Prudent-Active and Fast-Food-Sedentary Dietary-Lifestyle Patterns: The Association with Adiposity, Nutrition Knowledge and Sociodemographic Factors in Polish Teenagers—The ABC of Healthy Eating Project

 ,
,  ,
,  , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Methods
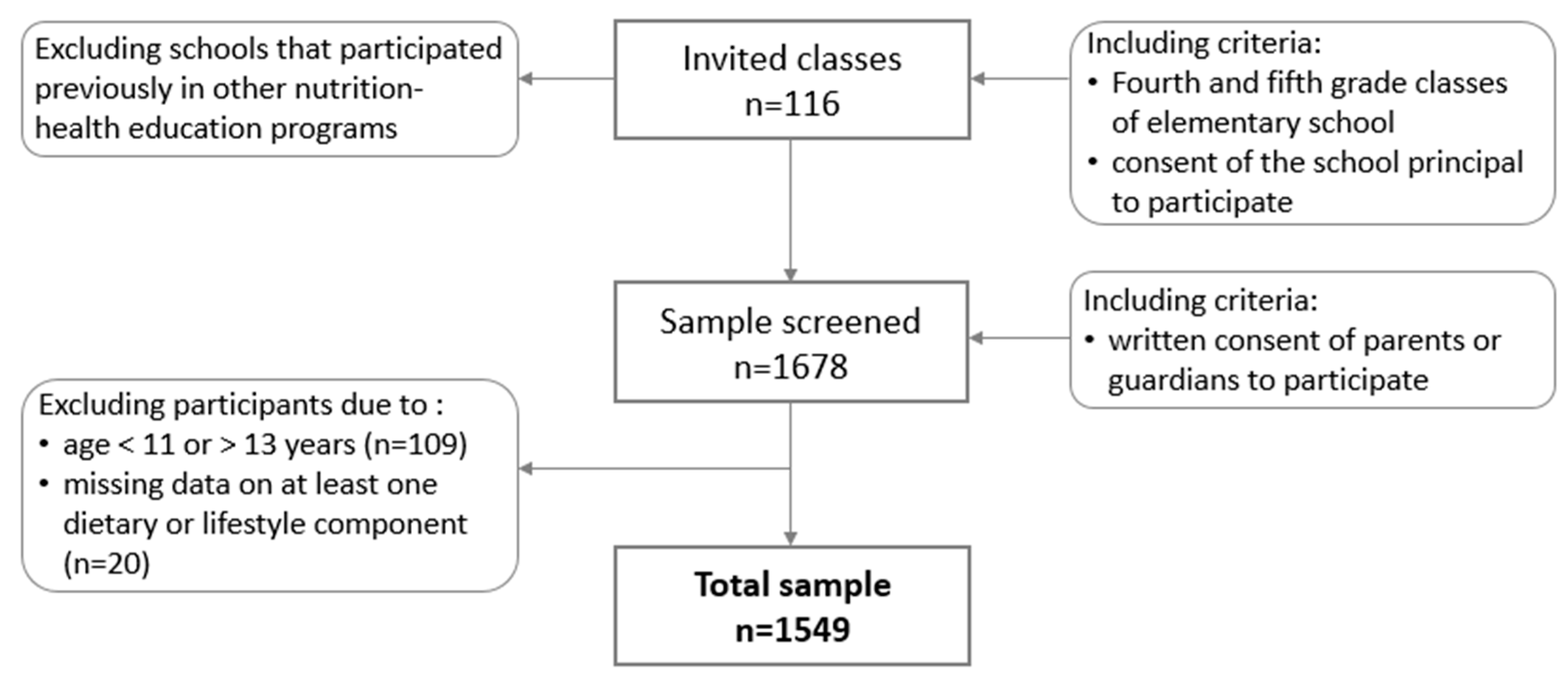
2.1. Study Design and Participants
2.2. Data Collection
2.3. Dietary Data
- four categories of breakfast consumption (number of days/week): 0/week, 1–3/week, 4–6/week, 7/week (every day);
- four categories of school meal consumption (number of days/week): 0/week, 1–3/week, 3–4/week, 5/week (every school day);
- seven categories for food frequency consumption: never or almost never, less than once a week, once a week, 2–4 times/week, 5–6 times/week, every day, several times a day; for further analysis, all frequencies of food consumption were converted into daily frequency (details in Table S1).
2.4. Lifestyle
2.5. Dietary-Lifestyle Patterns
2.6. Nutrition Knowledge
2.7. Socioeconomic Status
- Question: ‘Does your family own a car, van or truck?’ Answers: no (0 points); yes, one (1 point); yes, two or more (2 points).
- Question: ‘In recent years, how many times per year did you go away on holiday with your family?’ (necessary examples were given) Answers: not at all (0 points); once (1 point); twice (2 points); more than twice (2 points).
- Question: ‘Do you have your own bedroom for yourself?’ Answers: no (0 points); yes (1 point).
- Question: ‘How many computers or laptops or tablets does your family own?’ Answers: none (0 points); one (1 point); two (2 points); more than two (2 points).
2.8. Adiposity Measures
2.9. Ethical Approval
2.10. Statistical Analysis
- (i)
- the adherence to chosen a DLP by sociodemographic factors and nutrition knowledge in respect to a referent DLP—the following categorical variables were used as predictors (independent variables): gender (girls, reference: boys), age (12 or 13 years, reference: 11 years), residence (urban, reference: rural), Family Affluence Scale (moderate or high, reference: low), nutrition knowledge score (middle or upper tertile, reference: bottom tertile);
- (ii)
- the chance to fall in the adiposity category (central obesity or overweight)—two opposite DPLs were used as predictors while others were used as a referent (i.e., in total, three various pairs of DPLs were analysed).
3. Results
3.1. Dietary-Lifestyle Patterns Characteristic
3.2. Association between Dietary-Lifestyle Patterns, Sociodemographic Factors and Nutrition Knowledge
3.3. Association between Dietary-Lifestyle Patterns and Adiposity Measures
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Data availability statement
References
- Baxter, S.D. Cognitive processes in children’s dietary recalls: Insight from methodological studies. Eur. J. Clin. Nutr. 2009, 63, 19–32. [Google Scholar] [CrossRef] [PubMed]
- Fitzgerald, A.F.; Heary, C.; Nixon, E.; Kelly, C. Gender differences in factors influencing dietary patterns among Irish children and adolescents. Proc. Nutr. Soc. 2010, 69, E385. [Google Scholar] [CrossRef]
- Marshall, S.; Jones, D.; Ainsworth, B.; Reis, J.; Levy, S.; Macera, C. Race/ethnicity, social class, and leisure-time physical inactivity. Med. Sci. Sports Exercise 2007, 39, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Marques, A.; da Costa, F.C. Levels of physical activity of urban adolescents according to age and gender. Int. J. Sports Sci. 2013, 3, 23–27. [Google Scholar]
- Ferrari, K.E.; Olds, T.S.; Walters, J.L. All the stereotypes confirmed: Differences in how Australian boys and girls use their time. Health Educ. Behav. 2012, 39, 589–595. [Google Scholar] [CrossRef] [PubMed]
- Klomsten, A.T.; Marsh, H.W.; Skaalvik, E.M. Adolescents’ perceptions of masculine and feminine values in sport and physical education: A study of gender differences. Sex Roles 2005, 52, 625–636. [Google Scholar] [CrossRef]
- Jago, R.; Fox, K.R.; Page, A.S.; Brockman, R.; Thompson, L. Physical activity and sedentary behaviour typologies of 10-11 years old. Int. Behav. Nutr. Phys. Act. 2011, 7, 8–49. [Google Scholar] [CrossRef]
- Ranjit, N.; Evans, M.H.; Byrd-Williams, C.; Evans, A.E.; Hoelscher, D.M. Dietary and activity correlates of sugar-sweetened beverage consumption among adolescents. Pediatrics 2010, 126, e754–e761. [Google Scholar] [CrossRef]
- Popkin, B.M.; Adair, L.S.; Ng, S.W. Global nutrition transition and the pandemic of obesity in developing countries. Nutr. Rev. 2012, 70, 3–21. [Google Scholar] [CrossRef] [Green Version]
- Gubbels, J.S.; Kremers, S.P.; Stafleu, A.; Goldbohm, R.A.; de Vries, N.K.; Thijs, C. Clustering of energy balance-related behaviors in 5-year-old children: Lifestyle patterns and their longitudinal association with weight status development in early childhood. Int. J. Behav. Nutr. Phys. Act. 2012, 9, 77–91. [Google Scholar] [CrossRef]
- United States Department of Agriculture (USDA). A Series of Systematic Reviews on the Relationship between Dietary Patterns and Health Outcome. Available online: https://www.cnpp.usda.gov/2014 (accessed on 4 July 2018).
- Hu, H.B. Dietary pattern analysis: A new direction in nutrition epidemiology. Curr. Opin. Lipidol. 2002, 13, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Rachel, E.; Laxer, R.E.; Brownson, R.C.; Dubin, J.A.; Cooke, M.; Chaurasia, A.; Leatherdale, S.T. Clustering of risk-related modifiable behaviours and their association with overweight and obesity among a large sample of youth in the COMPASS study. BMC Public Health 2017, 17, 102. [Google Scholar]
- Pérez-Rodrigo, C.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Aranceta-Bartrina, J. Clustering of dietary patterns, lifestyles, and overweight among spanish children and adolescents in the ANIBES study. Nutrients 2016, 8, 11. [Google Scholar] [CrossRef] [PubMed]
- Nuutinen, T.; Lehto, E.; Ray, C.; Roos, E.; Villberg, J.; Tynjälä, J. Clustering of energy balance-related behaviours, sleep, and overweight among Finnish adolescents. Int. J. Public Health 2017, 62, 929–938. [Google Scholar] [CrossRef] [PubMed]
- Mandic, S.; Bengoechea, E.G.; Coppell, K.J.; Spence, J.C. Clustering of (Un)healthy behaviors in adolescents from Dunedin, New Zealand. Am. J. Health Behav. 2017, 41, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Dupuy, M.; Godeau, E.; Vignes, C.; Ahluwalia, N. Socio-demographic and lifestyle factors associated with overweight in a representative sample of 11–15 years old in France: Results from the WHO-Collaborative Health Behaviour in School-aged Children (HBSC) cross-sectional study. BMC Public Health 2011, 11, 442. [Google Scholar] [CrossRef] [PubMed]
- Eisenburg, L.K.; Corpeleijn, E.; van Sluijs, E.M.F.; Atkin, A.J. Clustering and correlates of multiple health behaviours in 9–10 year old children. PLoS ONE 2014, 9, e99498. [Google Scholar] [CrossRef]
- Lioret, S.; Touvier, M.; Lafay, L.; Volatier, J.C.; Maire, B. Dietary and physical activity patterns in French children are related to overweight and socioeconomic status. J. Nutr. 2008, 138, 101–107. [Google Scholar] [CrossRef]
- Ambrosini, G.L.; Emmett, P.M.; Northstone, K.; Howe, L.D.; Tilling, K.; Jebb, S.A. Identification of a dietary pattern prospectively associated with increased adiposity during childhood and adolescence. Int. J. Obes 2012, 36, 1299–1305. [Google Scholar] [CrossRef]
- Hinnig, P.F.; Monteiro, J.S.; Altenburg de Assis, M.A.; Levy, R.B.; Peres, M.A.; Perazi, F.M.; Porporatti, A.L.; De Luca Santo, G. Dietary patterns of children and adolescents from high, medium and low human development countries and associated socioeconomic factors: A systematic review. Nutrients 2018, 10, 436. [Google Scholar] [CrossRef]
- Jodkowska, M.; Oblacińska, A.; Tabak, I. Patterns of physical activity and sedentary behaviors among 13-year-olds in Poland. Pediatria Polska 2013, 88, 508–513. [Google Scholar] [CrossRef]
- Northstone, K.; Smith, A.D.A.C.; Newby, P.K.; Emmett, P.M. Longitudinal comparisons of dietary patterns derived by cluster analysis in 7- to 13-year-old children. Br. J. Nutr. 2012, 109, 1–9. [Google Scholar] [CrossRef]
- Corrêa, R.S.; Vencato, P.H.; Rockett, F.C.; Bosa, V.L. Dietary patterns: Are there differences between children and adolescents? Ciênc Saúde Coletiva 2017, 22, 553–562. [Google Scholar] [CrossRef]
- Te Velde, S.J.; De Bourdeaudhuij, I.; Thorsdottir, I.; Rasmussen, M.; Hagströmer, M.; Klepp, K.I.; Brug, J. Patterns in sedentary and exercise behaviors and associations with overweight in 9-14-year-old boys and girls—a cross-sectional study. BMC Public Health 2007, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Hamulka, J.; Wadolowska, L.; Hoffman, M.; Kowalkowska, J.; Gutkowska, K. The effect of an education program on nutrition knowledge, attitudes toward nutrition, diet quality, lifestyle, and body composition in Polish teenagers. The ABC of Healthy Eating project: Design, protocol, and methodology. Nutrients 2018, 10, 1439. [Google Scholar] [CrossRef]
- Pereira, M.A.; Erickson, E.; McKee, P.; Schrankler, K.; Raatz, S.K.; Lytle, L.A.; Pellegrini, A.D. Breakfast frequency and quality may affect glycemia and appetite in adults and children. J. Nutr. 2011, 141, 163–168. [Google Scholar] [CrossRef] [PubMed]
- Whati, L.H.; Senekal, M.; Steyn, N.P.; Nel, J.H.; Lombard, C.; Norris, S. Development of a reliable and valid nutritional knowledge questionnaire for urban South African adolescents. Nutrition 2005, 21, 76–85. [Google Scholar] [CrossRef] [PubMed]
- Mazur, J. Family affluence scale—validation study and suggested modification. Hygeia Public Health 2013, 48, 211–217. [Google Scholar]
- Cole, T.J.; Lobstein, T. Extended international (IOTF) body mass index cut-offs for thinness, overweight and obesity. Pediatric Obes. 2012, 7, 284–294. [Google Scholar] [CrossRef]
- Kułaga, Z.; Litwin, M.; Tkaczyk, M.; Palczewska, I.; Zajączkowska, M.; Zwolińska, D.; Krynicki, T.; Wasilewska, A.; Moczulska, A.; Morawiec-Knysak, A.; et al. Polish 2010 growth references for school-aged children and adolescents. Eur. J. Pediatrics 2011, 170, 599–609. [Google Scholar] [CrossRef]
- Ashwell, M.; Gunn, P.; Gibson, S. Waist-to-height ratio is a better screening tool than waist circumference and BMI for adult cardiometabolic risk factors: Systematic review and meta-analysis. Obes. Rev. 2012, 13, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Huh, J.; Riggs, N.R.; Spruijt-Metz, D.; Chou, C.P.; Huang, Z.; Pentz, M. Identifying patterns of eating and physical activity in children: A latent class analysis of obesity risk. Obesity 2011, 19, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Smetanina, N.; Albaviciute, E.; Babinska, V.; Karinauskiene, L.; Albertsson-Wikland, K.; Petrauskiene, A.; Verkauskiene, R. Prevalence of overweight/obesity in relation to dietary habits and lifestyle among 7–17 years old children and adolescents in Lithuania. BMC Public Health 2015, 15, 1001. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mu, M.; Xu, L.F.; Hu, D.; Wu, J.; Bai, M.J. Dietary Patterns and Overweight/Obesity: A Review Article. Iran. J. Public Health 2017, 46, 869–876. [Google Scholar] [PubMed]
- Janssen, I.; Katzmarzyk, P.T.; Boyce, W.F.; Vereecken, C.; Mulvihill, C.; Roberts, C.; Currie, C.; Pickett, W.; Health Behaviour in School-Aged Children Obesity Working Group. Comparison of overweight and obesity prevalence in school-aged youth from 34 countries and their relationships with physical activity and dietary patterns. Obes. Rev. 2005, 6, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Patrick, K.; Norman, G.J.; Calfas, K.J.; Sallis, J.F.; Zabinski, M.F.; Rupp, J.; Cella, J. Diet, physical activity, and sedentary behaviors as risk factors for overweight in adolescence. Arch. Pediatrics Adolesc. Med. 2004, 158, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Oellingrath, I.M.; Svendsen, M.V.; Brantsaeter, A.L. Tracking of eating patterns and overweight – a follow-up study of Norwegian schoolchildren from middle childhood to early adolescence. Nutr. J. 2011, 6, 106–118. [Google Scholar] [CrossRef]
- Moschonis, G.; Kalliora, A.C.; Costarelli, V.; Papandreou, Ch.; Koutoukidis, D.; Lionis, Ch.; Chrousos, G.P.; Manios, Y. on behalf of the Healthy Growth Study Group. Identification of lifestyle patterns associated with obesity and fat mass in children: The Healthy Growth Study. Public Health Nutr. 2013, 17, 614–624. [Google Scholar] [CrossRef]
- Cutler, G.J.; Flood, A.; Hannan, P.J.; Slavin, J.L.; Neumark-Sztainer, D. Association between major patterns of dietary intake and weight status in adolescents. Br. J. Nutr. 2012, 108, 349–356. [Google Scholar] [CrossRef]
- Wadolowska, L.; Kowalkowska, J.; Czarnocinska, J.; Jezewska-Zychowicz, M.; Babicz-Zielinska, E. Comparing dietary patterns derived by two methods and their associations with obesity in Polish girls aged 13–21 years: The cross-sectional GEBaHealth study. Perspect. Public Health 2017, 137, 182–189. [Google Scholar] [CrossRef]
- Gutiérrez-Pliego, E.; del Socorro Camarillo-Romero, L.; Montenegro-Morales, E.P.; José, L.G. Dietary patterns associated with body mass index (BMI) and lifestyle in Mexican adolescents. BMC Public Health 2016, 16, 850. [Google Scholar] [CrossRef]
- Santos, N.H.; Fiaccone, R.L.; Barreto, M.L.; Silva, L.A.; Silva, R. Association between eating patterns and body mass index in a sample of children and adolescents in Northeastern Brazil. Cadernos de Saúde Pública 2014, 30, 2235–2245. [Google Scholar] [CrossRef] [Green Version]
- Pinho, M.G.M.; Aadami, F.; Benedet, J.; Vasconcelos, F. Association between screen time and dietary patterns and overweight/obesity among adolescents. Rev. Nutr. 2017, 30, 377–389. [Google Scholar] [CrossRef] [Green Version]
- Aranceta, J.; Perez-Rodrigo, C.; Ribas, L.; Serra-Majem, L. Sociodemographic and lifestyle determinants of food patterns in Spanish children and adolescents: The enKid study. Eur. J. Clin. Nutr. 2003, 57, 40–44. [Google Scholar] [CrossRef]
- Grosso, G.; Mistretta, A.; Turconi, G.; Cena, H.; Roggi, C.; Galvano, F. Nutrition knowledge and other determinants of food intake and lifestyle habits in children and young adolescents living in a rural area of Sicily, South Italy. Public Health Nutr. 2012, 16, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Gower, J.R.; Moyer-Mileur, L.J.; Wilkinson, R.D.; Slater, H.; Jordan, K.C. Validity and reliability of a nutrition knowledge survey for assessment in elementary school children. J. Am. Diet Assoc. 2010, 110, 452–456. [Google Scholar] [CrossRef] [PubMed]
- Cutler, G.J.; Flood, A.; Hannan, P.; Neumark-Sztainer, D. Multiple sociodemographic and socioenvironmental characteristics are correlated with major patterns of dietary intake in adolescents. J. Am. Diet Assoc. 2011, 111, 230–240. [Google Scholar] [CrossRef]
- Petrauskienė, A.; Žaltauskė, V.; Albavičiūtė, E. Family socioeconomic status and nutrition habits of 7–8 year old children: Cross-sectional Lithuanian COSI study. Ital. J. Pediatrics 2015, 41, 34. [Google Scholar] [CrossRef]
- Voráčová, J.; Sigmund, E.; Sigmundová, D.; Kalman, M. Family affluence and the eating habits of 11- to 15-year-old Czech adolescents: HBSC 2002 and 2014. Int. J. Environ. Res. Public Health 2016, 13, 1034. [Google Scholar] [CrossRef]
- Darmon, N.; Drewnowski, A. Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: A systematic review and analysis. Nutr. Rev. 2015, 73, 643–660. [Google Scholar] [CrossRef]
- Darmon, N.; Drewnowski, A. Does social class predict diet quality? Am. J. Clin. Nutr. 2008, 87, 1107–1117. [Google Scholar] [CrossRef] [PubMed]
- Fismen, A.S.; Samdal, O.; Torsheim, T. Family affluence and cultural capital as indicators of social inequalities in adolescent’s eating behaviours: A population-based survey. BMC Public Health 2012, 12, 1036. [Google Scholar] [CrossRef] [PubMed]
- Anzman, S.L.; Rollins, B.Y.; Birch, L.L. Parental influence on children’s early eating environments and obesity risk: Implications for prevention. Int. J. Obes. 2010, 34, 1116–1124. [Google Scholar] [CrossRef] [PubMed]
- Fielding-Singh, P.; Wan, J. Table talk: How mothers and adolescents across socioeconomic status discuss food. Soc. Sci. Med. 2017, 187, 49–57. [Google Scholar] [CrossRef] [PubMed]
- Kantomaa, M.T.; Tammelin, T.H.; Näyhä, S.; Taanila, A.M. Adolescents’ physical activity in relation to family income and parents’ education. Prev. Med. 2007, 44, 410–415. [Google Scholar] [CrossRef] [PubMed]
- Drenowatz, C.D.; Eisenmann, J.C.; Pfeiffer, K.A.; Welk, G.; Heelan, K.; Gentile, D.; Walsh, D. Influence of socio-economic status on habitual physical activity and sedentary behavior in 8- to 11-year old children. BMC Public Health 2010, 10, 214. [Google Scholar] [CrossRef] [PubMed]
- McCormack, G.R.; Hawe, P.; Perry, R.; Blackstaffe, A. Associations between familial affluence and obesity risk behaviours among children. Paediatrics Child Health 2011, 16, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Sas-Nowosielski, K.; Ogrodnik, J. Stages of exercise change and screen time in adolescents. New Educ. Rev. 2012, 30, 281–291. [Google Scholar]
- Długosz, A. Wzory żywienia, niepożądane skutki zdrowotne, sytuacja społeczno-ekonomiczna i styl życia młodzieży z mniej zurbanizowanych regionów Polski (Dietary Patterns, Adverse Health Outcomes, Socioeconomic Situation and Lifestyle of Adolescents from Less Urbanized Regions of Poland); UWM: Olsztyn, Poland, 2017; pp. 1–108. [Google Scholar]
- Vašíčková, J.; Groffik, D.; Frömel, K.; Chmelík, F.; Wasowicz, W. Determining gender differences in adolescent physical activity levels using IPAQ long form and pedometers. Ann. Agric. Environ. Med. 2013, 20, 749–755. [Google Scholar]
- Spencer, R.A.; Rehman, L.; Kirk, S.F.L. Understanding gender norms, nutrition, and physical activity in adolescent girls: A scoping review. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 6–16. [Google Scholar] [CrossRef]
- Wadolowska, L.; Kowalkowska, J.; Lonnie, M.; Czarnocinska, J.; Jezewska-Zychowicz, M.; Babicz-Zielinska, E. Associations between physical activity patterns and dietary patterns in a representative sample of Polish girls aged 13–21 years: A cross-sectional study (GEBaHealth Project). BMC Public Health 2016, 16, 698. [Google Scholar] [CrossRef] [PubMed]
- Ball, K.; MacFarlane, A.; Crawford, D.; Savige, G.; Andrianopoulos, N.; Worsley, A. Can social cognitive theory constructs explain socio-economic variations in adolescent eating behaviours? A mediation analysis. Health Educ. Res. 2009, 24, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Larson, N.I.; Neumark-Sztainer, D.R.; Story, M.T.; Wall, M.M.; Harnack, L.J.; Eisenberg, M.E. Fast food intake: Longitudinal trends during the transition to young adulthood and correlates of intake. J. Adolesc. Health 2008, 43, 79–86. [Google Scholar] [CrossRef]
- Blakely, F.; Dunnagan, T.; Haynes, G.; Moore, S.; Pelicane, S. Moderate physical activity and its relationship to select measures of a healthy. Diet J. Rural Health 2004, 20, 160–165. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Jones, S.J.; Sun, H.; Probst, J.C.; Merchant, A.; Cavicchia, P. Diet, physical activity, and sedentary behaviors as risk factors for childhood obesity: An urban and rural comparison. Child Obes. 2012, 8, 440–448. [Google Scholar] [CrossRef] [PubMed]
- Ettienne-Gittens, R.; McKyer, E.L.; Odum, M. Rural versus urban Texas WIC participants’ fruit and vegetable consumption. Am. J. Health Behav. 2013, 37, 130–140. [Google Scholar] [CrossRef] [PubMed]
- Regis, M.F.; de Oliveira, L.M.F.T.; dos Santos, A.R.M.; Leonidio, A.C.R.; Diniz, P.R.B.; de Freitas, C.M.S.M. Urban versus rural lifestyle in adolescents: Associations between environment, physical activity levels and sedentary behavior. Einstein 2016, 14, 461–467. [Google Scholar] [CrossRef] [PubMed]
- Lazarou, C.; Kalavana, T. Urbanization influences dietary habits of Cypriot children: The CYKIDS study. Int. J. Public Health 2009, 54, 69–77. [Google Scholar] [CrossRef]
- GUS, Area and Population in Territorial Cross-Section in 2018. Available online: https://stat.gov.pl/download/gfx/portalinformacyjny/en/defaultaktualnosci/3286/3/23/1/population_size_and_structure_and_vital_statistics_in_poland_31-12-2017.pdf (accessed on 10 November 2018).
- Dietary assessment FAO 2018 Food and Agriculture Organization. Dietary Assessment: A Resource Guide to Method Selection and Application in Low Resource Settings. Available online: http://203.187.160.134:9011/www.fao.org/c3pr90ntc0td/3/i9940en/I9940EN.pdf (accessed on 15 November 2018).
- Kaminska, O.; Foulsham, T. Understanding Sources of Social Desirability Bias in Different Modes: Evidence from Eye-tracking. 2013. Available online: https://www.iser.essex.ac.uk/research/publications/working-papers/iser/2013-04.pdf (accessed on 15 November 2018).
- Klesges, L.M.; Baranowski, T.; Beech, B.; Cullen, K.; Murray, D.M.; Rochon, J.; Pratt, C. Social desirability bias in self-reported dietary, physical activity and weight concerns measures in 8- to 10-year-old African-American girls: Results from the Girls Health Enrichment Multisite Studies (GEMS). Prev. Med. 2004, 38, 78–87. [Google Scholar] [CrossRef]
- Novotny, J.A.; Rumpler, W.V.; Judd, J.T.; Riddick, H.W.; Rhodes, D.; McDowell, M.; Briefel, R. Diet interviews of subject pairs: How different persons recall eating the same foods. J. Am. Diet Assoc. 2001, 101, 1189–1193. [Google Scholar] [CrossRef]


{kind=link}
| Variables | Total Sample | Prudent-Active | Fast-Food-Sedentary | notPrudent-notFast-Food-LowActive | p-Value |
|---|---|---|---|---|---|
| Sample size | 1549 | 454 | 214 | 881 | |
| Sample percentage | 100.0 | 29.3 | 13.8 | 56.9 | |
| Gender | *** | ||||
| boys | 48.5 | 41.9 | 59.3 | 49.3 | |
| girls | 51.5 | 58.1 | 40.7 | 50.7 | |
| Age (years) | * | ||||
| 11 | 16.6 | 20.0 | 13.6 | 15.6 | |
| 12 | 73.5 | 72.3 | 73.3 | 74.2 | |
| 13 | 9.9 | 7.7 | 13.1 | 10.2 | |
| Residence | ns | ||||
| rural | 40.4 | 43.6 | 39.7 | 38.9 | |
| urban | 59.6 | 56.4 | 60.3 | 61.1 | |
| Family Affluence Scale (points) | 6.0 (5.0–7.0) | 6.0 (5.0–7.0) | 5.0 (4.0–6.0) | 6.0 (5.0–6.0) | *** |
| Family Affluence Scale | *** | ||||
| low | 24.4 | 24.0 | 35.0 | 20.4 | |
| moderate | 49.9 | 52.0 | 43.5 | 48.6 | |
| high | 25.7 | 24.0 | 21.5 | 31.0 | |
| Nutrition knowledge score (points) | 6.0 (4.0–8.0) | 7.0 (5.0–9.0) | 5.0 (3.0–7.0) | 6.0 (4.0–8.0) | **** |
| Nutrition knowledge score (tertiles) | **** | ||||
| bottom | 30.9 | 32.3 | 49.1 | 19.6 | |
| middle | 39.2 | 40.5 | 35.5 | 38.3 | |
| upper | 29.9 | 27.2 | 15.4 | 42.1 | |
| Central obesity a | 12.1 | 7.8 | 15.2 | 13.6 | ** |
| BMI-for-age by international standards, 2012 b | * | ||||
| thinness | 9.4 | 8.3 | 9.1 | 10.1 | |
| normal weight | 66.0 | 72.4 | 66.5 | 62.6 | |
| overweight/obesity | 24.6 | 19.3 | 24.4 | 27.4 | |
| BMI-for-age by Polish standards, 2010 c | ns | ||||
| thinness | 3.7 | 3.9 | 4.6 | 3.3 | |
| normal weight | 74.5 | 78.6 | 73.1 | 72.6 | |
| overweight/obesity | 21.9 | 17.5 | 22.3 | 24.1 | |
| Components of dietary-lifestyle patterns | |||||
| Breakfast consumption (days/week) | **** | ||||
| <1 | 5.7 | 3.1 | 15.0 | 4.9 | |
| 1 to 3 | 11.8 | 8.6 | 18.7 | 11.8 | |
| 4 to 6 | 12.6 | 7.5 | 14.5 | 14.6 | |
| every day | 69.9 | 80.8 | 51.8 | 68.7 | |
| School meal consumption (days/week) | **** | ||||
| <1 | 5.7 | 1.1 | 10.7 | 6.8 | |
| 1 to 2 | 7.3 | 1.1 | 18.7 | 7.7 | |
| 3 to 4 | 18.1 | 12.1 | 19.2 | 20.9 | |
| every school day | 68.9 | 85.7 | 51.4 | 64.6 | |
| Frequency of consumption of (times/day) | |||||
| vegetables | 0.43 (0.43–1.00) | 1.00 (0.79–1.00) | 0.43 (0.14–0.79) | 0.43 (0.14–0.79) | **** |
| fruits | 0.79 (0.14–1.00) | 1.00 (0.79–2.00) | 0.43 (0.14–0.79) | 0.43 (0.14–0.79) | **** |
| fruit or vegetable juices | 0.43 (0.14–1.00) | 1.00 (0.43–1.00) | 0.43 (0.14–0.79) | 0.43 (0.14–0.79) | **** |
| dairy products | 0.79 (0.43–1.00) | 1.00 (0.79–1.00) | 0.79 (0.43–1.00) | 0.43 (0.43–0.79) | **** |
| fish | 0.06 (0.06–0.14) | 0.14 (0.06–0.43) | 0.06 (0.00–0.14) | 0.06 (0.06–0.14) | **** |
| fast foods | 0.06 (0.06–0.14) | 0.06 (0.00–0.06) | 0.43 (0.06–0.43) | 0.06 (0.06–0.06) | **** |
| sweetened beverages | 0.43 (0.06–0.43) | 0.14 (0.06–0.43) | 1.00 (0.43–2.00) | 0.14 (0.06–0.43) | **** |
| energy drinks | 0.00 (0.00–0.00) | 0.00 (0.00–0.00) | 0.06 (0.00–0.43) | 0.00 (0.00–0.00) | **** |
| sweets | 0.43 (0.14–0.79) | 0.43 (0.14–0.79) | 1.00 (0.43–1.00) | 0.43 (0.14–0.43) | **** |
| Screen time (h/day) | **** | ||||
| <2 | 46.2 | 59.3 | 15.4 | 46.9 | |
| 2 to <4 | 34.5 | 31.9 | 26.7 | 37.7 | |
| 4 to <6 | 11.5 | 5.9 | 26.6 | 10.7 | |
| 6 to <8 | 4.3 | 2.0 | 11.7 | 3.6 | |
| 8 to <10 | 1.4 | 0.7 | 7.0 | 0.5 | |
| ≥10 | 2.1 | 0.2 | 12.6 | 0.6 | |
| Physical activity at school d | **** | ||||
| low | 5.6 | 1.1 | 10.3 | 6.7 | |
| moderate | 48.7 | 36.1 | 50.0 | 54.9 | |
| high | 45.7 | 62.8 | 39.7 | 38.4 | |
| Physical activity at leisure time e | **** | ||||
| low | 9.6 | 2.2 | 21.5 | 10.4 | |
| moderate | 40.4 | 26.4 | 40.2 | 47.7 | |
| high | 50.0 | 71.4 | 38.3 | 41.9 |
| Variables | Prudent-Active (Ref.: notPrudent-notFast-Food-LowActive) | Fast-Food-Sedentary (Ref.: notPrudent-notFast-Food-lowActive) | Fast-Food-Sedentary (Ref.: Prudent-Active) | |||
|---|---|---|---|---|---|---|
| Crude Model | Adjusted Model | Crude Model | Adjusted Model | Crude Model | Adjusted Model | |
| Girls (ref.: boys) | 1.35 * | 1.24 | 0.67 ** | 0.73 | 0.49 **** | 0.62 ** |
| (1.07; 1.70) | (0.98; 1.57) | (0.49; 0.90) | (0.54; 1.00) | (0.35; 0.69) | (0.43; 0.89) | |
| Age | ||||||
| 12 years (ref.: 11 years) | 0.76 | 0.71 * | 1.13 | 1.18 | 1.50 | 1.56 |
| (0.56; 1.02) | (0.52; 0.96) | (0.73; 1.75) | (0.75; 1.85) | (0.95; 2.38) | (0.94; 2.59) | |
| 13 years (ref.: 11 years) | 0.59 * | 0.51 ** | 1.47 | 1.56 | 2.51 ** | 3.20 ** |
| (0.37; 0.94) | (0.31; 0.84) | (0.82; 2.64) | (0.84; 2.88) | (1.31; 4.83) | (1.56; 6.54) | |
| Urban residence (ref.: rural) | 0.82 | 0.80 | 0.97 | 0.99 | 1.17 | 1.27 |
| (0.66; 1.04) | (0.63; 1.02) | (0.70; 1.33) | (0.73; 1.35) | (0.84; 1.64) | (0.88; 1.84) | |
| Family Affluence Scale | ||||||
| moderate (ref.: low) | 1.10 | 1.03 | 0.57 ** | 0.60 ** | 0.52 *** | 0.53 ** |
| (0.82; 1.48) | (0.76; 1.40) | (0.40; 0.81) | (0.42; 0.86) | (0.35; 0.77) | (0.34; 0.81) | |
| high (ref.: low) | 1.51 * | 1.32 | 0.61 * | 0.67 | 0.40 **** | 0.49 ** |
| (1.09; 2.10) | (0.94; 1.85) | (0.40; 0.92) | (0.44; 1.02) | (0.26; 0.63) | (0.29; 0.81) | |
| Nutrition knowledge score (tertiles) | ||||||
| middle (ref: bottom) | 1.56 ** | 1.57 ** | 0.58 ** | 0.59 ** | 0.37 **** | 0.38 **** |
| (1.15; 2.10) | (1.16; 2.13) | (0.41; 0.80) | (0.42; 0.82) | (0.25; 0.55) | (0.25; 0.57) | |
| upper (ref: bottom) | 2.55 **** | 2.40 **** | 0.37 ** | 0.42 *** | 0.15 **** | 0.16 **** |
| (1.88; 3.46) | (1.76; 3.29) | (0.18; 0.77) | (0.27; 0.65) | (0.09; 0.23) | (0.10; 0.26) | |
| Dietary-Lifestyle Patterns | Central Obesity a (Ref: Lack) | Overweight/Obesity (Ref: Normal Weight) | |
|---|---|---|---|
| International Standards, 2012 b | Polish Standards, 2010 c | ||
| Prudent-Active (ref.: notPrudent-notFast-food-lowActive) | |||
| Crude model | 0.54 ** | 0.61 *** | 0.67 ** |
| (0.36; 0.80) | (0.46; 0.81) | (0.50; 0.90) | |
| Adjusted model | 0.53 ** | 0.62 ** | 0.67 * |
| (0.35; 0.80) | (0.47; 0.84) | (0.50; 0.91) | |
| Fast-food-Sedentary (ref.: notPrudent-notFast-food-lowActive) | |||
| Crude model | 1.14 | 0.84 | 0.92 |
| (0.74; 1.76) | (0.58; 1.21) | (0.64; 1.34) | |
| Adjusted model | 1.08 | 0.82 | 0.92 |
| (0.69; 1.70) | (0.56; 1.19) | (0.63; 1.34) | |
| Fast-food-Sedentary (ref.: Prudent-Active) | |||
| Crude model | 2.12 ** | 1.37 | 1.38 |
| (1.25; 3.58) | (0.91; 2.07) | (0.90; 2.09) | |
| Adjusted model | 2.22 ** | 1.34 | 1.34 |
| (1.24; 3.97) | (0.86; 2.11) | (0.84; 2.13) | |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wadolowska, L.; Hamulka, J.; Kowalkowska, J.; Kostecka, M.; Wadolowska, K.; Biezanowska-Kopec, R.; Czarniecka-Skubina, E.; Kozirok, W.; Piotrowska, A. Prudent-Active and Fast-Food-Sedentary Dietary-Lifestyle Patterns: The Association with Adiposity, Nutrition Knowledge and Sociodemographic Factors in Polish Teenagers—The ABC of Healthy Eating Project. Nutrients 2018, 10, 1988. https://doi.org/10.3390/nu10121988
Wadolowska L, Hamulka J, Kowalkowska J, Kostecka M, Wadolowska K, Biezanowska-Kopec R, Czarniecka-Skubina E, Kozirok W, Piotrowska A. Prudent-Active and Fast-Food-Sedentary Dietary-Lifestyle Patterns: The Association with Adiposity, Nutrition Knowledge and Sociodemographic Factors in Polish Teenagers—The ABC of Healthy Eating Project. Nutrients. 2018; 10(12):1988. https://doi.org/10.3390/nu10121988
Chicago/Turabian StyleWadolowska, Lidia, Jadwiga Hamulka, Joanna Kowalkowska, Malgorzata Kostecka, Katarzyna Wadolowska, Renata Biezanowska-Kopec, Ewa Czarniecka-Skubina, Witold Kozirok, and Anna Piotrowska. 2018. "Prudent-Active and Fast-Food-Sedentary Dietary-Lifestyle Patterns: The Association with Adiposity, Nutrition Knowledge and Sociodemographic Factors in Polish Teenagers—The ABC of Healthy Eating Project" Nutrients 10, no. 12: 1988. https://doi.org/10.3390/nu10121988