
Antibacterial Activity of Essential Oils and Their Isolated Constituents against Cariogenic Bacteria: A Systematic Review

 and
and
Abstract
:
1. Introduction
2. Results

2.1. In Vitro Studies
2.1.1. Planktonic Studies
Crude EOs and Planktonic S. mutans

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Plant Species | Source | Microorganism | MIC (µg/mL) | MBC (µg/mL) | Score | Ref. |
|---|---|---|---|---|---|---|
| Achillea ligustica All. | Inflorescences | DSM 20523 | 155 | nt | +++ | [19] |
| Achillea ligustica All. | Leaves | DSM 20523 | 155 | nt | +++ | [19] |
| Achillea ligustica All. | flowering aerial parts | DSM 20523 | 38 | nt | ++++ | [19] |
| Achillea ligustica All. | Flowers | DSM 20523 | 155 | 310 | +++ | [22] |
| Achillea ligustica All. | vegetative parts | DSM 20523 | 39 | 39 | ++++ | [22] |
| Ageratum conyzoides | Leaves | ATCC 25175 | 4000 | nt | − | [23] |
| Aloysia gratissima | Leaves | UA 159 | 125–250 | 250–500 | +++ | [11] |
| Aloysia triphylla | Leaves | UA 159 | 125–250 | 125–250 | +++ | [11] |
| Alpinia speciosa | Root | UA 159 | 125–250 | 250–500 | +++ | [11] |
| Artemisia camphorata Vill. | Leaves | ATCC 25175 | 2000 | nt | + | [23] |
| Baccharis dracunculifolia | Leaves | UA 159 | 62.5–125 | 250–500 | ++++ | [11] |
| Bidens sulphurea | Leaves | ATCC 25175 | 250 | nt | +++ | [23] |
| Cinnamomum zeylanicum | Leaves | UA 159 | 250–500 | 500–1000 | +++ | [11] |
| Coriandrum sativum | Leaves | UA 159 | 31.2–62.5 | 62.5–125 | ++++ | [11] |
| Croton cajucara Benth | Leaves | ATCC 4646 | 40.1 | 13.8 | ++++ | [21] |
| Cryptomeria japonica | aerial parts | ATCC 25175 | 100 | 200 | ++++ | [20] |
| Cuminum cyminum | CS | PTCC 1601 | 4000 | nt | − | [24] |
| Cymbopogon citratus | Leaves | UA 159 | 125–250 | 250–500 | +++ | [11] |
| Cymbopogon martini | leaves | UA 159 | 125–250 | 250–500 | +++ | [11] |
| Cymbopogon winterianus | Leaves | UA 159 | 125–250 | 250–500 | +++ | [11] |
| Cyperus articulatus | Bulbs | UA 159 | 125–250 | 250–500 | +++ | [11] |
| Elyonurus muticus | Leaves | UA 159 | 125–250 | 250–500 | +++ | [11] |
| Eucalyptus radiate | CS | JC-2 | 10,000 | 10,000 | − | [25] |
| Eugenia caryophyllata L. | CS | ATCC 25175 | 200 | 800 | +++ | [26] |
| Eugenia caryophyllata L. | CS | ATCC 5175 | 600 | nt | ++ | [27] |
| Eugenia florida | Leaves | UA 159 | 125–250 | 125–250 | +++ | [11] |
| Eugenia uniflora | Leaves | UA 159 | 125–250 | 250–500 | +++ | [11] |
| Foeniculum vulgare Mill. | Leaves | ATCC 25175 | >4000 | nt | − | [23] |
| Lavandula officinalis | CS | JC-2 | >10,000 | >10,000 | − | [25] |
| Leptosperfum scoparium | CS | JC-2 | 2500 | 2500 | − | [25] |
| Lippia alba | Leaves | ATCC 25175 | 500 | nt | +++ | [23] |
| Lippia alba | Leaves | UA 159 | 125–250 | 250–500 | +++ | [11] |
| Lippia sidoides | Leaves | UA 159 | 62.5–125 | 125–250 | ++++ | [11] |
| Melaleuca alternifólia | CS | JC-2 | 10,000 | 10,000 | − | [25] |
| Melaleuca alternifólia | Leaves | clinical isolates | 0.25–2 | 0.25–2 | * | [28] |
| Mentha piperita | Leaves | UA159 | 250–500 | 250–500 | +++ | [11] |
| Mentha piperita | CS | PTCC 1601 | 6000 | nt | + | [24] |
| Mikania glomerata | Leaves | UA 159 | 62.5–125 | 125–250 | ++++ | [11] |
| Ocimum americanum L. | Leaves | ATCC 6363 | 0.04 | 0.08 | * | [29] |
| Ocimum gratissimum L. | Leaves | ATCC 25175 | 1000 | nt | ++ | [23] |
| Pelargonium graveolens | Leaves | ATCC 25175 | 1000 | nt | ++ | [23] |
| Romarinus officinalis L. | Leaves | JC-2 | >10,000 | >10,000 | − | [25] |
| Rosmarinus officinalis L. | Leaves | ATCC 25275 | >2000 | nt | − | [15] |
| Rosmarinus officinalis L. | CS | PTCC 1601 | 2000 | nt | − | [30] |
| Satureja biflora | flowering aerial parts | clinical isolates | 640 | nt | ++ | [31] |
| Satureja masukensis | flowering aerial parts | clinical isolates | 570 | nt | ++ | [31] |
| Satureja pseudosimensis | Leaves and flowering tops | clinical isolates | 920 | nt | ++ | [31] |
| Siparuna guianenses | Leaves | UA 159 | 62.5–125 | 125–250 | ++++ | [11] |
| Syzygium aromaticum | Leaves | ATCC 25175 | 2000 | nt | + | [23] |
| Syzygium aromaticum | Leaves | UA 159 | 250–500 | 250–500 | +++ | [11] |
| Tagetes erecta L. | Leaves | ATCC 25175 | >4000 | nt | − | [23] |
| Thymus eriocalyx | CS | PTCC 1601 | 2000 | nt | + | [30] |
| Zivuphus zoazeiro | Leaves | UA 159 | 250–500 | 500–1000 | +++ | [11] |
Crude EOs and Planktonic S. sobrinus, S. sanguinis and S. salivarius
Crude EOs and Planktonic Lactobacilli
EO-Isolated Compounds against Streptococci and Lactobacilli
| Plant Species | Source | Microorg | S. sobrinus 1 | S. sanguinis 2 | S. salivarius 3 | Ref. | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MIC (µg/mL) | MBC (µg/mL) | Score | MIC (µg/mL) | MBC (µg/mL) | Score | MIC (µg/mL) | MBC (µg/mL) | Score | ||||
| Achillea ligustica All | inflorescences | IMC104 3 | nt | nt | nt | nt | 1250 | nt | + | [19] | ||
| Achillea ligustica All | Leaves | IMC104 3 | nt | nt | nt | nt | 1250 | nt | + | [19] | ||
| Achillea ligustica All | flowering aerial parts | IMC104 3 | nt | nt | nt | nt | 625 | nt | ++ | [19] | ||
| Ageratum conyzoides L. | Leaves | ATCC 33478 1 | >4000 | nt | − | >4000 | nt | − | 4000 | nt | − | [23] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| Artemisia camphorata Vill. | Leaves | ATCC 33478 1 | 2000 | nt | + | 2000 | nt | + | 4000 | nt | − | [23] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| Bidens sulphurea | Leaves | ATCC 33478 1 | 4000 | nt | − | 4000 | nt | − | 4000 | nt | − | [23] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| Croton cajucara Benth | Leaves | ATCC 27609 1 | 13.8 | nt | ++++ | nt | nt | nt | nt | [21] | ||
| Cryptomeria japonica | aerial parts | ATCC 27607 1 | 100 | 100 | ++++ | 100 | 200 | ++++ | nt | nt | [20] | |
| ATCC 10556 2 | ||||||||||||
| Eucalyptus radiate | CS | ATCC 6715 1 | 10,000 | 10,000 | − | nt | nt | nt | nt | [25] | ||
| ATCC B13 1 | ||||||||||||
| Eugenia caryophyllata L. | Flowers | ATCC 27607 1 | 200 | 800 | +++ | 400 | 800 | +++ | nt | nt | [26] | |
| ATCC 10556 2 | ||||||||||||
| Foeniculum vulgare Mill. | Leaves | ATCC 33478 1 | >4000 | nt | − | >4000 | nt | − | >4000 | nt | − | [23] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| Lavandula officinalis | CS | 6715 1 B13 1 | 10,000 10,000 | 10,000 10,000 | − − | nt | nt | nt | nt | [25] | ||
| Leptosperfum scoparium | CS | 6715 1 B13 1 | 1300 2500 | 2500 2500 | + − | nt | nt | nt | nt | [25] | ||
| Lippia alba | Leaves | ATCC 33478 1 | 1000 | nt | ++ | 1000 | nt | ++ | 2000 | nt | + | [23] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| Melaleuca alternifólia | CS | 6715 1 B13 1 | 10,000 2500 | 10,000 10,000 | − − | nt | nt | nt | nt | [25] | ||
| Mentha piperita | CS | Ssb 176 1 | 3000 | nt | − | 6000 | nt | − | nt | nt | [32] | |
| Ssg 009 2 | ||||||||||||
| Ocimum basilicum | CS | Ssb 176 1 | 6000 | nt | − | 6000 | nt | − | nt | nt | [32] | |
| Ssg 009 2 | ||||||||||||
| Ocimum gratissimum L. | Leaves | ATCC 33478 1 | 1000 | nt | ++ | 2000 | nt | + | 2000 | nt | + | [23] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| Pelargonium graveolens | Leaves | ATCC 33478 1 | 1000 | nt | ++ | 2000 | nt | + | 2000 | nt | + | [23] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| Rosmarinus officinalis L. | Leaves | 6715 1 | 10,000 10,000 | 10,000 10,000 | − − | nt | nt | nt | nt | [25] | ||
| B13 1 | ||||||||||||
| Rosmarinus officinalis L. | Leaves | ATCC 33478 1 | 500 | nt | +++ | >2000 | nt | − | 600 | nt | ++ | [15] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| Salvia officinalis | CS | Ssb 176 1 | 3000 | nt | − | 6000 | nt | − | nt | nt | [32] | |
| Ssg 009 2 | ||||||||||||
| Syzygium aromaticum | Leaves | ATCC 33478 1 | >4000 | nt | − | >4000 | nt | − | >4000 | nt | − | [23] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| Tagetes erecta L. | Leaves | Ssb 176 1 | 6000 | nt | − | nt | nt | nt | nt | [32] | ||
| Ssg 009 2 | ||||||||||||
| Plant Species | Source | Microorg | L. acidophilus 1 | L. casei 2 | Ref. | ||||
|---|---|---|---|---|---|---|---|---|---|
| MIC (µg/mL) | MBC (µg/mL) | Score | MIC (µg/mL) | MBC (µg/mL) | Score | ||||
| Achillea ligustica All. | Inflorescences | IMC 101 1 | 310 | nt | +++ | nt | nt | [19] | |
| Achillea ligustica All. | Leaves | IMC 101 1 | 2500 | nt | − | nt | nt | [19] | |
| Achillea ligustica All. | flowering aerial parts | IMC 101 1 | 1250 | nt | + | nt | nt | [19] | |
| Ageratum conyzoides L. | Leaves | ATCC 11578 2 | nt | nt | 4000 | nt | - | [23] | |
| Artemisia camphorata Vill. | Leaves | ATCC 11578 2 | nt | nt | 500 | nt | +++ | [23] | |
| Bidens sulphurea | Leaves | ATCC 11578 2 | nt | nt | 500 | nt | +++ | [23] | |
| Croton cajucara Benth | Leaves | ATCC 4646 2 | nt | nt | 22.3 | nt | ++++ | [21] | |
| Foeniculum vulgare Mill. | Leaves | ATCC 11578 2 | nt | nt | 4000 | nt | − | [23] | |
| Lippia alba | Leaves | ATCC 11578 2 | nt | nt | 500 | nt | +++ | [23] | |
| Ocimum americanum L. | Leaves | ATCC 6363 2 | nt | nt | 0.04 | 0.3 * | * | [29] | |
| Ocimum basilicum | aerial parts | ATCC 4356 1 | 80,000 | nt | − | nt | nt | [33] | |
| Ocimum gratissimum L. | Leaves | ATCC 11578 2 | nt | nt | 500 | nt | +++ | [23] | |
| Origanum vulgare | aerial parts | ATCC 4356 1 | 5000 | nt | − | nt | nt | [33] | |
| Pelargonium graveolens | Leaves | ATCC 11578 2 | nt | nt | 1000 | nt | ++ | [23] | |
| Rosmarinus officinalis | aerial parts | ATCC 4356 1 | 80,000 | nt | − | nt | nt | [33] | |
| Salvia officinalis | aerial parts | ATCC 4356 1 | 80,000 | nt | − | nt | nt | [33] | |
| Syzygium aromaticum | Leaves | ATCC 11578 2 | nt | nt | 1000 | nt | ++ | [23] | |
| Tagetes erecta L. | Leaves | ATCC 11578 2 | nt | nt | 4000 | nt | − | [23] | |
| Thymus vulgaris | aerial parts | ATCC 4356 1 | 5000 | nt | − | nt | nt | [33] | |
| Compound | Plant Species | Culture Collection | MIC (μg/mL) | MBC (μg/mL) | Score | Ref. |
|---|---|---|---|---|---|---|
| 1,8, Cineole | Achillea ligustica All | DSM 20523 | 2500 | nt | − | [19] |
| 1,8, Cineole | Achillea ligustica All | DSM 20523 | 155 | 1250 | +++ | [22] |
| 1,8, Cineole | Rosmarinus officinalis | ATCC 25275 | 1500 | nt | + | [15] |
| Camphor | Rosmarinus officinalis | ATCC 25275 | 1500 | nt | + | [15] |
| Caryophyllene oxide | Satureja species | clinical isolates | 250 | nt | +++ | [31] |
| Eugenol | Eugenia caryophyllata L. | ATCC 25175 | 100 | 200 | ++++ | [26] |
| Linalool | Achillea ligustica All | DSM 20523 | 625 | nt | ++ | [19] |
| Linalool | Achillea ligustica All | DSM 20523 | 310 | 310 | +++ | [22] |
| Linalool | Croton cajucara Benth | ATCC 25175 | no activity | nt | − | [21] |
| Linalool | Satureja species | clinical isolates | 370 | nt | +++ | [31] |
| Menthol | Mentha longifolia L. | clinical isolates | 15.6 | nt | ++++ | [34] |
| Pulegone | Satureja species | clinical isolates | 1750 | nt | + | [31] |
| Sabinene | Cryptomeria japonica | ATCC 25175 | 800 | 1600 | ++ | [20] |
| Terpinen-4-ol | Achillea ligustica All | DSM 20523 | 1250 | nt | + | [19] |
| Terpinen-4-ol | Achillea ligustica All | DSM 20523 | 310 | 625 | +++ | [22] |
| Terpinen-4-ol | Cryptomeria japonica | ATCC 25175 | 1600 | 3200 | + | [20] |
| Verbenone | Rosmarinus officinalis | ATCC 25275 | 1000 | nt | ++ | [15] |
| Viridiflorol | Achillea ligustica All | DSM 20523 | 2500 | nt | − | [19] |
| α-Pinene | Cryptomeria japonica | ATCC 25175 | 6400 | 28,000 | − | [20] |
| α-Pinene | Rosmarinus officinalis | ATCC 25275 | 2000 | nt | + | [15] |
| α-Terpineol | Cryptomeria japonica | ATCC 25175 | 1600 | 3200 | + | [20] |
| β-Caryophyllene | Eugenia caryophyllata L. | ATCC 25175 | 1600 | 3200 | + | [26] |
| β-Caryophyllene | Rosmarinus officinalis | ATCC 25275 | 300 | nt | +++ | [15] |
| β-Myrcene | Rosmarinus officinalis | ATCC 25275 | 400 | nt | +++ | [15] |
| β-Pinene | Achillea ligustica All | DSM 20523 | 1250 | nt | + | [19] |
| β-Pinene | Achillea ligustica All | DSM 20523 | 625 | 1250 | ++ | [22] |
| γ-Terpinene | Achillea ligustica All | DSM 20523 | 2500 | nt | − | [19] |
| Compound | Source | Culture Collection | L. acidophilus 1 | L. casei 2 | Ref. | ||||
|---|---|---|---|---|---|---|---|---|---|
| MIC (µg/mL) | MBC (µg/mL) | Score | MIC (µg/mL) | MBC (µg/mL) | Score | ||||
| 1,8, Cineole * | Achillea ligustica All | IMC101 1 | 5000 | nt | − | nt | nt | [19] | |
| Linalool | Croton cajucara Benth | ATCC 4646 2 | nt | nt | no activity | nt | − | [21] | |
| Linalool * | Achillea ligustica All | IMC101 1 | 5000 | nt | − | nt | nt | [19] | |
| Menthol | Mentha longifolia L. | clinical isolates | 31.2 | nt | ++++ | nt | nt | [34] | |
| Terpinen-4-ol * | Achillea ligustica All | IMC101 1 | 5000 | nt | − | nt | nt | [19] | |
| β-Pinene * | Achillea ligustica All | IMC101 1 | 2500 | nt | − | nt | nt | [19] | |
| γ-Terpinene * | Achillea ligustica All | IMC101 1 | 5000 | nt | − | nt | nt | [19] | |
| Compound | Plant Species | Culture Collection | S. sobrinus 1 | S. sanguinis 2 | S. salivarius 3 | Ref. | ||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| MIC (µg/mL) | MBC (µg/mL) | Score | MIC (µg/mL) | MBC (µg/mL) | Score | MIC (µg/mL) | MBC (µg/mL) | Score | ||||
| 1,8-cineole | Achillea ligustica All | IMC104 3 | nt | nt | nt | nt | 1250 | nt | + | [19] | ||
| Camphor | Rosmarinus officinalis | ATCC 33478 1 | 1500 | nt | + | 400 | nt | +++ | 400 | nt | +++ | [15] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| Eugenol | Eugenia caryophyllata L. | ATCC 27607 1 | 200 | 400 | +++ | 400 | 800 | +++ | nt | nt | [26] | |
| ATCC 10556 2 | ||||||||||||
| Linalool | Achillea ligustica All | IMC104 3 | nt | nt | nt | nt | 625 | nt | ++ | [19] | ||
| Linalool | Croton cajucara Benth | ATCC 27609 1 | no activity | nt | − | nt | nt | nt | nt | [21] | ||
| Sabinene | Cryptomeria japonica | ATCC 27607 1 ATCC 10556 2 | 200 | 200 | +++ | 400 | 400 | +++ | nt | nt | [20] | |
| Terpinen-4-ol | Achillea ligustica All | IMC104 3 | nt | nt | nt | nt | 625 | nt | ++ | [19] | ||
| Terpinen-4-ol | Cryptomeria japônica | ATCC 27607 1 | 1600 | 3200 | + | 1600 | 3200 | + | nt | nt | [20] | |
| ATCC 10556 2 | ||||||||||||
| Verbenone | Rosmarinus officinalis | ATCC 33478 1 | 1000 | nt | ++ | 400 | nt | +++ | 400 | nt | +++ | [15] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| Viridiflorol | Achillea ligustica All | IMC104 3 | nt | nt | nt | nt | 625 | nt | ++ | [19] | ||
| α-Pinene | Cryptomeria japonica | ATCC 27607 1 | 6400 | 12.800 | − | 6400 | 6400 | - | nt | nt | [20] | |
| ATCC 10556 2 | ||||||||||||
| α-Pinene | Rosmarinus officinalis | ATCC 33478 1 | 1000 | nt | ++ | 400 | nt | +++ | 400 | nt | +++ | [15] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| α-Terpineol | Cryptomeria japônica | ATCC 27607 1 | 1600 | 1600 | + | 1600 | 3200 | + | nt | nt | [20] | |
| ATCC 10556 2 | ||||||||||||
| β-Caryophyllene | Eugenia caryophyllata L. | ATCC 27607 1 | 12,800 | 12,800 | − | 1600 | 3200 | + | nt | nt | [26] | |
| ATCC 10556 2 | ||||||||||||
| β-Caryophyllene | Rosmarinus officinalis | ATCC 33478 1 | 400 | nt | +++ | 400 | nt | +++ | 400 | nt | +++ | [15] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| β-Myrcene | Rosmarinus officinalis | ATCC 33478 1 | 1500 | nt | + | 1500 | nt | + | 400 | nt | +++ | [15] |
| ATCC 10556 2 | ||||||||||||
| ATCC 25975 3 | ||||||||||||
| β-Pinene | Achillea ligustica All | IMC104 3 | nt | nt | nt | nt | 625 | nt | ++ | [19] | ||
| γ-Terpinene | Achillea ligustica All | IMC104 3 | nt | nt | nt | nt | 625 | nt | ++ | [19] | ||
2.1.2. Biofilm Studies
Crude EOs and Biofilms of Streptococci and Lactobacilli
2.2. In Vivo Studies
Randomized Clinical Trials
2.3. Chemical and Botanical Characterization and Georeferencing of the most Promising Bioactive EOs
| Ref. | Essential Oil/Fraction or Isolated Compound | Biofilm Formation | |||
|---|---|---|---|---|---|
| Strain | Test(s) Performed | Biofilm Age Conditions | Outcomes | ||
| [11] | Aloysia gratíssima (Ag), Coriandrum sativum (Cs) and Baccharis dracunculifolia (Bd) fraction | S. mutans UA159 | Formation of S. mutans biofilm, the samples were placed in the wells of sterile polystyrene U-bottom microtiter plates, previously treated with saliva | S. mutans cells (1.0 × 107 cells/mL in BHI medium) were added to wells containing BHI medium with 2% sucrose and the samples were incubated at 37 °C for 18 h | Biofilm of Cs4 and Bd2 fractions presented a better performance since they inhibited more than 90% of biofilm formation at lower concentrations (31.2 μg/mL). |
| [21] | Croton cajucara Benth leaves | S. mutans ATCC 25175 | Macro technique using microbial disks subjected to the action of the essential oil and controls | The biofilms were exposed to controls and essential oil for 3 min and incubated for 72 h at 37 °C | Growth inhibition: EO 70%–75% Chlorhexidine 65%–70% |
| [21] | Croton cajucara Benth leaves | S. sobrinus ATCC 27609 | Macro technique using microbial disks subjected to the action of the essential oil and controls | The biofilms were exposed to controls and essential oil for 3 min and incubated for 72 h at 37 °C | Growth inhibition: EO 75%–80% Chlorhexidine 50%–55% |
| [21] | Croton cajucara Benth leaves | L. casei ATCC 4646 | Macro technique using microbial disks subjected to the action of the essential oil and controls | The biofilms were exposed to controls and essential oil for 3 min and incubated for 72 h at 37 °C | Growth inhibition: EO 80%–85% Chlorhexidine 65%–70% |
| [38] | Curcuma longa root | S. mutans ATCC 25175 | Technique using 24-well plates containing resin teeth. | After cultivating S. mutans for 24 h at 37 °C, the supernatant was removed, and the wells were rinsed with distilled H2O. Biofilm formation in the wells was measured by staining with 0.1% safranin | Biofilm formation was decreased in the presence of C. longa essential oil at concentrations higher than 500 µg/mL |
| [39] | Mentha piperita and Rosmarinus officinalis | S. mutans PTCC 1601 | Biofilm formation (SBF) assay | The biofilms were exposed to controls and essential oil and incubated for 17 ± 1 h at 37 °C | M. piperita and R. officinalis oils effectively inhibited S. mutans biofilm at 6000 and 2000 ppm, respectively. |
| [29] | Ocimum americanum L. leaves | S. mutans KPSK2 | Microtiter technique Protocol using saliva. | The biofilms were exposed to controls and essential oil (0.3% and 3% v/v) for 5 min and incubated for 24 h | EO 0.3% (v/v) 7.2 × 104 CFU/mL; EO 3% (v/v) 2.9 × 103 CFU/mL; 0.2% Chlorhexidine: 1.7 × 103 CFU/mL; Saline solution 8.5.106 CFU/mL |
| [29] | Ocimum americanum L. leaves | L. casei ATCC 6363 | Microtiter technique Protocol using saliva. | The biofilms were exposed to controls and essential oil (0.3% and 3% v/v) for 5 min and incubated for 24 h | EO 0.3% (v/v) 5.1 × 105 CFU/mL; EO 3% (v/v) 6.3 × 103 CFU/mL; 0.2% Chlorhexidine: 2.5 × 103 CFU/mL; Saline solution 6.0 × 106 CFU/mL |
| Plant Species or Chemical Constituent | Antibacterial Efficacy | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Planktonic Cells | Biofilms | Clinical Trial | |||||||||
| Smu | Ssob | Ssan | Ssal | Lc | La | Smu | Ssob | Ssal | Lc | ||
| A. ligustica | + | ||||||||||
| B. dracunculifolia | + | ||||||||||
| C. cajucara | + | + | + | + | + | + | |||||
| C. japonica | + | + | + | ||||||||
| C. sativum | + | ||||||||||
| E. caryophyllata | + | + | + | ||||||||
| L. sidoides | + | Plaque reduction | |||||||||
| O. americanum | + | + | + | + | |||||||
| Menthol | + | + | |||||||||
| Eugenol | + | + | + | ||||||||

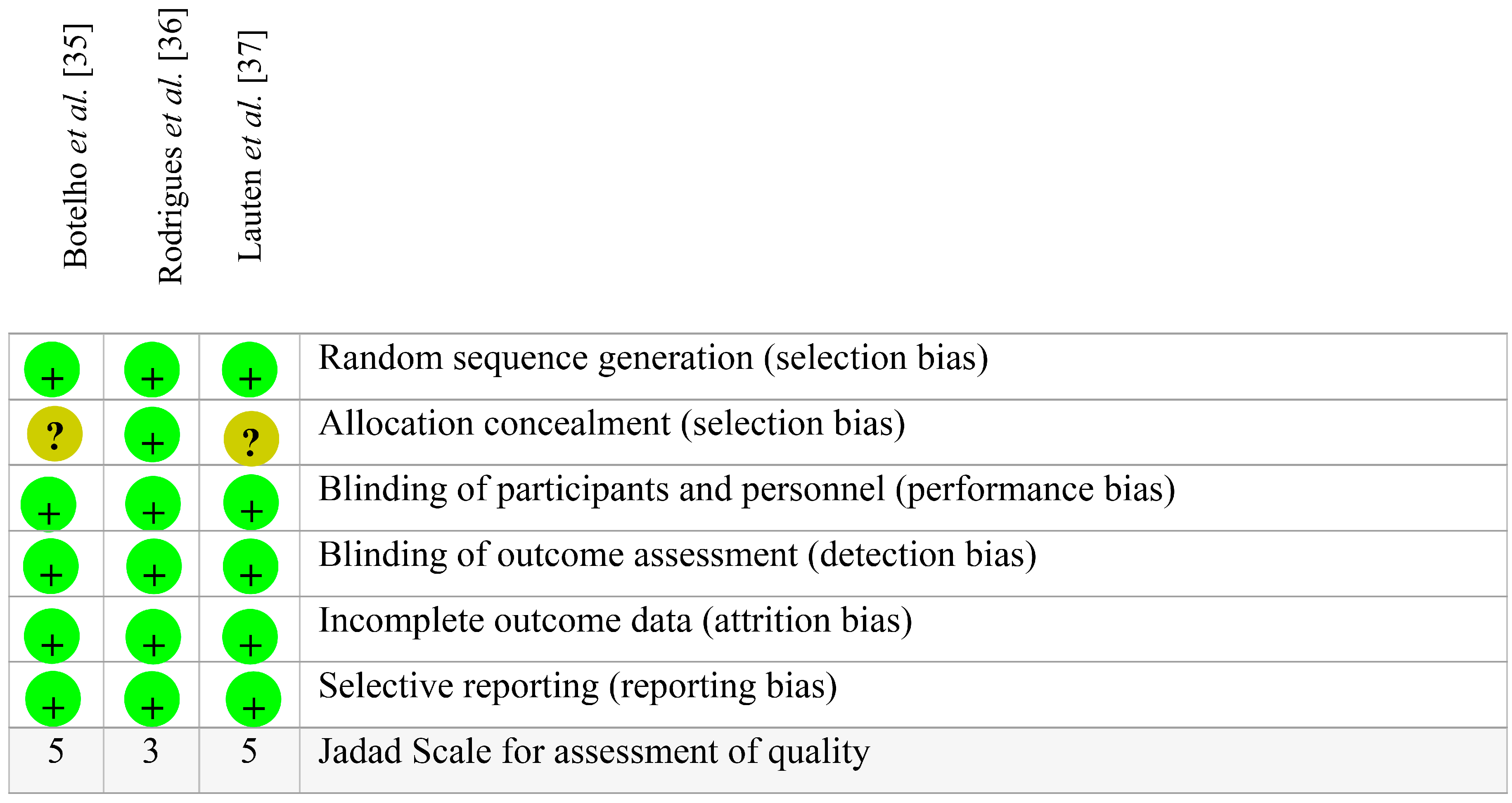
| Plant Species | Essential Oil Formulation | Study Design | Sample Size | Country | Age (Mean ± SD)/Gender (Fem) * | Sample Loss/Reasons | Control Group | Dosing Protocol | Assessment Checkpoints | Assessment Instruments of Interest | Outcome ** | Ref. |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Lipia sidoides | 1% L. sidoides mouthrinse | Phase II, randomized, double-blind, crossover | n = 55 (n = 27 L. sidoides group; n = 28 control group) | Brazil | 31 ± 10.90 55.6% F | 16 individuals (no gender distinction)/lack of compliance or could not be reached for follow-up visits. | 0.12% CHX | Rinsing approx. 15 mL for 30 s, twice a day (once after breakfast and once in the late afternoon) during a 7-day period. | Baseline, 1 week | Plaque index (PI) measured at four sites per tooth (Ainamo & Bay, 1975) | +/+ | [35] |
| Lipia sidoides | 10% L. sidoides gel | Phase II, randomized, double-blind, crossover. Partial mouth experimental model | n = 26 (n = 13 L. sidoides group; n = 13 control group) | Brazil | 22 ± 4.24 50.0% F | 4 individuals (no gender distinction)/third molar extraction | Placebo gel | Filling a toothshield with the gel prior to insertion in the mouth and seating it over the experimental teeth 3 times a day for at least 1 min. | Baseline, 3 weeks | Plaque index (PI) measured at six sites per tooth (Turesky et al., 1970) | −/+ | [36] |
| Melaleuca alternifolia, Leptospermum scoparium, Calendula officinalis and Camellia sinensis | Multi-herbal mouthrinse containing 0.67% (v/v) M. alternifolia oil, 0.33% (v/v) M. scoparium oil, 1% (v/v) C. officinalis flower extract (1:2) liquid extract [90% E/W]), 0.5% (w/v) C. sinensis extract (dry extract, 80% polyphenols) and 12.8% ethanol in water. | Phase I and II, randomized, double-blind | Phase I n = 8 (experimental group) Phase II n = 20 (n = 10 experim. group; n = 10 control group) | USA | 31.88 ± 7.51 Phase I: 62.5% F Phase II: 82.3% F | Phase I: 1 female/reported mild ‘hay fever’-like symptoms. Her symptoms were judged to be unrelated to the mouthrinse. Phase II: 3 female/One reported lightheadedness (possibly related to the test rinse); One dropped out to participate in another study; and one was excluded because she required treatment with antibiotics for an unrelated condition. | Placebo mouth rinse | Rinsing approx. 15 mL for 30 s, twice a day during a 6-week period. | Baseline, 6 weeks and 12 weeks | Plaque index (PI) measured at six sites per tooth (Quigley & Hein, 1962) | −/− | [37] |
3. Discussion
3.1. Promising Essential Oils against Cariogenic Bacteria
3.2. Promising Compounds Isolated from Essential Oils against Cariogenic Bacteria


3.3. Rational Clinical Use of Essential Oils and Isolated Compounds
4. Methods
4.1. Focused Question
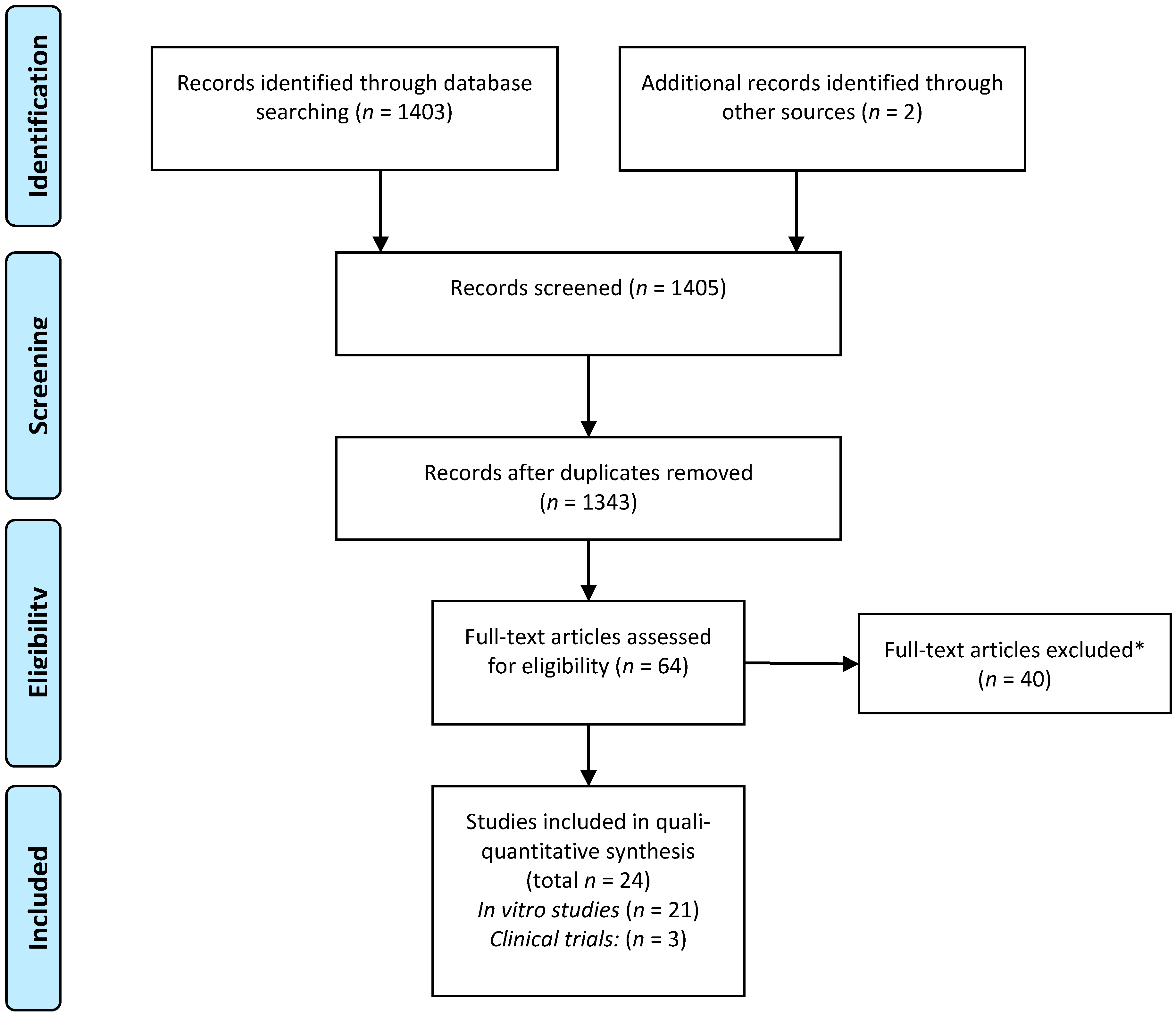
4.2. Search Strategy and Selection of the Studies
| Bibliographic Databases (Primary Sources) | Search Strategy (Descriptors and Boolean Operators) |
|---|---|
| SciVerse Scopus (Since 1995 until December 2014) |
|
| Web of Science (Refine: article or review) (Since 1990 until December 2014) |
|
| Medline via Pubmed (Since 1966 until December 2014) |
|
| SciELO (Scientific Electronic Library Online) (Since 1998 until December 2014) and LILACS (Latin American and Caribbean Health Sciences Literature) (Since 1982 until December 2014) |
|
| Cochrane Library |
|
| Google Scholar |
|
4.3. Eligibility Criteria
4.4. Data Pooling and Analysis
| MIC Range | Intensity of Antibacterial Activity | Score |
|---|---|---|
| ≤100 µg/mL | very strong activity | (++++) |
| 101–500 µg/mL | strong activity | (+++) |
| 501–1000 µg/mL | moderate activity | (++) |
| 1001–2000 µg/mL | weak activity | (+) |
| >2001 µg/mL | no activity | (−) |
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- National Institute of Health Consensus Development Panel; National Institutes of Health Consensus Development Conference statement. Diagnosis and management of dental caries throughout life. In J. Am. Dent. Assoc.; 2001; 132, pp. 1153–1161. [Google Scholar]
- Bagramian, R.A.; Garcia-Godoy, F.; Volpe, A.R. The global increase in dental caries. A pending public health crisis. Am. J. Dent. 2009, 22, 3–8. [Google Scholar] [PubMed]
- Bönecker, M.; Tenuta, L.M.; Pucca Junior, G.A.; Costa, P.B.; Pitts, N. A social movement to reduce caries prevalence in the world. Braz. Oral Res. 2013, 27, 5–6. [Google Scholar] [CrossRef] [PubMed]
- Gunsolley, J.C. Clinical efficacy of antimicrobial mouthrinses. J. Dent. 2010, 38, S6–S10. [Google Scholar] [CrossRef]
- Maguire, A. ADA clinical recommendations on topical fluoride for caries prevention. Evid. Based Dent. 2014, 15, 38–39. [Google Scholar] [CrossRef] [PubMed]
- Yévenes, I.; Alvarez, S.R.; Jara, M.N.; Wolfenson, P.M.; Smith, L.P. Comparison of mouthrinses containing chlorhexidine and other active agents with chlorhexidine mouthrinse-gel: Effects on de novo formation. J. Dent. Sci. 2009, 24, 345–348. [Google Scholar]
- Samuels, N.; Grbic, J.T.; Saffer, A.J.; Wexler, I.D.; Williams, R.C. Effect of an herbal mouth rinse in preventing periodontal inflammation in an experimental gingivitis model: A pilot study. Compend. Contin. Educ. Dent. 2012, 33, 204–206, 208–211. [Google Scholar] [PubMed]
- Jeon, J.G.; Rosalen, P.L.; Falsetta, M.L.; Koo, H. Natural products in caries research: Current (limited) knowledge, challenges and future perspective. Caries Res. 2011, 45, 243–263. [Google Scholar]
- Magee, P. Antiseptic drugs and disinfectants. Side Eff. Drugs Annu. 2007, 29, 241–243. [Google Scholar]
- Bassolé, I.H.; Juliani, H.R. Essential oils in combination and their antimicrobial properties. Molecules 2012, 17, 3989–4006. [Google Scholar] [CrossRef] [PubMed]
- Galvão, L.C.C.; Furletti, V.F.; Bersan, S.M.F.; Cunha, M.G.; Ruiz, A.L.T.G.; Carvalho, J.E.; Sartoratto, A.; Rehder, V.L.G.; Figueira, G.M.; Duarte, M.C.T.; et al. Antimicrobial Activity of Essential Oils against Streptococcus mutans and their Antiproliferative Effects. Evid. Based Complement. Altern. Med. 2012, 12, 751435. [Google Scholar]
- Bakkali, F.; Averbeck, S.; Averbeck, D.; Idaomar, M. Biological effects of essential oils—A review. Food Chem. Toxicol. 2008, 46, 446–475. [Google Scholar] [CrossRef] [PubMed]
- Sá, R.C.S.; Andrade, L.N.; Sousa, D.P. A review on anti-inflammatory activity of monoterpenes. Molecules 2013, 18, 1227–1254. [Google Scholar] [CrossRef] [PubMed]
- Pichersky, E.; Noel, J.P.; Dudareva, N. Biosynthesis of plant volatiles: Nature’s diversity and ingenuity. Science 2006, 311, 808–811. [Google Scholar] [CrossRef] [PubMed]
- Bernardes, W.A.; Lucarini, R.; Tozatti, M.G.; Flauzino, L.G.; Souza, M.G.; Turatti, I.C.; Andrade e Silva, M.L.; Martins, C.H.; da Silva Filho, A.A.; Cunha, W.R. Antibacterial activity of the essential oil from Rosmarinus officinalis and its major components against oral pathogens. Z. Naturforschung C 2010, 65, 588–593. [Google Scholar]
- Botelho, M.A.; Santos, R.A.; Martins, J.G.; Carvalho, C.O.; Paz, M.C.; Azenha, C.; Ruela, R.S.; Queiroz, D.B.; Ruela, W.S.; Marinho, G.; et al. Efficacy of a mouthrinse based on leaves of the neem tree (Azadirachta indica) in the treatment of patients with chronic gingivitis: A double-blind, randomized, controlled trial. J. Med. Plant Res. 2008, 2, 341–346. [Google Scholar]
- Preus, H.R.; Koldsland, O.C.; Aass, A.M.; Sandvik, S.; Hansen, B.F. The plaque- and gingivitis-inhibiting capacity of a commercially available essential oil product. A parallel, split-mouth, single blind, randomized, placebo-controlled clinical study. Acta Odontol. Scand. 2013, 71, 1613–1619. [Google Scholar] [CrossRef] [PubMed]
- Van Leeuwen, M.P.; Slot, D.E.; van der Weijden, G.A. The effect of an essential-oils mouthrinse as compared to a vehicle solution on plaque and gingival inflammation: A systematic review and meta-analysis. Int. J. Dent. Hyg. 2014, 12, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Cecchini, C.; Silvi, S.; Cresci, A.; Piciotti, A.; Caprioli, G.; Papa, F.; Sagratini, G.; Vittori, S.; Maggi, F. Antimicrobial efficacy of Achillea ligustica All. (Asteraceae) essential oils against reference and isolated oral microorganisms. Chem. Biodivers. 2012, 9, 12–24. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.D.; Jeong, M.R.; Jeong, S.I.; Moon, S.E.; Kil, B.S.; Yun, S.I.; Lee, K.Y.; Song, Y.H. Chemical composition and antimicrobial activity of the essential oil of Cryptomeria japonica. Phytother. Res. 2007, 21, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Alviano, W.S.; Mendonça-Filho, R.R.; Alviano, D.S.; Bizzo, H.R.; Souto-Padrón, T.; Rodrigues, M.L.; Bolognese, A.M.; Alviano, C.S.; Souza, M.M. Antimicrobial activity of Croton cajucara Benth linalool-rich essential oil on artificial biofilms and planktonic microorganisms. Oral Microbiol. Immunol. 2005, 20, 101–105. [Google Scholar] [CrossRef] [PubMed]
- Maggi, F.; Bramucci, M.; Cecchini, C.; Coman, M.M.; Cresci, A.; Cristalli, G.; Lupidi, G.; Papa, F.; Quassinti, L.; Sagratini, G.; et al. Composition and biological activity of essential oil of Achillea ligustica All. (Asteraceae) naturalized in central Italy: Ideal candidate for anti-cariogenic formulations. Fitoterapia 2009, 80, 313–319. [Google Scholar] [CrossRef] [PubMed]
- Aguiar, G.P.; Carvalho, C.E.; Dias, H.J.; Reis, E.B.; Martins, M.H.; Wakabayashi, K.A.; Groppo, M.; Martins, C.H.; Cunha, W.R.; Crotti, A.E. Antimicrobial activity of selected essential oils against cariogenic bacteria. Nat. Prod. Res. 2013, 27, 1668–1672. [Google Scholar] [CrossRef] [PubMed]
- Shayegh, S.; Rasooli, I.; Taghizadeh, M.; Astaneh, S.D. Phytotherapeutic inhibition of supragingival dental plaque. Nat. Prod. Res. 2008, 22, 428–439. [Google Scholar] [CrossRef] [PubMed]
- Takarada, K.; Kimizuka, R.; Takahashi, N.; Honma, K.; Okuda, K.; Kato, T. A comparison of the antibacterial efficacies of essential oils against oral pathogens. Oral Microbiol. Immunol. 2004, 19, 61–64. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.E.; Kim, H.Y.; Cha, J.D. Synergistic effect between clove oil and its major compounds and antibiotics against oral bacteria. Arch. Oral Biol. 2011, 56, 907–916. [Google Scholar] [CrossRef] [PubMed]
- Silvestri, J.D.F.; Paroul, N.; Czyewski, E.; Lerin, L.; Rotava, I.; Cansian, R.L.; Mossi, A.; Toniazzo, G.; Oliveira, D.; Treichel, H. Perfil da composição química e atividades antibacteriana e antioxidante do óleo essencial do cravo-da-índia (Eugenia caryophyllata Thunb.). Rev. Ceres 2010, 57, 589–594. [Google Scholar] [CrossRef]
- Hammer, K.A.; Dry, L.; Johnson, M.; Michalak, E.M.; Carson, C.F.; Riley, T.V. Susceptibility of oral bacteria to Melaleuca alternifolia (tea tree) oil in vitro. Oral Microbiol. Immunol. 2003, 18, 389–392. [Google Scholar] [CrossRef] [PubMed]
- Thaweboon, S.; Thaweboon, B. In vitro antimicrobial activity of Ocimum americanum L. essential oil against oral microorganisms. Southeast Asian J. Trop. Med. Public Health 2009, 40, 1025–1233. [Google Scholar] [PubMed]
- Rasooli, I.; Shayegh, S.; Taghizadeh, M.; Astaneh, S.D.A. Rosemarinus officinalis and Thymus eriocalyx essential oils combat in vitro and in vivo dental biofilm formation. Pharmacogn. Mag. 2008, 14, 65–74. [Google Scholar]
- Vagionas, K.; Graikou, K.; Ngassapa, O.; Runyoro, D.; Chinou, I. Composition and antimicrobial activity of the essential oils of three Satureja species growing in Tanzania. Food Chem. 2007, 103, 319–324. [Google Scholar] [CrossRef]
- Shapiro, S.; Meier, A.; Guggenheim, B. The antimicrobial activity of essential oils and essential oil components towards oral bacteria. Oral Microbiol. Immunol. 1994, 9, 202–208. [Google Scholar] [CrossRef] [PubMed]
- Roldán, L.P.; Díaz, G.J.; Duringer, J.M. Composition and antibacterial activity of essential oils obtained from plants of the Lamiaceae family against pathogenic and beneficial bacteria. Rev. Colomb. Cienc. Pecu. 2010, 23, 451–446. [Google Scholar]
- Al-Bayati, F.A. Isolation and identification of antimicrobial compound from Mentha longifolia L. leaves grown wild in Iraq. Ann. Clin. Microbiol. Antimicrob. 2009, 12, 8–20. [Google Scholar]
- Botelho, M.A.; Bezerra-Filho, J.G.; Correa, L.L.; Fonseca, S.G.C.; Montenegro, D.; Gapski, R.; Brito, G.A.C.; Heukelbach, J. Effect of a novel essential oil mouthrinse without alcohol on gingivitis: A double-blinded randomized controlled trial. J. Appl. Oral Sci. 2007, 15, 175–180. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, I.S.C.; Tavares, V.N.; Pereira, S.L.S.; Costa, F.N. Antiplaque and antigingivitis effect of Lippia sidoides. A double-blind clinical study in humans. J. Appl. Oral Sci. 2009, 17, 404–407. [Google Scholar] [CrossRef] [PubMed]
- Lauten, J.D.; Boyd, L.; Hanson, M.B.; Lillie, D.; Gullion, C.; Madden, T.E. A Clinical Study: Melaleuca, Manuka, Calendula and Green Tea Mouth Rinse. Phytother. Res. 2005, 19, 951–957. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.H.; Kim, B.S.; Keum, K.S.; Yu, H.H.; Kim, Y.H.; Chang, B.S.; Ra, J.Y.; Moon, H.D.; Seo, B.R.; Choi, N.Y.; et al. Essential oil of Curcuma longa inhibits Streptococcus mutans biofilm formation. J. Food Sci. 2011, 76, H226–H230. [Google Scholar] [CrossRef] [PubMed]
- Rasooli, I.; Shayegh, S.; Taghizadeh, M.; Astaneh, S.D. Phytotherapeutic prevention of dental biofilm formation. Phytother. Res. 2008, 22, 1162–1167. [Google Scholar] [CrossRef] [PubMed]
- Lang, G.; Buchbauer, G. A review on recent research results (2008–2010) on essential oils as antimicrobials and antifungals. A review. Flavour Fragr. J. 2012, 27, 13–39. [Google Scholar] [CrossRef]
- Lobo, P.L.; Fonteles, C.S.; Marques, L.A.; Jamacaru, F.V.; Fonseca, S.G.; de Carvalho, C.B.; de Moraes, M.E. The efficacy of three formulations of Lippia sidoides Cham. essential oil in the reduction of salivary Streptococcus mutans in children with caries: A randomized, double-blind, controlled study. Phytomedicine 2014, 21, 1043–1047. [Google Scholar] [CrossRef] [PubMed]
- Vu, B.; Chen, M.; Crawford, R.J.; Ivanova, E.P. Bacterial extracellular polysaccharides involved in biofilm formation. Molecules 2009, 13, 2535–2554. [Google Scholar] [CrossRef]
- Loesche, W.J. Role of Streptococcus mutans in Human Dental Decay. Microbiol. Rev. 1986, 50, 353–380. [Google Scholar] [PubMed]
- Gross, E.L.; Beall, C.J.; Kutsch, S.R.; Firestone, N.D.; Leys, E.J.; Griffen, A.L. Beyond Streptococcus mutans: Dental Caries Onset Linked to Multiple Species by 16S rRNA Community Analysis. PLoS ONE 2012, 7, e47722. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.I.; Aweh, A.J.; Coker, A.O.; Savage, K.O.; Abosede, D.A.; Oyedeji, K.S. Lactobacilli in human dental caries and saliva. Microbios 2001, 105, 77–85. [Google Scholar] [PubMed]
- Marsh, P.D. Microbiology of Dental Plaque Biofilms and Their Role in Oral Health and Caries. Dent. Clin. North Am. 2010, 54, 441–454. [Google Scholar] [CrossRef] [PubMed]
- Lodi, G. Pianti Officinali Italiane, 2nd ed.; Edagricole: Bologna, Italy, 2001; p. 397. [Google Scholar]
- Park, Y.K.; Alencar, S.M.; Aguiar, C.L. Botanical origin and chemical composition of Brazilian propolis. J. Agric. Food Chem. 2002, 50, 2502–2506. [Google Scholar] [CrossRef] [PubMed]
- Parreira, N.A.; Magalhães, L.G.; Morais, D.R.; Caixeta, S.C.; Sousa, J.P.; Bastos, J.K.; Cunha, W.R.; Silva, M.L.; Nanayakkara, N.P.; Rodrigues, V.; et al. Antiprotozoal, schistosomicidal, and antimicrobial activities of the essential oil from the leaves of Baccharis dracunculifolia. Chem. Biodivers. 2010, 7, 993–1001. [Google Scholar] [CrossRef] [PubMed]
- Di Stasi, L.C.; Santos, E.M.C.; Moreira dos Santos, C.; Hiruma, C.A. Plantas Medicinais da Amazônia; UNESP: São Paulo, Brazil, 1989; p. 127. [Google Scholar]
- Mdoe, F.P.; Cheng, S.S.; Lyaruu, L.; Nkwengulila, G.; Chang, S.T.; Kweka, E.J. Larvicidal efficacy of Cryptomeria japonica leaf essential oils against Anopheles gambiae. Parasites Vector. 2014, 4, 426. [Google Scholar] [CrossRef]
- Matsunaga, T.; Hasegawa, C.; Kawasuji, T.; Suzuki, H.; Saito, H.; Sagioka, T. Isolation of the antiulcer compound in essential oil from the leaves of Cryptomeria japonica. Biol. Pharm. Bull. 2000, 23, 595–598. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.S.; Lin, H.Y.; Chang, S.T. Chemical composition and antifungal activity of essential oils from different tissues of Japanese Cedar (Cryptomeria japonica). J. Agric. Food Chem. 2005, 53, 614–619. [Google Scholar] [CrossRef] [PubMed]
- Snigdha, C.; Monika, T. Coriandrum sativum: A promising functional and medicinal food. Int. J. Phytomed. Relat. Ind. 2013, 5, 59–65. [Google Scholar]
- Freires, I.A.; Murata, R.M.; Furletti, V.F.; Sartoratto, A.; Alencar, S.M.; Figueira, G.M.; Rodrigues, J.A.O.; Duarte, M.C.T.; Rosalen, P.L. Coriandrum sativum L. (coriander) essential oil: Antifungal activity and mode of action on Candida spp., and molecular targets affected in human whole-genome expression. PLoS ONE 2014, 9, e99086. [Google Scholar] [CrossRef] [PubMed]
- Freires, I.A.; Bueno-Silva, B.; Galvão, L.C.C.; Duarte, M.C.T.; Sartoratto, A.; Figueira, G.M.; Alencar, S.M.; Rosalen, P.L. The effect of essential oils and bioactive fractions on Streptococcus mutans and Candida albicans biofilms: A confocal analysis. Evid. Based Complement. Altern. Med. 2015, 2015, 871316. [Google Scholar] [CrossRef]
- Harsha, S.N.; Anilakumar, K.R. In vitro free radical scavenging and DNA damage protective property of Coriandrum sativum L. leaves extract. J. Food Sci. Technol. 2012, 51, 1533–1539. [Google Scholar] [CrossRef] [PubMed]
- Sreelatha, S.; Padma, P.R.; Umadevi, M. Protective effects of Coriandrum sativum extracts on carbon tetrachloride-induced hepatotoxicity in rats. Food Chem. Toxicol. 2009, 47, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Chaieb, K.; Hajlaoui, H.; Zmantar, T.; Kahla-Nakbi, A.B.; Rouabhia, M.; Mahdouani, K.; Bakhrouf, A. The chemical composition and biological activity of clove essential oil, Eugenia caryophyllata (Syzigium aromaticum L. Myrtaceae): A short review. Phytother. Res. 2007, 21, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Lacoste, E.; Chaumont, J.P.; Mandin, D.; Plumel, M.M.; Matos, F.J.A. Antiseptic properties of essential oil of Lippia sidoides Cham. Application to the cutaneous microflora. Ann. Pharm. Fr. 1996, 54, 228–230. [Google Scholar] [PubMed]
- Monteiro, M.V.; de Melo Leite, A.K.; Bertini, L.M.; de Morais, S.M.; Nunes Pinheiro, D.C. Topical anti-inflammatory, gastroprotective and antioxidant effects of the essential oil of Lippia sidoides Cham. leaves. J. Ethnopharmacol. 2006, 111, 378–382. [Google Scholar] [CrossRef] [PubMed]
- Botelho, M.A.; Nogueira, N.A.P.; Bastos, G.M.; Fonseca, S.G.C.; Lemos, T.L.G.; Matos, F.J.A.; Montenero, D.; Heukelback, J.; Rao, V.S.; Brito, G.A.C. Antimicrobial activity of the essential oil from Lippia sidoides, carvacrol and thymol against oral pathogens. Braz. J. Med. Biol. Res. 2007, 40, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Yamada, A.N.; Grespan, R.; Yamada, A.T.; Silva, E.L.; Silva-Filho, S.E.; Damião, M.J.; de Oliveira Dalalio, M.M.; Bersani-Amado, C.A.; Cuman, R.K. Anti-inflammatory Activity of Ocimum americanum L. Essential Oil in Experimental Model of Zymosan-Induced Arthritis. Am. J. Chin. Med. 2013, 41, 913–926. [Google Scholar] [CrossRef] [PubMed]
- Shadia, E.; El-Aziz, A.; Omer, E.A.; Sabra, A.S. Chemical Composition of Ocimum americanum Essential Oil and Its Biological Effects Against, Agrotis ipsilon, (Lepidoptera: Noctuidae). Res. J. Agric. Biol. Sci. 2007, 3, 740–747. [Google Scholar]
- Bozin, B.; Mimmkica-Dukic, N.; Samojlik, I.; Jovin, E. Antimicrobial and antioxidant properties of rosemary and sage (Rosmarinus offcinalis L. and Salvia officinalis L., Lamiaceae) essential oils. J. Agric. Food Chem. 2007, 55, 7879–7885. [Google Scholar] [CrossRef] [PubMed]
- Bilia, A.R.; Guccione, C.; Isacchi, B.; Righeschi, C.; Firenzuoli, F.; Bergonzi, M.C. Essential oils loaded in nanosystems: A developing strategy for a successful therapeutic approach. Evid. Based Complement. Altern. Med. 2014, 2014, 651593. [Google Scholar] [CrossRef]
- Işcan, G.; Kirimer, N.; Kürkcüoğlu, M.; Başer, K.H.; Demirci, F. Antimicrobial screening of Mentha piperita essential oils. J. Agric. Food Chem. 2002, 50, 3943–3946. [Google Scholar] [CrossRef] [PubMed]
- Quintas, V.; Prada-López, I.; Prados-Frutos, J.C.; Tomás, I. In situ antimicrobial activity on oral biofilm: Essential oils vs. 0.2% chlorhexidine. Clin. Oral Investig. 2015, 19, 97–107. [Google Scholar] [CrossRef] [PubMed]
- Pramod, K.; Ansari, S.H.; Ali, J. Eugenol: A natural compound with versatile pharmacological actions. Nat. Prod. Commun. 2010, 5, 1999–2006. [Google Scholar] [PubMed]
- Souza-Costa, C.A.; Teixeira, H.M.; Nascimento, A.B.L.; Hebling, J. Biocompatibility of resin-based dental materials applied as liners in deep cavities prepared in human teeth. J. Biomed. Mater. Res. B 2007, 81, 175–184. [Google Scholar] [CrossRef]
- Kohlert, C.; Van Rensen, I.; März, R.; Schindler, G.; Graefe, E.U.; Veit, M. Bioavailability and pharmacokinetics of natural volatile terpenes in animals and humans. Planta Med. 2000, 66, 495–505. [Google Scholar] [CrossRef] [PubMed]
- Michiels, J.; Missotten, J.; Dierick, N.; Freumaut, D.; Maene, P.; Smet, S. In vitro degradation and in vivo passage kinetics of carvacrol, thymol, eugenol and trans-cinnamaldehyde along the gastrointestinal tract of piglets. J. Sci. Food Agric. 2008, 13, 2371–2381. [Google Scholar] [CrossRef]
- Kohlert, C.; Schindler, G.; März, R.W.; Abel, G.; Brinkhaus, B.; Derendorf, H.; Gräfe, E.U.; Veit, M. Systemic availability and pharmacokinetics of thymol in humans. J. Clin. Pharmacol. 2002, 42, 731–731. [Google Scholar] [CrossRef] [PubMed]
- Turek, C.; Stintzing, F.C. Stability of essential oils: A review. Compr. Rev. Food Sci. Food Saf. 2013, 12, 40–53. [Google Scholar] [CrossRef]
- Vlachojannis, C.; Winsauer, H.; Chrubasik, S. Effectiveness and safety of a mouthwash containing essential oil ingredients. Phytother. Res. 2013, 27, 685–691. [Google Scholar] [CrossRef] [PubMed]
- Freires, I.A.; Silva, I.C.; Alves, L.A.; Bezerra, L.M.; Castro, R.D. Clinical applicability of natural product(s)-containing mouthwashes as adjunctive treatment of biofilm-induced gingivitis: A systematic review. Braz. J. Med. Plants 2012, 14, 700–711. [Google Scholar]
- Zero, D.T.; Zhang, J.Z.; Harper, D.S.; Wu, M.; Kelly, S.; Waskow, J.; Hoffman, M. The remineralizing effect of an essential oil fluoride mouthrinse in an intraoral caries test. J. Am. Dent. Assoc. 2004, 135, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Liberati, A.; Altman, D.G.; Tetzlaff, J.; Mulrow, C.; Gøtzsche, P.C.; Loannidis, J.P.A.; Clarke, M.; Devereaux, P.J.; Kleijnen, J.; Moher, D. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. BMJ 2009, 339, b2700. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Duarte, M.C.T.; Leme, E.E.; Delarmelina, C.; Soares, A.A.; Figueira, G.M.; Sartoratto, A. Activity of essential oils from Brazilian medicinal plants on Escherichia coli. J. Ethnopharmacol. 2007, 111, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Tanzer, J.M. Essential dependence of smooth surface caries on, and augmentation of fissure caries by, sucrose and Streptococcus mutans infection. Infect. Immun. 1979, 25, 526–531. [Google Scholar] [PubMed]
- Thylstrup, A.; Fejerskov, O. Cariologia Clínica, 3rd ed.; Santos: São Paulo, Brazil, 2001; p. 421. [Google Scholar]
- Gagnier, J.J.; Boon, H.; Rochon, P.; Moher, D.; Barnes, J.; Bombardier, C. Reporting Randomized, Controlled Trials of Herbal Interventions: An Elaborated CONSORT Statement. Ann. Intern. Med. 2006, 144, 364–367. [Google Scholar] [CrossRef] [PubMed]
- Linde, K.; Jonas, W.B.; Melchart, D.; Willich, S. The methodological quality of randomized controlled trials of homeopathy, herbal medicines and acupuncture. Int. J. Epidemiol. 2001, 30, 526–531. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.K.; Chen, Z.X.; Zhou, Z.G.; Zhang, B.; Tian, J.; Chen, J.P.; Wang, L.; Wang, C.H.; Chen, H.Y.; Li, Y.P. Intravenous chemotherapy for resected gastric cancer: Meta-analysis of randomized controlled trials. World J. Gastroenterol. 2002, 8, 1023–1028. [Google Scholar] [PubMed]
- Beek, D.V.; Gans, J.; McIntyre, P.; Prasad, K. Steroids in adults with acute bacterial meningitis: A systematic review. Lancet Infect. Dis. 2004, 4, 139–143. [Google Scholar] [CrossRef] [PubMed]
- Huntley, A.L.; Ernst, E. Soy for the treatment of perimenopausal symptoms—A systematic review. Maturitas 2004, 47, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Green, S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.0.1 [updated September 2008]. The Cochrane Collaboration: London, UK, 2008. Available online: Http://www.cochrane-handbook.org (accessed on 11 September 2014).
- Sample Availability: Not available.
© 2015 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Freires, I.A.; Denny, C.; Benso, B.; De Alencar, S.M.; Rosalen, P.L. Antibacterial Activity of Essential Oils and Their Isolated Constituents against Cariogenic Bacteria: A Systematic Review. Molecules 2015, 20, 7329-7358. https://doi.org/10.3390/molecules20047329
Freires IA, Denny C, Benso B, De Alencar SM, Rosalen PL. Antibacterial Activity of Essential Oils and Their Isolated Constituents against Cariogenic Bacteria: A Systematic Review. Molecules. 2015; 20(4):7329-7358. https://doi.org/10.3390/molecules20047329
Chicago/Turabian StyleFreires, Irlan Almeida, Carina Denny, Bruna Benso, Severino Matias De Alencar, and Pedro Luiz Rosalen. 2015. "Antibacterial Activity of Essential Oils and Their Isolated Constituents against Cariogenic Bacteria: A Systematic Review" Molecules 20, no. 4: 7329-7358. https://doi.org/10.3390/molecules20047329