2001.8 ± 2176.1 | 1879.5 ± 1563.2 | 2534.5 ± 2270.5 |
| Calcium (mg/dL) | 8.7 ± 0.7 | 9.3 ± 0.8 | 9.5 ± 1.1 | 9.3 ± 1.2 |
| Phosphorus (mg/dL) | 5.0 ± 1.7 | 5.4 ± 1.9 | 4.6 ± 1.7 | 5.1 ± 1.4 |
| PTH (pg/mL) | 560.8 ± 236.5 | 381.5 ± 215.6 | 325.9 ± 338.7 | 289.2 ± 273.0 |
| Iron (μg/dL) | 61.7 ± 12.3 | 67.1 ± 28.1 | 81.3 ± 30.3 | 54.6 ± 19.9 * |
| TIBC (μg/dL) | 222.7 ± 26.7 | 235.3 ± 24.1 | 241.4 ± 26.2 | 219.3 ± 23.6 * |
| Ferritin (μg/dL) | 305.0 ± 289.3 | 305.2 ± 232.8 | 215.1 ± 91.6 | 319.7 ± 174.4 |


2.4. Changes in Erythrocyte Membrane FA Content
| Cholecalciferol with Olive Oil | Cholecalciferol with Omega-3 FA | |||
|---|---|---|---|---|
| Baseline | 12 Weeks | Baseline | 12 Weeks | |
| Saturated | 47.0 ± 8.6 | 40.4 ± 0.5 | 45.1 ± 9.8 | 41.4 ± 1.2 |
| Myristic | 0.5 ± 0.2 | 0.3 ± 0.1 * | 0.5 ± 0.1 | 0.4 ± 0.1 |
| Palmitic | 25.9 ± 4.4 | 21.9 ± 0.5 * | 25.4 ± 5.1 | 23.1 ± 1.4 |
| Stearic | 20.0 ± 4.2 | 17.7 ± 0.6 | 18.8 ± 4.7 | 17.4 ± 0.6 |
| Lignoceric | 0.6 ± 0.2 | 0.4 ± 0.1 * | 0.5 ± 0.2 | 0.5 ± 0.2 |
| Monounsaturated | 17.8 ± 1.9 | 16.1 ± 0.9 * | 17.5 ± 1.5 | 15.9 ± 1.0 * |
| Palmitoleic | 0.8 ± 0.4 | 0.6 ± 0.2 | 0.7 ± 0.2 | 0.6 ± 0.2 |
| Oleic | 16.0 ± 1.6 | 14.6 ± 0.8 | 15.8 ± 1.5 | 14.5 ± 1.0 * |
| Polyunsaturated | 34.0 ± 10.3 | 42.5 ± 0.7 | 36.2 ± 11.1 | 41.7 ± 1.5 |
| Omega-6 | 23.3 ± 5.0 | 28.2 ± 2.8 | 25.8 ± 7.0 | 24.6 ± 2.3 |
| Linoleic | 9.5 ± 1.3 | 9.2 ± 1.5 | 10.0 ± 2.1 | 9.3 ± 1.4 |
| AA | 10.0 ± 4.0 | 14.1 ± 1.2 * | 11.2 ± 4.6 | 11.3 ± 1.8 |
| Omega-3 | 10.8 ± 5.7 | 14.3 ± 2.3 | 10.4 ± 4.5 | 17.1 ± 2.7 * |
| Alpha-linolenic | 0.4 ± 0.2 | 0.2 ± 0.1 * | 0.2 ± 0.1 | 0.2 ± 0.1 |
| EPA | 1.6 ± 0.9 | 2.0 ± 0.9 | 1.3 ± 0.5 | 3.9 ± 1.4 * |
| DHA | 6.9 ± 3.9 | 9.2 ± 1.5 | 6.6 ± 2.9 | 9.3 ± 1.2 * |
| Omega-3 index | 8.4 ± 4.7 | 11.2 ± 2.1 | 7.8 ± 3.4 | 13.2 ± 2.2 * |
| AA/EPA | 8.2 ± 4.6 | 8.9 ± 6.3 | 9.2 ± 3.6 | 3.5 ± 2.3 * |
| Omega-6/Omega-3 | 2.7 ± 1.3 | 2.1 ± 0.6 | 2.8 ± 1.1 | 1.5 ± 0.4 * |
| Total trans-fatty acid | 0.93 ± 0.24 | 0.91 ± 0.12 | 0.91 ± 0.24 | 0.86 ± 0.14 |
| Trans-palmitoleic acid | 0.18 ± 0.06 | 0.16 ± 0.06 | 0.22 ± 0.03 | 0.16 ± 0.05 * |
| Trans-oleic acid | 0.62 ± 0.18 | 0.53 ± 0.14 | 0.57 ± 0.17 | 0.54 ± 0.12 |
| Trans-linoleic acid | 0.31 ± 0.11 | 0.38 ± 0.17 | 0.34 ± 0.10 | 0.32 ± 0.08 |
| 18:2 n6tt | 0.06 ± 0.03 | 0.10 ± 0.09 | 0.07 ± 0.06 | 0.05 ± 0.03 |
| 18:2 n6ct | 0.10 ± 0.04 | 0.11 ± 0.02 | 0.05 ± 0.03 | 0.13 ± 0.06 |
| 18:2 n6tc | 0.15 ± 0.07 | 0.16 ± 0.08 | 0.17 ± 0.03 | 0.14 ± 0.04 |
3. Discussion
4. Materials and Methods
4.1. Study Design and Patients
4.2. Survey of Food Consumption
4.3. Laboratory Measurements
4.4. Gas Chromatography
4.5. Statistical Analysis
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Go, A.S.; Chertow, G.M.; Fan, D.; McCulloch, C.E.; Hsu, C.Y. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N. Engl. J. Med. 2004, 351, 1296–1305. [Google Scholar] [CrossRef] [PubMed]
- Tonelli, M.; Wiebe, N.; Culleton, B.; House, A.; Rabbat, C.; Fok, M.; McAlister, F.; Garg, A.X. Chronic kidney disease and mortality risk: A systematic review. JASN 2006, 17, 2034–2047. [Google Scholar] [CrossRef] [PubMed]
- Foley, R.N.; Parfrey, P.S.; Sarnak, M.J. Clinical epidemiology of cardiovascular disease in chronic renal disease. Am. J. Kidney Dis. 1998, 32, S112–S119. [Google Scholar] [CrossRef] [PubMed]
- Vanholder, R.; Massy, Z.; Argiles, A.; Spasovski, G.; Verbeke, F.; Lameire, N. Chronic kidney disease as cause of cardiovascular morbidity and mortality. Nephrol. Dial. Transplant. 2005, 20, 1048–1056. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Heimburger, O.; Lindholm, B.; Kaysen, G.A.; Bergstrom, J. Are there two types of malnutrition in chronic renal failure? Evidence for relationships between malnutrition, inflammation and atherosclerosis (mia syndrome). Nephrol. Dial. Transplant. 2000, 15, 953–960. [Google Scholar] [CrossRef] [PubMed]
- Vaziri, N.D. Role of dyslipidemia in impairment of energy metabolism, oxidative stress, inflammation and cardiovascular disease in chronic kidney disease. Clin. Exp. Nephrol. 2014, 18, 265–268. [Google Scholar] [CrossRef] [PubMed]
- Mizobuchi, M.; Towler, D.; Slatopolsky, E. Vascular calcification: The killer of patients with chronic kidney disease. JASN 2009, 20, 1453–1464. [Google Scholar] [CrossRef] [PubMed]
- LaClair, R.E.; Hellman, R.N.; Karp, S.L.; Kraus, M.; Ofner, S.; Li, Q.; Graves, K.L.; Moe, S.M. Prevalence of calcidiol deficiency in ckd: A cross-sectional study across latitudes in the united states. Am. J. Kidney Dis. 2005, 45, 1026–1033. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F. Vitamin d deficiency. N. Engl. J. Med. 2007, 357, 266–281. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Iodice, S.; Zittermann, A.; Grant, W.B.; Gandini, S. Vitamin d status and mortality risk in CKD: A meta-analysis of prospective studies. Am. J. Kidney Dis. 2011, 58, 374–382. [Google Scholar] [PubMed]
- Pilz, S.; Tomaschitz, A.; Friedl, C.; Amrein, K.; Drechsler, C.; Ritz, E.; Boehm, B.O.; Grammer, T.B.; Marz, W. Vitamin D status and mortality in chronic kidney disease. Nephrol. Dial. Transplant. 2011, 26, 3603–3609. [Google Scholar] [CrossRef] [PubMed]
- Wolf, M.; Shah, A.; Gutierrez, O.; Ankers, E.; Monroy, M.; Tamez, H.; Steele, D.; Chang, Y.; Camargo, C.A., Jr.; Tonelli, M.; et al. Vitamin D levels and early mortality among incident hemodialysis patients. Kidney Int. 2007, 72, 1004–1013. [Google Scholar] [CrossRef] [PubMed]
- Pecovnik-Balon, B.; Jakopin, E.; Bevc, S.; Knehtl, M.; Gorenjak, M. Vitamin D as a novel nontraditional risk factor for mortality in hemodialysis patients. Ther. Apher. Dial. 2009, 13, 268–272. [Google Scholar] [CrossRef]
- Drechsler, C.; Pilz, S.; Obermayer-Pietsch, B.; Verduijn, M.; Tomaschitz, A.; Krane, V.; Espe, K.; Dekker, F.; Brandenburg, V.; Marz, W.; et al. Vitamin D deficiency is associated with sudden cardiac death, combined cardiovascular events, and mortality in haemodialysis patients. Eur. Heart J. 2010, 31, 2253–2261. [Google Scholar] [CrossRef] [PubMed]
- Melamed, M.L.; Astor, B.; Michos, E.D.; Hostetter, T.H.; Powe, N.R.; Muntner, P. 25-hydroxyvitamin D levels, race, and the progression of kidney disease. JASN 2009, 20, 2631–2639. [Google Scholar] [CrossRef] [PubMed]
- Dusso, A.S.; Brown, A.J.; Slatopolsky, E. Vitamin D. Am. J. Physiol. Ren. Physiol. 2005, 289, F8–F28. [Google Scholar] [CrossRef]
- Zehnder, D.; Bland, R.; Williams, M.C.; McNinch, R.W.; Howie, A.J.; Stewart, P.M.; Hewison, M. Extrarenal expression of 25-hydroxyvitamin D(3)-1 alpha-hydroxylase. J. Clin. Endocrinol. Metab. 2001, 86, 888–894. [Google Scholar] [PubMed]
- Hewison, M.; Zehnder, D.; Chakraverty, R.; Adams, J.S. Vitamin d and barrier function: A novel role for extra-renal 1 alpha-hydroxylase. Mol. Cell. Endocrinol. 2004, 215, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Matias, P.J.; Jorge, C.; Ferreira, C.; Borges, M.; Aires, I.; Amaral, T.; Gil, C.; Cortez, J.; Ferreira, A. Cholecalciferol supplementation in hemodialysis patients: Effects on mineral metabolism, inflammation, and cardiac dimension parameters. CJASN 2010, 5, 905–911. [Google Scholar] [PubMed]
- An, W.S.; Lee, S.M.; Son, Y.K.; Kim, S.E.; Kim, K.H.; Han, J.Y.; Bae, H.R.; Rha, S.H.; Park, Y. Omega-3 fatty acid supplementation increases 1,25-dihydroxyvitamin D and fetuin-A levels in dialysis patients. Nutr. Res. 2012, 32, 495–502. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.C.; Qiao, G.; Uskokovic, M.; Xiang, W.; Zheng, W.; Kong, J. Vitamin D: A negative endocrine regulator of the renin-angiotensin system and blood pressure. J. Steroid Biochem. Mol. Biol. 2004, 89–90, 387–392. [Google Scholar] [CrossRef] [PubMed]
- Rigby, W.F.; Denome, S.; Fanger, M.W. Regulation of lymphokine production and human T lymphocyte activation by 1,25-dihydroxyvitamin d3. Specific inhibition at the level of messenger RNA. J. Clin. Investig. 1987, 79, 1659–1664. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Law, C.S.; Grigsby, C.L.; Olsen, K.; Gardner, D.G. A role for the cell cycle phosphatase Cdc25a in vitamin D-dependent inhibition of adult rat vascular smooth muscle cell proliferation. J. Steroid Biochem. Mol. Biol. 2010, 122, 326–332. [Google Scholar] [CrossRef] [PubMed]
- Martinesi, M.; Bruni, S.; Stio, M.; Treves, C. 1,25-dihydroxyvitamin D3 inhibits tumor necrosis factor-alpha-induced adhesion molecule expression in endothelial cells. Cell Biol. Int. 2006, 30, 365–375. [Google Scholar] [CrossRef] [PubMed]
- Lambert, P.W.; Stern, P.H.; Avioli, R.C.; Brackett, N.C.; Turner, R.T.; Greene, A.; Fu, I.Y.; Bell, N.H. Evidence for extrarenal production of 1 alpha, 25-dihydroxyvitamin D in man. J. Clin. Investig. 1982, 69, 722–725. [Google Scholar] [CrossRef]
- Jean, G.; Souberbielle, J.C.; Chazot, C. Monthly cholecalciferol administration in haemodialysis patients: A simple and efficient strategy for vitamin D supplementation. Nephrol. Dial. Transplant. 2009, 24, 3799–3805. [Google Scholar] [CrossRef]
- Hewison, M.; Burke, F.; Evans, K.N.; Lammas, D.A.; Sansom, D.M.; Liu, P.; Modlin, R.L.; Adams, J.S. Extra-renal 25-hydroxyvitamin D3–1alpha-hydroxylase in human health and disease. J. Steroid Biochem. Mol. Biol. 2007, 103, 316–321. [Google Scholar] [CrossRef] [PubMed]
- Tokmak, F.; Quack, I.; Schieren, G.; Sellin, L.; Rattensperger, D.; Holland-Letz, T.; Weiner, S.M.; Rump, L.C. High-dose cholecalciferol to correct vitamin D deficiency in haemodialysis patients. Nephrol. Dial. Transplant. 2008, 23, 4016–4020. [Google Scholar] [CrossRef] [PubMed]
- Leaf, A.; Kang, J.X.; Xiao, Y.F.; Billman, G.E. Clinical prevention of sudden cardiac death by n-3 polyunsaturated fatty acids and mechanism of prevention of arrhythmias by n-3 fish oils. Circulation 2003, 107, 2646–2652. [Google Scholar] [CrossRef] [PubMed]
- An, W.S.; Lee, S.M.; Son, Y.K.; Kim, S.E.; Kim, K.H.; Han, J.Y.; Bae, H.R.; Park, Y. Effect of omega-3 fatty acids on the modification of erythrocyte membrane fatty acid content including oleic acid in peritoneal dialysis patients. Prostaglandins Leukot Essent Fat. Acids 2012, 86, 29–34. [Google Scholar] [CrossRef]
- Siguel, E.N.; Lerman, R.H. Altered fatty acid metabolism in patients with angiographically documented coronary artery disease. Metabolism 1994, 43, 982–993. [Google Scholar] [CrossRef] [PubMed]
- Paganelli, F.; Maixent, J.M.; Duran, M.J.; Parhizgar, R.; Pieroni, G.; Sennoune, S. Altered erythrocyte n-3 fatty acids in mediterranean patients with coronary artery disease. Int. J. Cardiol. 2001, 78, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Block, R.C.; Harris, W.S.; Reid, K.J.; Spertus, J.A. Omega-6 and trans fatty acids in blood cell membranes: A risk factor for acute coronary syndromes? Am. Heart J. 2008, 156, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Jo, S.; An, W.S.; Park, Y. Erythrocyte n-3 polyunsaturated fatty acids and the risk of type 2 diabetes in koreans: A case-control study. Ann. Nutr. Metab. 2013, 63, 283–290. [Google Scholar] [PubMed]
- Willett, W.C.; Stampfer, M.J.; Manson, J.E.; Colditz, G.A.; Speizer, F.E.; Rosner, B.A.; Sampson, L.A.; Hennekens, C.H. Intake of trans fatty acids and risk of coronary heart disease among women. Lancet 1993, 341, 581–585. [Google Scholar] [CrossRef] [PubMed]
- Oomen, C.M.; Ocke, M.C.; Feskens, E.J.; van Erp-Baart, M.A.; Kok, F.J.; Kromhout, D. Association between trans fatty acid intake and 10-year risk of coronary heart disease in the zutphen elderly study: A prospective population-based study. Lancet 2001, 357, 746–751. [Google Scholar] [CrossRef] [PubMed]
- Lemaitre, R.N.; King, I.B.; Raghunathan, T.E.; Pearce, R.M.; Weinmann, S.; Knopp, R.H.; Copass, M.K.; Cobb, L.A.; Siscovick, D.S. Cell membrane trans-fatty acids and the risk of primary cardiac arrest. Circulation 2002, 105, 697–701. [Google Scholar] [CrossRef] [PubMed]
- Lemaitre, R.N.; King, I.B.; Mozaffarian, D.; Sotoodehnia, N.; Rea, T.D.; Kuller, L.H.; Tracy, R.P.; Siscovick, D.S. Plasma phospholipid trans fatty acids, fatal ischemic heart disease, and sudden cardiac death in older adults: The cardiovascular health study. Circulation 2006, 114, 209–215. [Google Scholar] [CrossRef]
- Mozaffarian, D.; Cao, H.; King, I.B.; Lemaitre, R.N.; Song, X.; Siscovick, D.S.; Hotamisligil, G.S. Trans-palmitoleic acid, metabolic risk factors, and new-onset diabetes in U.S. Adults: A cohort study. Ann. Int. Med. 2010, 153, 790–799. [Google Scholar] [CrossRef]
- Mozaffarian, D.; de Oliveira Otto, M.C.; Lemaitre, R.N.; Fretts, A.M.; Hotamisligil, G.; Tsai, M.Y.; Siscovick, D.S.; Nettleton, J.A. Trans-palmitoleic acid, other dairy fat biomarkers, and incident diabetes: The multi-ethnic study of atherosclerosis (mesa). Am. J. Clin. Nutr. 2013, 97, 854–861. [Google Scholar] [CrossRef] [PubMed]
- Lebreton, J.P.; Joisel, F.; Raoult, J.P.; Lannuzel, B.; Rogez, J.P.; Humbert, G. Serum concentration of human alpha 2 HS glycoprotein during the inflammatory process: Evidence that alpha 2 HS glycoprotein is a negative acute-phase reactant. J. Clin. Investig. 1979, 64, 1118–1129. [Google Scholar] [CrossRef] [PubMed]
- Triffitt, J.T.; Gebauer, U.; Ashton, B.A.; Owen, M.E.; Reynolds, J.J. Origin of plasma alpha2HS-glycoprotein and its accumulation in bone. Nature 1976, 262, 226–227. [Google Scholar] [CrossRef]
- Schafer, C.; Heiss, A.; Schwarz, A.; Westenfeld, R.; Ketteler, M.; Floege, J.; Muller-Esterl, W.; Schinke, T.; Jahnen-Dechent, W. The serum protein alpha 2-heremans-schmid glycoprotein/fetuin-a is a systemically acting inhibitor of ectopic calcification. J. Clin. Investig. 2003, 112, 357–366. [Google Scholar] [CrossRef] [PubMed]
- Stefan, N.; Hennige, A.M.; Staiger, H.; Machann, J.; Schick, F.; Krober, S.M.; Machicao, F.; Fritsche, A.; Haring, H.U. Alpha2-heremans-schmid glycoprotein/fetuin-a is associated with insulin resistance and fat accumulation in the liver in humans. Diabetes Care 2006, 29, 853–857. [Google Scholar] [CrossRef] [PubMed]
- Ix, J.H.; Shlipak, M.G.; Brandenburg, V.M.; Ali, S.; Ketteler, M.; Whooley, M.A. Association between human fetuin-A and the metabolic syndrome: Data from the heart and soul study. Circulation 2006, 113, 1760–1767. [Google Scholar] [CrossRef] [PubMed]
- Weikert, C.; Stefan, N.; Schulze, M.B.; Pischon, T.; Berger, K.; Joost, H.G.; Haring, H.U.; Boeing, H.; Fritsche, A. Plasma fetuin-a levels and the risk of myocardial infarction and ischemic stroke. Circulation 2008, 118, 2555–2562. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.Y.; Woo, J.; Lam, C.W.; Wang, M.; Chan, I.H.; Gao, P.; Lui, S.F.; Li, P.K.; Sanderson, J.E. Associations of serum fetuin-a with malnutrition, inflammation, atherosclerosis and valvular calcification syndrome and outcome in peritoneal dialysis patients. Nephrol. Dial. Transplant. 2005, 20, 1676–1685. [Google Scholar] [CrossRef] [PubMed]
- Stenvinkel, P.; Wang, K.; Qureshi, A.R.; Axelsson, J.; Pecoits-Filho, R.; Gao, P.; Barany, P.; Lindholm, B.; Jogestrand, T.; Heimburger, O.; et al. Low fetuin-a levels are associated with cardiovascular death: Impact of variations in the gene encoding fetuin. Kidney Int. 2005, 67, 2383–2392. [Google Scholar] [CrossRef] [PubMed]
- Park, M.K.; Kim, D.W.; Kim, J.; Park, S.; Joung, H.; Song, W.O.; Paik, H.Y. Development of a dish-based, semi-quantitative FFQ for the korean diet and cancer research using a database approach. Br. J. Nutr. 2011, 105, 1065–1072. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, S.M.; Son, Y.K.; Kim, S.E.; An, W.S. The Effects of Omega-3 Fatty Acid on Vitamin D Activation in Hemodialysis Patients: A Pilot Study. Mar. Drugs 2015, 13, 741-755. https://doi.org/10.3390/md13020741
Lee SM, Son YK, Kim SE, An WS. The Effects of Omega-3 Fatty Acid on Vitamin D Activation in Hemodialysis Patients: A Pilot Study. Marine Drugs. 2015; 13(2):741-755. https://doi.org/10.3390/md13020741
Chicago/Turabian StyleLee, Su Mi, Young Ki Son, Seong Eun Kim, and Won Suk An. 2015. "The Effects of Omega-3 Fatty Acid on Vitamin D Activation in Hemodialysis Patients: A Pilot Study" Marine Drugs 13, no. 2: 741-755. https://doi.org/10.3390/md13020741