Diagnosis of Obstructive Sleep Apnea in Patients with Allergic and Non-Allergic Rhinitis

 , , , , , ,
, , , , , ,  , and
, and
Abstract
:1. Introduction
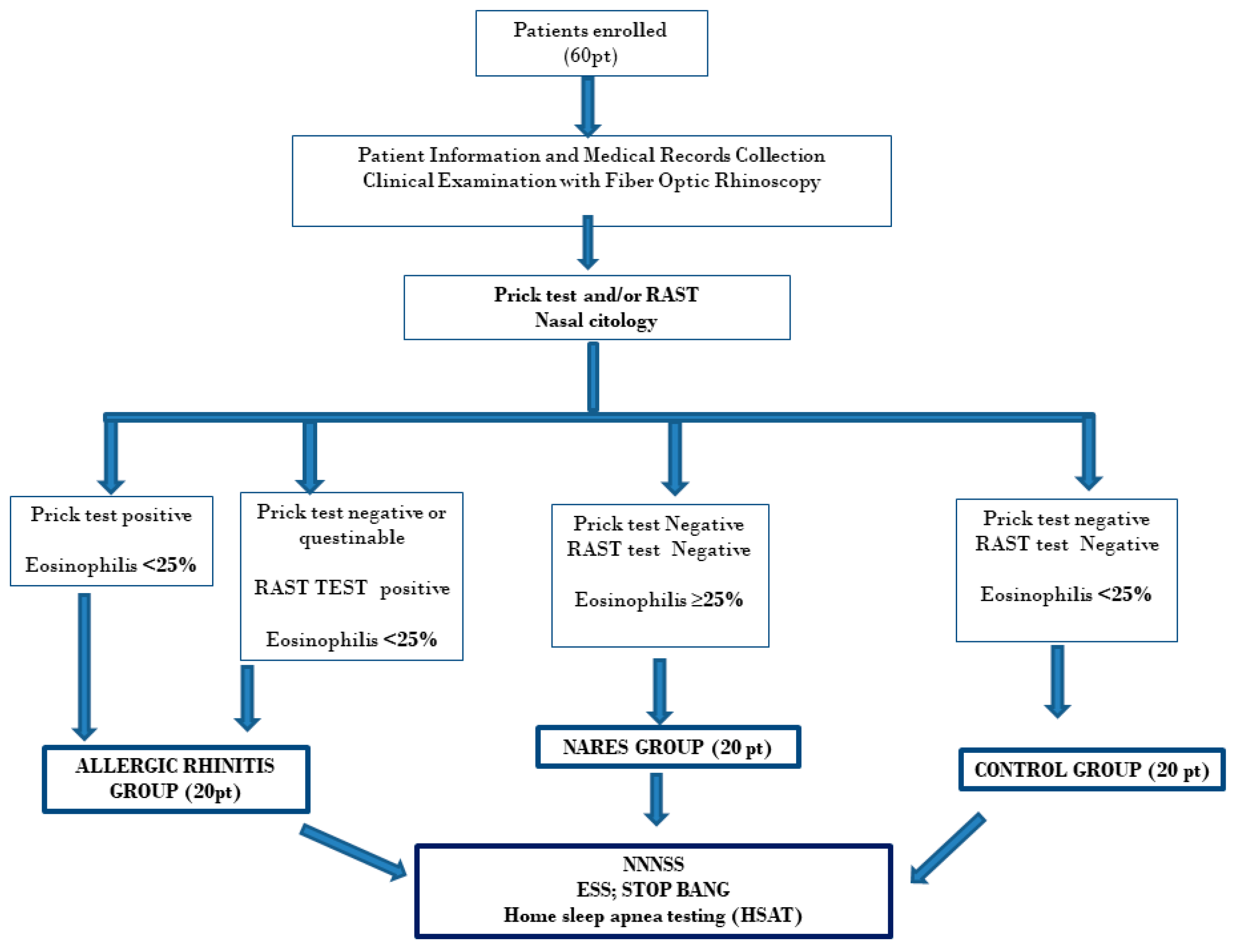
2. Materials and Methods
2.1. Allergic Rhinitis Diagnosis
2.2. NARES Diagnosis
2.3. Non-Nasal Symptom (NNSS) Severity Investigation
2.4. STOP BANG and ESS
2.5. Home Sleep Apnea Testing (HSAT)
2.6. Statistical Analysis
3. Results
3.1. Nasal Cytology
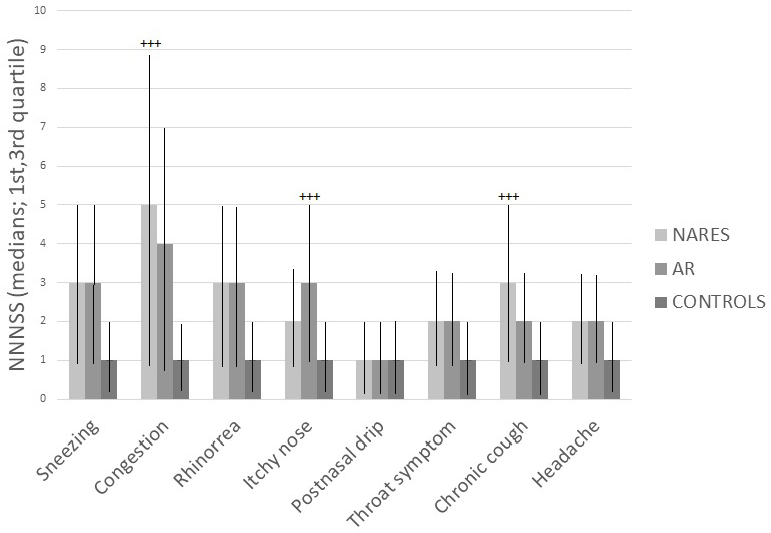
3.2. NNNSS
3.3. STOP-BANG and ESS
3.4. Home Sleep Apnea Testing (HSAT)
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Emeryk, A.; Emeryk-Maksymiuk, J.; Janeczek, K. New Guidelines for the Treatment of Seasonal Allergic Rhinitis. Postepy Derm. Alergol. 2019, 36, 255–260. [Google Scholar] [CrossRef] [PubMed]
- Brożek, J.L.; Bousquet, J.; Baena-Cagnani, C.E.; Bonini, S.; Canonica, G.W.; Casale, T.B.; van Wijk, R.G.; Ohta, K.; Zuberbier, T.; Holger, J. Allergic Rhinitis and Its Impact on Asthma (ARIA) Guidelines: 2010 Revision. J. Allergy Clin. Immunol. 2010, 126, 466–476. [Google Scholar] [CrossRef]
- Ellis, A.K.; Keith, P.K. Non-allergic rhinitis with eosinophilia syndrome. Curr. Allergy Asthma Rep. 2006, 6, 215–220. [Google Scholar] [CrossRef] [PubMed]
- Moneret-Vautrin, D.A.; Hsieh, V.; Wayoff, M.; Guyot, J.L.; Mouton, C.; Maria, Y. Non-allergic rhinitis with eosinophilia syndrome a precursor of the triad: Nasal polyposis, intrinsic asthma, and intolerance to aspirin. Ann. Allergy 1990, 64, 513–518. [Google Scholar] [PubMed]
- Settipane, G.A.; Klein, D.E. Non allergic rhinitis: Demography of eosinophils in nasal smear, blood total eosinophil counts and IgE levels. N. Engl. Reg. Allergy Proc. 1985, 6, 363–366. [Google Scholar] [CrossRef] [PubMed]
- Benjafield, A.V.; Ayas, N.T.; Eastwood, P.R. Estimation of the Global Prevalence and Burden of Obstructive Sleep Apnoea: A Literature-Based Analysis. Lancet Respir. Med. 2019, 7, 687–698. [Google Scholar] [CrossRef] [Green Version]
- Mullol, B.; Douglas, G.; Hopkins, K. EPOS 2012: European position paper on rhinosinusitisand nasal polyps 2012. A summary for otorhinolaryngologists. Rhinology 2012, 50, 1–12. [Google Scholar]
- Fokkens, W.J. Thoughts on the patho-physiology of non-allergic rhinitis. Curr. Allergy Asthma Rep. 2002, 2, 203–209. [Google Scholar] [CrossRef]
- Young, T.; Finn, L.; Palta, M. Chronic nasal congestion at night is a risk factor for snoring in a population-based cohort study. Arch. Intern. Med. 2001, 161, 1514–1519. [Google Scholar] [CrossRef]
- Georgalas, C. The role of the nose in snoring and obstructive sleep apnoea: An update. Eur. Arch. Otolaryngol. 2011, 268, 1365–1373. [Google Scholar] [CrossRef] [Green Version]
- Brożek, J.L.; Bousquet, J.; Agache, I. Allergic rhinitis and its impact on asthma (ARIA) guidelines-2016 revision. J. Allergy Clin. Immunol. 2017, 140, 950–958. [Google Scholar] [CrossRef] [Green Version]
- Salzano, F.A.; Marino, L.; Salzano, G.; Botta, R.M.; Cascone, G.; D’Agostino Fiorenza, U.; Selleri, C.; Casolaro, V. Microbiota Composition and the Integration of Exogenous and Endogenous Signals in Reactive Nasal Inflammation. J. Immunol. Res. 2018, 3, 2724951. [Google Scholar] [CrossRef] [PubMed]
- Scadding, G.K.; Kariyawasam, H.H.; Scadding, G. BSACI Guideline for the Diagnosis and Management of Allergic and Non-Allergic Rhinitis (Revised Edition 2017; First Edition 2007). Clin. Exp. Allergy. 2017, 47, 856–889. [Google Scholar] [CrossRef] [PubMed]
- Alkhalil, M.; Schulman, E.; Getsy, J. Obstructive sleep apnea syndrome and asthma: What are the links? J. Clin. Sleep Med. 2009, 5, 71–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, S.S. Flow-regulatory function of upper airway in health and disease: A unified pathogenetic view of sleep-disordered breathing. Lung 1993, 171, 311–333. [Google Scholar] [CrossRef] [PubMed]
- Smith, P.L.; Wise, R.A.; Gold, A.R.; Schwartz, A.R.; Permutt, S. Upper airway pressure-flow relationships in obstructive sleep apnea. J. Appl. Physiol. 1988, 64, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Davidson, T.M. The great leap forward: The anatomic basis for the acquisition of speech and obstructive sleep apnea. Sleep Med. 2003, 4, 185–194. [Google Scholar] [CrossRef]
- McNicholas, W.T.; Tarlo, S.; Cole, P.; Zamel, N.; Rutherford, R.; Griffin, D.; Phillipson, E.A. Obstructive apneas during sleep in patients with seasonal allergic rhinitis. Am. Rev. Resp. Dis. 1982, 126, 625–628. [Google Scholar]
- Magliulo, G.; Iannella, G.; Ciofalo, A.; Polimeni, A.; De Vincentiis, M.; Pasquariello, B.; Montevecchi, F.; Vicini, C. Nasal pathologies in patients with obstructive sleep apnoea patologie nasali in pazienti affetti da syndrome delle apnee ostruttive del sonno. Acta Otorhinolaryngol. Ital. 2019, 38, 1–7. [Google Scholar]
- Magliulo, G.; De Vincentiis, M.; Iannella, G.; Ciofalo, A.; Pasquariello, B.; Manno, A.; Angeletti, D.; Polimeni, A. Olfactory Evaluation in Obstructive Sleep Apnoea Patients. Acta Otorhinolaryngol. Ital. 2018, 38, 338–345. [Google Scholar]
- Gül, A.; Cınar, F.; Evren, C.; Uğur, M.B.; Sarıkaya, S. The prevalence of allergic rhinitis in patients with simple snoring and obstructive sleep apnea syndrome. Kulak Burun Bogaz Ihtis Derg. 2011, 21, 70–75. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochford, S.; Rochford, P.; Sutherland, M.F. Atopy is frequent among obstructive sleep apnoea patients undergoing skin prick testing and polysomnography in a public hospital. Intern. Med. J. 2009, 39, 139–161. [Google Scholar]
- Kumar, R.; Nagar, D.; Mallick, A.; Kumar, M.; Tarke, C.R.; Goel, N. Obstructive sleep apnea and atopy among middle-aged chronic obstructive pulmonary disease and bronchial asthma patients. J. Assoc. Phys. India 2013, 61, 615–618. [Google Scholar]
- Braido, F.; Baiardini, I.; Lacedonia, D.; Facchini, F.M.; Fanfulla, F.; Molinengo, G.; Canonica, G.W. Sleep apnea risk in subjects with asthma with or without comorbid rhinitis. Respir. Care 2014, 59, 1851–1855. [Google Scholar] [CrossRef] [Green Version]
- Bozkurt, B.; Ugur, K.S.; Karamanli, H.; Kucuker, F.; Ozol, D. Polysomnographic Findings in Persistent Allergic Rhinitis. Sleep Breath 2017, 21, 255–261. [Google Scholar] [CrossRef]
- Kramer, M.F.; de la Chaux, R.; Fintelmann, R.; Rasp, G. Nares: A risk factor for obstructive sleep apnea? Am. J. Otolaryngol. 2004, 25, 173–177. [Google Scholar] [CrossRef] [PubMed]
- Kalpaklioğlu, A.F.; Kavut, A.B.; Ekici, M. Allergic and non-allergic rhinitis: The threat for obstructive sleep apnea. Ann. Allergy Asthma Immunol. 2009, 103, 20–25. [Google Scholar] [CrossRef]
- Vicini, C.; De Vito, A.; Benazzo, M.; Frassineti, S.; Campanini, A.; Frasconi, P.; Mira, E. The nose oropharynx hypopharynx and larynx (NOHL) classification: A new system of diagnostic standardized examination for OSAHS patients. Eur. Arch. Otorhinolaryngol. 2012, 269, 1297–1300. [Google Scholar] [CrossRef]
- Park, C.E.; Shin, S.Y.; Lee, K.H.; Cho, J.S.; Kim, S.W. The effect of allergic rhinitis on the degree of stress, fatigue and quality of life in OSA patients. Eur. Arch. Otorhinolaryngol. 2012, 269, 2061–2064. [Google Scholar] [CrossRef]
- Stuck, B.A.; Czajkowski, J.; Hagner, A.E.; Klimek, L.; Verse, T.; Hörmann, K.; Maurer, J.T. Changes in daytime sleepiness, quality of live, and objective sleep patterns in seasonal allergic rhinitis: A controlled clinical trial. J. Allergy Clin. Immunol. 2004, 113, 663–668. [Google Scholar] [CrossRef]
- Gelardi, M. Atlas of Nasal Cytology, 2nd ed.; Edi Ermes: Milano, MI, Italy, 2012. [Google Scholar]
- Meltzer, E.O.; Jalowayski, A.A. Nasal cytology in clinical practice. Am. J. Rhinol. 1988, 2, 47–54. [Google Scholar] [CrossRef]
- Spector, S.L.; Nicklas, R.A.; Chapman, J.A.; Bernstein, I.L.; Berger, W.E.; Blessing-Moore, J.; Dykewicz, M.S.; Fineman, S.M.; Lee, R.E.; James, T.; et al. Symptom severity assessment of allergic rhinitis: Part 1. Ann. Allergy Asthma Immunol. 2003, 91, 105–110. [Google Scholar] [CrossRef]
- Young, T.; Finn, L.; Kim, H.C. Nasal obstruction as a risk factor for sleep-disordered breathing. J. Allergy Clin. Immunol. 1997, 99, S757–S762. [Google Scholar] [CrossRef]
- Rappai, M.; Collop, N.; Kemp, S.; deShazo, R. The nose and sleep-disordered breathing: What we know and what we do not know. Chest 2003, 124, 2309–2323. [Google Scholar] [CrossRef] [Green Version]
- Abrishami, A.; Khajehdehi, A.; Chung, F. A systematic review of screening questionnaires for obstructive sleep apnea. Can. Anaesth 2010, 57, 423–438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, F.; Subramanyam, R.; Liao, P.; Sasaki, E.; Shapiro, C.; Sun, Y. High STOP-Bang indicates a high probability of obstructive sleep apnoea. BJA 2012, 108, 768–775. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johns, M.W. A new method for measuring daytime sleepiness: The Epworth sleepinees scale. Sleep 1991, 14, 540–545. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, Y.; Wu, S.; Zhang, L.; Yang, Y.; Cao, S.; Li, O. Association of Allergic Rhinitis With Obstructive Sleep Apnea: A Meta-Analysis. Medicine (Baltimore) 2018, 97, e13783. [Google Scholar] [CrossRef] [PubMed]
- Berry, R.B.; Brooks, R.; Gamaldo, S.M.; Harding, S.M.; Lloyd, R.M.; Marcus, C.L.; Vaughn, B.V. For the American Academy of Sleep Medicine. In The AASM Manual for the Scoring of Sleep: And Associated Events: Rules, Terminology and Technical Specifications, Version 2.3; American Academy of Sleep Medicine: Darien, IL, USA, 2017. [Google Scholar]
- Zheng, M.; Wang, X.; Zhang, L. Association between allergic and nonallergic rhinitis and obstructive sleep apnea. Curr. Opin. Allergy Clin. Immunol. 2018, 18, 16–25. [Google Scholar] [CrossRef]
- Blaiss, M.; Reigel, T.; Philpot, E. A study to determine the impact of rhinitis on sufferers’ sleep and daily routine [abstract]. J. Allergy Clin. Immunol. 2005, 115, S197. [Google Scholar] [CrossRef]
- Léger, D.; Annesi-Maesano, I.; Carat, F.; Rugina, M.; Chanal, I.; Pribil, C.; Abdelkader El Hasnaoui, M.D.; Bousquet, J. Allergic rhinitis and its consequences on quality of sleep: An unexplored area. Arch. Intern. Med. 2006, 166, 1744–1748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kramer, M.F.; De La Chaux, R.; Dreher, A.; Pfrogner, E.; Rasp, G. Allergic Rhinitis Does Not Constitute a Risk Factor for Obstructive Sleep Apnea Syndrome. Acta Otolaryngol. 2001, 121, 494–499. [Google Scholar] [CrossRef] [PubMed]
- Rubinstein, I. Nasal inflammation in patients with obstructive sleep apnea. Laryngoscope 1995, 105, 175–177. [Google Scholar] [CrossRef]
- Byun, M.K.; Park, S.C.; Chang, Y.S.; Kim, Y.S.; Kim, S.K.; Kim, H.J.; Chang, J.; Ahn, C.M.; Park, M.S. Association of moderate to severe asthma with obstructive sleep apnea. Yonsei Med. J. 2013, 54, 942–948. [Google Scholar] [CrossRef] [PubMed]
- Thornton, M.A.; Akasheh, N.; Walsh, M.T.; Moloney, M.; Sheahan, P.O.; Smyth, C.M.; Walsh, R.M.; Morgan, R.M.; Curran, D.R.; Walsh, M.T. Eosinophil recruitment to nasal nerves after allergen challenge in allergic rhinitis. Clin. Immunol. 2013, 147, 50–57. [Google Scholar] [CrossRef]
- Craig, T.J.; McCann, J.L.; Gurevich, F.; Davies, M.J. The correlation between allergic rhinitis and sleep disturbance. J. Allergy Clin. Immunol. 2004, 114, S139–S145. [Google Scholar] [CrossRef]
- Craig, T.J.; McCann, J.L.; Gurevich, F.; Davies, M.J. Mediators and cytokines in persistent allergic rhinitis and non-allergic rhinitis with eosinophilia syndrome. Int. Arch. Allergy Immunol. 2012, 159, 171–178. [Google Scholar]
- Makihara, S.; Okano, M.; Fujiwara, T.; Noda, Y.; Higaki, T.; Miyateke, T.; Kengo Kanai, M.D.; Takenori Haruna, M.D.; Shin Kariya, M.D.; Nishizaki, K. Local expression of interleukin-17a is correlated with nasal eosinophilia and clinical severity in allergic rhinitis. Allergy Rhinol. (Providence) 2014, 5, 22–27. [Google Scholar] [CrossRef]
- Krouse, H.J.; Davis, J.E.; Krouse, J.H. Immune mediators in allergic rhinitis and sleep. Otolaryngol. Head Neck Surg 2002, 126, 607–613. [Google Scholar] [CrossRef]
- Carpagnano, E.G.; Lacedonia, D.; Foschino-Barbaro, M.P. Non-invasive study of airways inflammation in sleep apnea patients. Sleep Med. Rev. 2011, 15, 317–326. [Google Scholar] [CrossRef]
- Mullington, J.M.; Hinze-Selch, D.; Pollmächer, T. Mediators of inflammation and their interaction with sleep. Relevance for chronic fatigue syndrome and related conditions. Ann. N. Y. Acad. Sci. 2001, 933, 201–206. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | Nares 20 pts | AR 20 pts | Controls 20 pts | p | p′ | p″ |
|---|---|---|---|---|---|---|
| Male % | 60 (12/20 pz) | 50 (10/20 pz) | 50 (10/20 pz) | 0.02 | 0.15 | 0.25 |
| Female % | 40 (8/20 pz) | 50 (10/20 pz) | 50 (10/20 pz) | 0.21 | 0.02 | 0.26 |
| Age, mean ± SD, y | 47.9 ± 11.3 | 45.8 ± 8.7 | 46.6 ± 7.8 | 0.4 | 0.35 | 0.35 |
| Height, mean ± SD, cm | 174.8 ± 3.2 | 173.3 ± 1.9 | 171 ± 2.25 | 0.25 | 0.69 | 0.75 |
| Weight, mean ± SD, Kg | 75.3 ± 4.3 | 72.5 ± 2.5 | 69.6 ± 3.8 | 0.62 | 0.42 | 0.9 |
| Gastroesophageal reflux disease, % | 15 (3/20 pz) | 10 (2/20 pz) | 10 (2/20 pz) | 0.9 | 0.38 | 0.04 |
| Smoker, % | 20 (4/20 pz) | 25 (5/20 pz) | 20 (4/20 pz) | 0.14 | 0.14 | 0.036 |
| BMI, mean ± SD, Kg/m2 | 23.8 ± 3 | 23.72 ± 2.1 | 23.6 ± 1.9 | 0.23 | 0.78 | 0.87 |
| Neck circumference, mean ± SD, cm | 40 ± 3 | 39 ± 2 | 38 ± 1.5 | 0.45 | 0.45 | 0.39 |
| NARES (n = 20) | AR (n = 20) | Controls (n = 20) | p | p′ | p″ | |
|---|---|---|---|---|---|---|
| Eosinophils (%) | 42.5 (35–48.5) | 5.6 (2.5–7.75) | 0 | 0 | <0.005 | <0.005 |
| NNNSS | ||||||
| Sneezing | 3 (1–4) | 3 (3–3) | 1 (1–1) | 0.020 | 0.0002 | 0.000005 |
| Congestion | 5 (5–6) | 4 (3–4) | 1 (1–1) | 0.001 | 0.0035 | 0.00009 |
| Rhinorrhea | 3 (3–4) | 3 (2–4) | 1 (1–1) | 0.025 | 0.0005 | 0.00066 |
| Itchy nose | 2 (1–2.25) | 3 (2–3.75) | 1 (1–1) | 0.001 | 0.0004 | 0.00114 |
| Postnasal drip | 1 (1–1.25) | 1 (1–2) | 1 (1–1) | 0.01 | 0.021 | 0.038 |
| Throat symptom | 2 (1.75–2) | 2 (1–2) | 1 (1–1) | 0.026 | 0.0015 | 0.00078 |
| Chronic cough | 3 (2–4) | 2 (2–2) | 1 (1–1) | 0.001 | 0.0006 | 0.0005 |
| Headache | 2 (1–3) | 2 (1–2) | 1 (1–1) | 0.07 | 0.0004 | 0.0003 |
| ESS | 14.5 (12.25–18.25) | 10.5 (7.5–13.5) | 4 (1–5) | 0.0006 | 0.002 | 0.0026 |
| STOP-BANG | 6 (5–7) | 4 (3.75–5.25) | 1 (0–1) | 0.004 | 0.0004 | 0.041 |
| NARES | AR | CONTROL | p | p′ | p″ | ||||
|---|---|---|---|---|---|---|---|---|---|
| n° | % | n° | % | n° | % | ||||
| NO-OSA | 8/20 | 40 | 13 | 60 | 18 | 90 | 0.0004 | 0.05 | |
| OSA | 12/20 | 60 | 7/20 | 35 | 2/20 | 10 | 0.05 | ||
| MILD OSA | 5/12 | 42 | 4/7 | 57 | 1/2 | 50 | 0.6 | 1 | 1 |
| MODERATE OSA | 3/12 | 25 | 1/7 | 14 | 1/2 | 50 | 1 | 0.4 | 0.5 |
| SEVERE OSA | 4/12 | 33 | 2/7 | 29 | / | / | 1 | 1 | 1 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pace, A.; Iannella, G.; Rossetti, V.; Visconti, I.C.; Gulotta, G.; Cavaliere, C.; De Vito, A.; Maniaci, A.; Cocuzza, S.; Magliulo, G.; et al. Diagnosis of Obstructive Sleep Apnea in Patients with Allergic and Non-Allergic Rhinitis. Medicina 2020, 56, 454. https://doi.org/10.3390/medicina56090454
Pace A, Iannella G, Rossetti V, Visconti IC, Gulotta G, Cavaliere C, De Vito A, Maniaci A, Cocuzza S, Magliulo G, et al. Diagnosis of Obstructive Sleep Apnea in Patients with Allergic and Non-Allergic Rhinitis. Medicina. 2020; 56(9):454. https://doi.org/10.3390/medicina56090454
Chicago/Turabian StylePace, Annalisa, Giannicola Iannella, Valeria Rossetti, Irene Claudia Visconti, Giampiero Gulotta, Carlo Cavaliere, Andrea De Vito, Antonino Maniaci, Salvatore Cocuzza, Giuseppe Magliulo, and et al. 2020. "Diagnosis of Obstructive Sleep Apnea in Patients with Allergic and Non-Allergic Rhinitis" Medicina 56, no. 9: 454. https://doi.org/10.3390/medicina56090454