Prevalence, Discontinuation Rate, and Risk Factors for Severe Local Site Reactions with Topical Field Treatment Options for Actinic Keratosis of the Face and Scalp


Abstract
:1. Introduction
2. Severe Local Site Reactions with Topical Field Treatment for Actinic Keratosis of the Face and Scalp
2.1. Prevalence of Severe Local Site Reactions
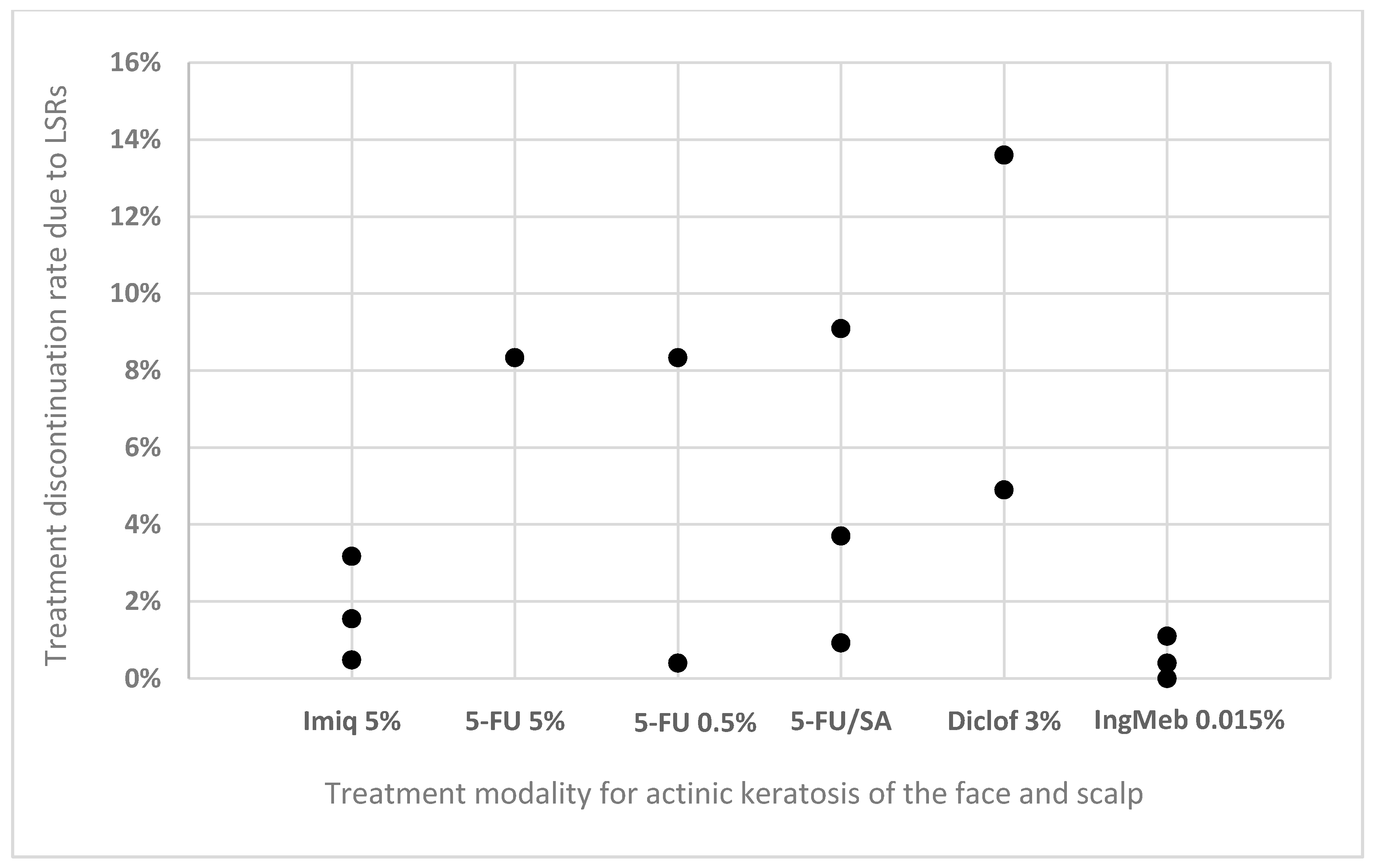
2.2. Treatment Discontinuation Due to Local Site Reactions
2.3. Therapy-Unrelated Risk Factors for Development of Local Site Reactions with Increased Severity
3. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dréno, B.; Amici, J.M.; Basset-Seguin, N.; Cribier, B.; Claudel, J.P.; Richard, M.A. Management of actinic keratosis: A practical report and treatment algorithm from AKTeamTM expert clinicians. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 1141–1149. [Google Scholar] [CrossRef] [PubMed]
- Dziunycz, P.J.; Schuller, E.; Hofbauer, G.F.L. Prevalence of Actinic Keratosis in Patients Attending General Practitioners in Switzerland. Dermatology 2018, 234, 214–219. [Google Scholar] [CrossRef]
- Zalaudek, I.; Piana, S.; Moscarella, E.; Longo, C.; Zendri, E.; Castagnetti, F.; Pellacani, G.; Lallas, A.; Argenziano, G. Morphologic grading and treatment of facial actinic keratosis. Clin. Dermatol. 2014, 32, 80–87. [Google Scholar] [CrossRef]
- Olsen, E.A.; Abernethy, M.L.; Kulp-Shorten, C.; Callen, J.P.; Glazer, S.D.; Huntley, A.; McCray, M.; Monroe, A.B.; Tschen, E.; Wolf, J.E., Jr. A double-blind, vehicle-controlled study evaluating masoprocol cream in the treatment of actinic keratoses on the head and neck. J. Am. Acad. Dermatol. 1991, 24, 738–743. [Google Scholar] [PubMed]
- Fernández-Figueras, M.T.; Carrato, C.; Sáenz, X.; Puig, L.; Musulen, E.; Ferrándiz, C.; Ariza, A. Actinic keratosis with atypical basal cells (AK I) is the most common lesion associated with invasive squamous cell carcinoma of the skin. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 991–997. [Google Scholar] [CrossRef]
- Neri, L.; Peris, K.; Longo, C.; Calvieri, S.; Frascione, P.; Parodi, A.; Eibenschuz, L.; Bottoni, U.; Pellacani, G.; The Actinic Keratosis—TReatment Adherence INitiative (AK-TRAIN) Study Group. Physician—Patient communication and patient-reported outcomes in the actinic keratosis treatment adherence initiative (AK-TRAIN): A multicenter, prospective, real-life study of treatment satisfaction, quality of life and adherence to topical field-direc. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 93–107. [Google Scholar] [CrossRef]
- Hanke, W.C.; Norlin, J.M.; Mark, K.; Larsson, T.; Stone, S. Quality of life in treatment of AK: Treatment burden of ingenol mebutate gel is small and short lasting. J. Dermatol. Treat. 2016, 27, 450–455. [Google Scholar]
- Strohal, R.; Kerl, H.; Schuster, L. Treatment of actinic keratoses with 5% topical imiquimod: A multicenter prospective observational study from 93 Austrian office-based dermatologists. J. Drugs Dermatol. 2012, 11, 574–578. [Google Scholar] [PubMed]
- Stockfleth, E.; Peris, K.; Guillen, C.; Cerio, R.; Basset-Seguin, N.; Foley, P.; Sanches, J.; Culshaw, A.; Erntoft, S.; Lebwohl, M. Physician perceptions and experience of current treatment in actinic keratosis. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 298–306. [Google Scholar] [CrossRef] [PubMed]
- Stockfleth, E.; Kerl, H.; Zwingers, T.; Willers, C. Low-dose 5-fluorouracil in combination with salicylic acid as a new lesion-directed option to treat topically actinic keratoses: Histological and clinical study results. Br. J. Dermatol. 2011, 165, 1101–1108. [Google Scholar] [CrossRef]
- Sotiriou, E.; Apalla, Z.; Vrani, F.; Lazaridou, E.; Vakirlis, E.; Lallas, A.; Ioannides, D. Daylight photodynamic therapy vs. Conventional photodynamic therapy as skin cancer preventive treatment in patients with face and scalp cancerization: An intra-individual comparison study. J. Eur. Acad. Dermatol. Venereol. 2017, 31, 1303–1307. [Google Scholar] [CrossRef] [PubMed]
- Lebwohl, M.; Dinehart, S.; Whiting, D.; Lee, P.K.; Tawfik, N.; Jorizzo, J.; Lee, J.H.; Fox, T.L. Imiquimod 5% cream for the treatment of actinic keratosis: Results from two phase III, randomized, double-blind, parallel group, vehicle-controlled trials. J. Am. Acad. Dermatol. 2004, 50, 714–721. [Google Scholar] [CrossRef] [PubMed]
- Swanson, N.; Abramovits, W.; Berman, B.; Kulp, J.; Rigel, D.S.; Levy, S. Imiquimod 2.5% and 3.75% for the treatment of actinic keratoses: Results of two placebo-controlled studies of daily application to the face and balding scalp for two 2-week cycles. J. Am. Acad. Dermatol. 2010, 62, 582–590. [Google Scholar] [CrossRef] [PubMed]
- Hanke, W.; Beer, K.R.; Stockfleth, E.; Wu, J.; Rosen, T.; Levy, S. Imiquimod 2.5% and 3.75% for the treatment of actinic keratoses: Results of two placebo-controlled studies of daily application to the face and balding scalp for two 3-week cycles. J. Am. Acad. Dermatol. 2010, 62, 573–581. [Google Scholar] [CrossRef] [PubMed]
- Skroza, N.; Proietti, I.; Bernardini, N.; Balduzzi, V.; Mambrin, A.; Marchesiello, A.; Tolino, E.; Zuber, S.; la Torre, G.; Potenza, C. Factors influencing response to ingenol mebutate therapy for actinic keratosis of face and scalp. World J. Clin. Oncol. 2017, 8, 405–411. [Google Scholar] [CrossRef] [PubMed]
- Jim On, S.C.; Knudsen, K.M.; Skov, T.; Lebwohl, M. Relationship between severity of the local skin reactions and the rate of local skin reaction resolution in patients treated with ingenol mebutate gel. Clin. Cosmet. Investig. Dermatol. 2016, 9, 211–216. [Google Scholar] [PubMed]
- Lebwohl, M.; Swanson, N.; Anderson, L.L.; Melgaard, A.; Xu, Z.; Berman, B. Ingenol Mebutate Gel for Actinic Keratosis. N. Engl. J. Med. 2012, 366, 1010–1019. [Google Scholar] [CrossRef]
- Stough, D.; Bucko, A.D.; Vamvakias, G.; Rafal, E.S.; Davis, S.A. Fluorouracil Cream 0.5% for the Treatment of Actinic Keratoses on the Face Interim Results of an 18-Month Open-Label Study. J. Clin. Aesthet. Dermatol. 2008, 1, 16–21. [Google Scholar]
- Pflugfelder, A.; Welter, A.K.; Leiter, U.; Weide, B.; Held, L.; Eigentler, T.K.; Dirschka, T.; Stockfleth, E.; Nashan, D.; Garbe, C. Open label randomized study comparing 3 months vs. 6 months treatment of actinic keratoses with 3% diclofenac in 2.5% hyaluronic acid gel: A trial of the German Dermatologic Cooperative Oncology Group. J. Eur. Acad. Dermatol. Venereol. 2012, 26, 48–53. [Google Scholar] [CrossRef]
- Simon, J.C.; Dominicus, R.; Karl, L.; Rodriguez, R.; Willers, C.; Dirschka, T. A prospective randomized exploratory study comparing the efficacy of once-daily topical 0.5% 5-fluorouracil in combination with 10.0% salicylic acid (5-FU/SA) vs. cryosurgery for the treatment of hyperkeratotic actinic keratosis. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 881–889. [Google Scholar] [CrossRef]
- Sotiriou, E.; Evangelou, G.; Papadavid, E.; Apalla, Z.; Vrani, F.; Vakirlis, E.; Panagiotou, M.; Stefanidou, M.; Pombou, T.; Krasagakis, K.; et al. Conventional vs. daylight photodynamic therapy for patients with actinic keratosis on face and scalp: 12-month follow-up results of a randomized, intra-individual comparative analysis. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 595–600. [Google Scholar] [CrossRef] [PubMed]
- See, J.A.; Gebauer, K.; Wu, J.K.; Manoharan, S.; Kerrouche, N.; Sullivan, J. High Patient Satisfaction with Daylight-Activated Methyl Aminolevulinate Cream in the Treatment of Multiple Actinic Keratoses: Results of an Observational Study in Australia. Dermatol. Ther. 2017, 7, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Rubel, D.M.; Spelman, L.; Murrell, D.F.; See, J.A.; Hewitt, D.; Foley, P.; Bosc, C.; Kerob, D.; Kerrouche, N.; Wulf, H.C.; et al. Daylight photodynamic therapy with methyl aminolevulinate cream as a convenient, similarly effective, nearly painless alternative to conventional photodynamic therapy in actinic keratosis treatment: A randomized controlled trial. Br. J. Dermatol. 2014, 171, 1164–1171. [Google Scholar] [CrossRef] [PubMed]
- Serra-Guillén, C.; Nagore, E.; Llombart, B.; Sanmartín, O.; Requena, C.; Calomarde, L.; Guillén, C. A 12-Day Course of Imiquimod 5% for the Treatment of Actinic Keratosis: Effectiveness and Local Reactions. Actas Dermo-Sifiliográficas 2018, 109, 248–253. [Google Scholar] [CrossRef] [PubMed]
- Rivers, J.K.; Rosoph, L.; Provost, N.; Bissonnette, R. Open-label study to assess the safety and efficacy of imiquimod 5% cream applied once daily three times per week in cycles for treatment of actinic keratoses on the head. J. Cutan. Med. Surg. 2008, 12, 97–101. [Google Scholar] [CrossRef] [PubMed]
- Stockfleth, E.; Sterry, W.; Carey-Yard, M.; Bichel, J. Multicentre, open-label study using imiquimod 5% cream in one or two 4-week courses of treatment for multiple actinic keratoses on the head. Br. J. Dermatol. 2007, 157, 41–46. [Google Scholar] [CrossRef]
- Alomar, A.; Bichel, J.; McRae, S. Vehicle-controlled, randomized, double-blind study to assess safety and efficacy of imiquimod 5% cream applied once daily 3 days per week in one or two courses of treatment of actinic keratoses on the head. Br. J. Dermatol. 2007, 157, 133–141. [Google Scholar] [CrossRef]
- Korman, N.; Moy, R.; Ling, M.; Matheson, R.; Smith, S.; McKane, S.; Lee, J.H. Dosing With 5% Imiquimod Cream 3 Times per Week for the Treatment of Actinic Keratosis. Arch. Dermatol. 2005, 141, 467–473. [Google Scholar] [CrossRef]
- Rosen, R.; Marmur, E.; Anderson, L.; Welburn, P.; Katsamas, J. A New, Objective, Quantitative Scale for Measuring Local Skin Responses Following Topical Actinic Keratosis Therapy with Ingenol Mebutate. Dermatol. Ther. 2014, 4, 207–219. [Google Scholar] [CrossRef]
- Stockfleth, E.; Von Kiedrowski, R.; Dominicus, R.; Ryan, J.; Ellery, A.; Falque, M. Efficacy and Safety of 5-Fluorouracil 0.5%/Salicylic Acid 10 % in the Field-Directed Treatment of Actinic Keratosis: A Phase III, Randomized, Double-Blind, Vehicle-Controlled Trial. Dermatol. Ther. 2017, 9, 81–96. [Google Scholar] [CrossRef]
- Askew, D.A.; Mickan, S.M.; Soyer, H.P.; Wilkinson, D. Effectiveness of 5-fluorouracil treatment for actinic keratosis—A systematic review of randomized controlled trials. Int. J. Dermatol. 2009, 48, 453–463. [Google Scholar] [CrossRef]
- Tanghetti, E.; Werschler, W.P. Comparison of 5% 5-Fluorouracil Cream and 5% Imiquimod Cream in the Management of Actinic Keratoses on the Face and Scalp. J. Drugs Dermatol. 2007, 6, 144–147. [Google Scholar] [PubMed]
- Stockfleth, E.; Zwingers, T.; Willers, C. Recurrence rates and patient assessed outcomes of 0.5% 5-fluorouracil in combination with salicylic acid treating actinic keratoses. Eur. J. Dermatol. 2012, 22, 370–374. [Google Scholar]
- Smith, S.; Piacquadio, D.; Morhenn, V.; Atkin, D.; Fitzpatrick, R. Short Incubation PDT versus 5-FU in Treating Actinic Keratoses. J. Drugs Dermatol. 2003, 2, 629–635. [Google Scholar] [PubMed]
- Samorano, L.P.; Torezan, L.A.; Sanches, J.A. Evaluation of the tolerability and safety of a 0.015% ingenol mebutate gel compared to 5% 5-fluorouracil cream for the treatment of facial actinic keratosis: A prospective randomized trial. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1822–1827. [Google Scholar] [CrossRef] [PubMed]
- Stockfleth, E.; Ulrich, C.; Langeasschenfeldt, B.; Kremer, H.J.; Drecoll, U.; Maus, J.; Röwert-Huber, J. Treatment of multiple, multiform actinic keratoses on the head with imiquimod 5% cream. Eur. J. Dermatol. 2009, 19, 355–359. [Google Scholar] [PubMed]
- Ricci, F.; Tambone, S.; Neri, L.; Fania, L.; Piccioni, A.; Guerriero, C.; Fargnoli, M.C.; Peris, K. Real-life efficacy and safety of ingenol mebutate for the treatment of actinic keratosis of the face and scalp: A single arm retrospective study. J. Dermatol. Treat. 2016, 27, 525–530. [Google Scholar] [CrossRef] [PubMed]
- Fargnoli, M.C.; Piccioni, A.; Neri, L.; Tambone, S.; Pellegrini, C.; Peris, K. Conventional vs. daylight methyl aminolevulinate photodynamic therapy for actinic keratosis of the face and scalp: An intra-patient, prospective, comparison study in Italy. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 1926–1932. [Google Scholar] [CrossRef] [PubMed]
- Flohil, S.C.; Van Der Leest, R.J.T.; Dowlatshahi, E.A.; Hofman, A.; De Vries, E.; Nijsten, T. Prevalence of actinic keratosis and its risk factors in the general population: The Rotterdam study. J. Investig. Dermatol. 2013, 133, 1971–1978. [Google Scholar] [CrossRef] [PubMed]
- Galvão, L.E.G.; Botelho, K.P.; de Sá Gonçalves, H.; Caldas, J.C. Daylight photodynamic therapy—Experience and safety in treatment of actinic keratoses of the face and scalp in low latitude and high brightness region. An. Bras. Dermatol. 2017, 92, 142–144. [Google Scholar] [CrossRef]
- Ortega del Olmo, R.; Salido-Vallejo, R. Ingenol mebutate for the treatment of actinic keratosis: Effectiveness and safety in 246 patients treated in real-life clinical practice. J. Dermatol. Treat. 2018, 29, 393–399. [Google Scholar] [CrossRef] [PubMed]
- Joe, H.J.; Oh, B.H. Ingenol mebutate in low amounts for the treatment of actinic keratosis in Korean patients. Clin. Cosmet. Investig. Dermatol. 2017, 10, 93–98. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author | Year of Publication | Treatment Modality | Number of Patients | Application Frequency | Overall Prevalence of LSR | Prevalence of Severe LSR | Prevalence of Systemic Symptoms |
|---|---|---|---|---|---|---|---|
| Sotiriou et al. [21] | 2018 | DL-PDT with MAL | 46 | Once | 71.6% | 0% | 0% |
| Sotiriou et al. [11] | 2017 | DL-PDT with MAL | 26 | Once | 69.2% | 0% | 0% |
| See et al. [22] | 2017 | DL-PDT with MAL | 81 | Once | 44.4% * (erythema) | 1.2% | 0% |
| Rubel et al. [23] | 2014 | DL-PDT with MAL | 100 | Once | 39.0% | 0% | 0% |
| Serra-Guillén et al. [24] | 2017 | Imiquimod 5% | 65 | Once daily for 12 consecutive days | 100% | 58.5% | 20% |
| Rivers et al. [25] | 2008 | Imiquimod 5% | 42 | Three times per week for 4 weeks followed by 4 weeks of rest and second cycle if needed | 95.2% * (erythema) | 8.8% * (scabbing or crusting) | 14% * (upper respiratory infection) |
| Stockfleth et al. [26] | 2007 | Imiquimod 5% | 828 | Three times per week for 4 weeks followed by 4 weeks of rest and second cycle if needed | NR | 31.8% * (erythema) | 6% * (headache) |
| Alomar et al. [27] | 2007 | Imiquimod 5% | 129 | Three times per week for 4 weeks followed by 4 weeks of rest and second cycle if needed | 96.9% * (erythema) | 31.0% * (erythema) | NR |
| Korman et al. [28] | 2005 | Imiquimod 5% | 241 | Three times per week for 16 weeks | 98.3% * (erythema) | 33.2% * (erythema) | NR |
| Lebwohl et al. [12] | 2004 | Imiquimod 5% | 215 | Twice per week for 16 weeks | 97.2% * (erythema) | 17.7% * (erythema) | NR |
| Swanson et al. [13] | 2010 | Imiquimod 3.75% | 160 | Once daily 2-week on/off/on cycle | Almost all | 33.8% | NR |
| Hanke et al. [14] | 2010 | Imiquimod 3.75% | 162 | Once daily 3-week on/off/on cycle | Almost all | 54.9% | 8% * (Influenza-like illness) |
| Skroza et al. [15] | 2017 | Ingenol mebutate gel 0.015% | 130 | Once daily for 3 consecutive days | 100% | 17.7% * (edema) | 0% |
| Jim On et al. [16] | 2016 | Ingenol mebutate gel 0.015% | 274 | Once daily for 3 consecutive days, | 100% | 24.5% | NR |
| Pflugfelder et al. [19] | 2012 | 3% diclofenac in 2.5% hyaluronic acid gel | 418 | Twice daily for 3 or 6 months | NR | 13.6% | NR |
| Stockfleth et al. [10] | 2011 | 3% diclofenac in 2.5% hyaluronic acid gel | 185 | Twice daily for up to 12 weeks | 62.7% | 11.9% ** | |
| Simon et al. [20] | 2015 | 5-fluorouracil 0.5%⁄salicylic acid 10.0% | 33 | Once daily for up to 6 weeks | 8.8% * (erythema) | 18.2% | NR |
| Stockfleth et al. [10] | 2011 | 5-fluorouracil 0.5%⁄salicylic acid 10.0% | 187 | Once daily for up to 12 weeks | 92.0% | 27.8% ** | |
| Stough et al. [18] | 2008 | 5-fluorouracil 0.5% | 277 | Once daily for up to 4 weeks | 87.0% | 19.1% | NR |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Balcere, A.; Rone Kupfere, M.; Čēma, I.; Krūmiņa, A. Prevalence, Discontinuation Rate, and Risk Factors for Severe Local Site Reactions with Topical Field Treatment Options for Actinic Keratosis of the Face and Scalp. Medicina 2019, 55, 92. https://doi.org/10.3390/medicina55040092
Balcere A, Rone Kupfere M, Čēma I, Krūmiņa A. Prevalence, Discontinuation Rate, and Risk Factors for Severe Local Site Reactions with Topical Field Treatment Options for Actinic Keratosis of the Face and Scalp. Medicina. 2019; 55(4):92. https://doi.org/10.3390/medicina55040092
Chicago/Turabian StyleBalcere, Alise, Māra Rone Kupfere, Ingrīda Čēma, and Angelika Krūmiņa. 2019. "Prevalence, Discontinuation Rate, and Risk Factors for Severe Local Site Reactions with Topical Field Treatment Options for Actinic Keratosis of the Face and Scalp" Medicina 55, no. 4: 92. https://doi.org/10.3390/medicina55040092