Association between Inflammatory Potential of Diet and Bone-Mineral Density in Korean Postmenopausal Women: Data from Fourth and Fifth Korea National Health and Nutrition Examination Surveys

Abstract
:1. Introduction
2. Materials and Methods
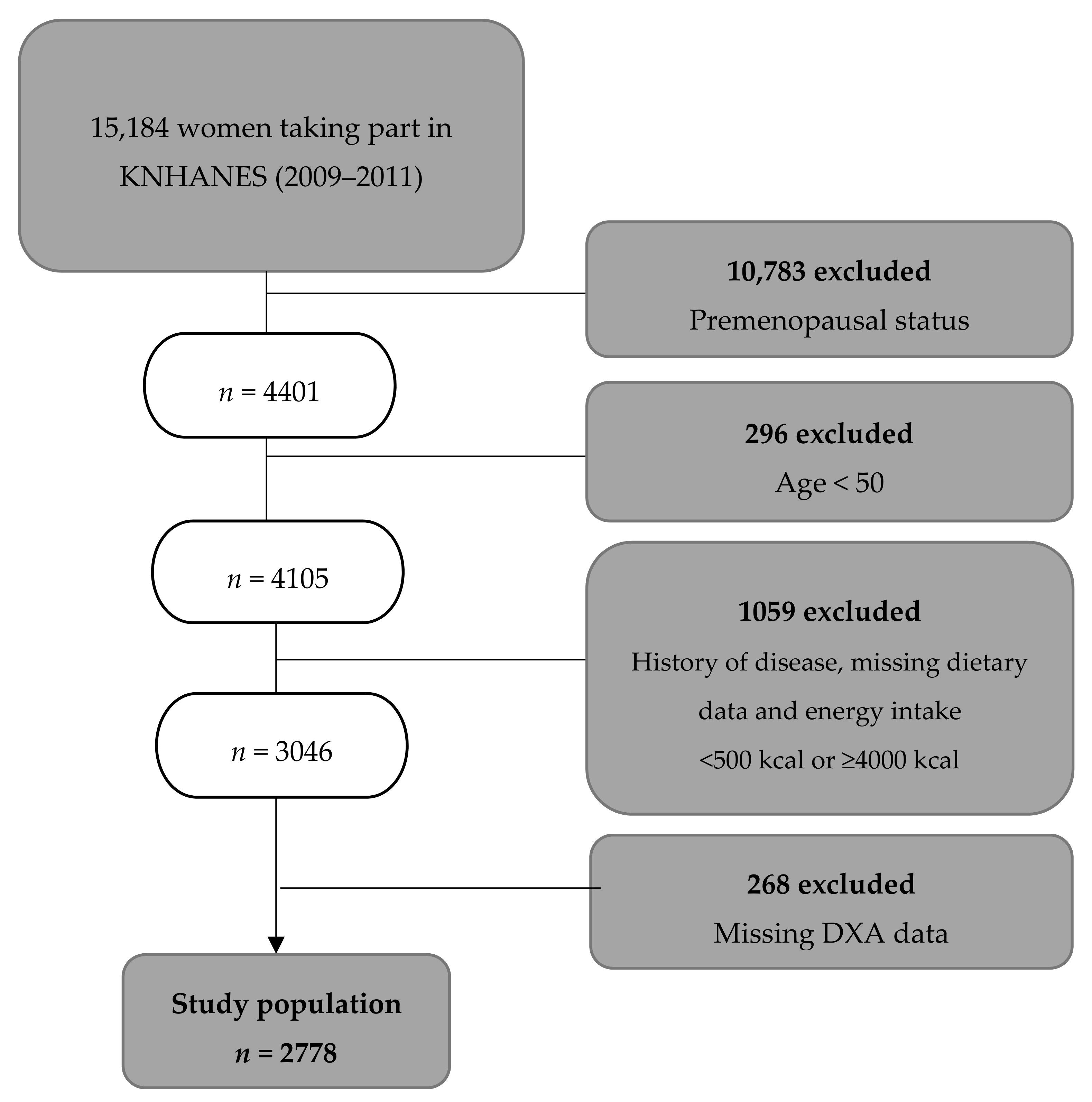
2.1. Study Population
2.2. Analysis of DII®
2.3. Bone-Mineral Density (BMD)
2.4. Covariates
2.5. Statistical Analysis
3. Results
3.1. Characteristics of Study Participants
3.2. BMD According to DII®
3.3. Risk of Osteopenia/Osteoporosis According to DII®
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- Korea National Statistical Office. Korean Statistical Information Service. 2015. Available online: http://kosis.kr/publication/publicationThema.do?pubcode=PJ (accessed on 15 July 2018).
- Oden, A.; McCloskey, E.V.; Kanis, J.A.; Harvey, N.C.; Johansson, H. Burden of high fracture probability worldwide: Secular increases 2010–2040. Osteoporos. Int. 2015, 26, 2243–2248. [Google Scholar] [CrossRef] [PubMed]
- Cauley, J.A. Osteoporosis: Fracture epidemiology update 2016. Curr. Opin. Rheumatol. 2017, 29, 150–156. [Google Scholar] [CrossRef] [PubMed]
- Thulkar, J.; Singh, S.; Sharma, S.; Thulkar, T. Preventable risk factors for osteoporosis in postmenopausal women: Systematic review and meta-analysis. J. Mid-life Health 2016, 7, 108–113. [Google Scholar] [CrossRef] [PubMed]
- Anderson, J.B.; Garner, S.C.; Klemmer, P.J. Diet, Nutrients, and Bone Health; CRC Press: Boca Raton, FL, USA, 2011; ISBN 9781439819555. [Google Scholar]
- Folbert, E.C.; Hegeman, J.H.; Gierveld, R.; Van Netten, J.J.; Van Der Velde, D.; Ten Duis, H.J.; Slaets, J.P. Complications during hospitalization and risk factors in elderly patients with hip fracture following integrated orthogeriatric treatment. Arch. Orthop. Trauma. Surg. 2017, 137, 507–515. [Google Scholar] [CrossRef] [PubMed]
- Bliuc, D.; Alarkawi, D.; Nguyen, T.V.; Eisman, J.A.; Center, J.R. Risk of subsequent fractures and mortality in elderly women and men with fragility fractures with and without osteoporotic bone density: The dubbo osteoporosis epidemiology study. J. Bone Miner. Res. 2015, 30, 637–646. [Google Scholar] [CrossRef] [PubMed]
- Schett, G. Effects of inflammatory and anti-inflammatory cytokines on the bone. Eur. J. Clin. Investig. 2011, 41, 1361–1366. [Google Scholar] [CrossRef]
- ILoi, F.; Córdova, L.A.; Pajarinen, J.; Lin, T.H.; Yao, Z.; Goodman, S.B. Inflammation, fracture and bone repair. Bone 2016, 86, 119–130. [Google Scholar] [CrossRef]
- Pfeilschifter, J.; Koöditz, R.; Pfohl, M.; Schatz, H. Changes in proinflammatory cytokine activity after menopause. Endocr. Rev. 2002, 23, 90–119. [Google Scholar] [CrossRef] [PubMed]
- Barbaresko, J.; Koch, M.; Schulze, M.B.; Nothlings, U. Dietary pattern analysis and biomarkers of low-grade inflammation: A systematic literature review. Nutr. Rev. 2013, 71, 511–527. [Google Scholar] [CrossRef]
- Corley, J.; Kyle, J.A.; Starr, J.M.; McNeill, G.; Deary, I.J. Dietary factors and biomarkers of systemic inflammation in older people: The Lothian birth cohort 1936. Br. J. Nutr. 2015, 114, 1088–1098. [Google Scholar] [CrossRef]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Hébert, J.R. Designing and developing a literature-derived, population-based dietary inflammatory index. Public. Health. Nutr. 2014, 17, 1689–1696. [Google Scholar] [CrossRef]
- Phillips, C.M.; Shivappa, N.; Hebert, J.R.; Perry, I.J. Dietary inflammatory index and biomarkers of lipoprotein metabolism, inflammation and glucose homeostasis in adults. Nutrients. 2018, 10, 1033. [Google Scholar] [CrossRef]
- Shivappa, N.; Wirth, M.D.; Murphy, E.A.; Hurley, T.G.; Hebert, J.R. Association between the Dietary Inflammatory Index (DII) and urinary enterolignans and C-reactive protein from the National Health and Nutrition Examination Survey-2003-2008. Eur. J. Nutr. 2019, 58, 797–805. [Google Scholar] [CrossRef] [PubMed]
- Wirth, M.D.; Shivappa, N.; Davis, L.; Hurley, T.G.; Ortaglia, A.; Drayton, R.; Blair, S.N.; Hebert, J.R. Construct validation of the dietary inflammatory index among African Americans. J. Nutr. Health. Aging. 2017, 21, 487–491. [Google Scholar] [CrossRef]
- Shivappa, N.; Hebert, J.R.; Rietzschel, E.R.; De Buyzere, M.L.; Langlois, M.; Debruyne, E.; Marcos, A.; Huybrechts, I. Associations between dietary inflammatory index and inflammatory markers in the Asklepios Study. Br. J. Nutr. 2015, 113, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Vahid, F.; Shivappa, N.; Faghfoori, Z.; Khodabakhshi, A.; Zayeri, F.; Hebert, J.R.; Davoodi, S.H. Validation of a Dietary Inflammatory Index (DII) and association with risk of gastric cancer: A case-control study. Asian. Pac. J. Cancer. Prev. 2018, 19, 1471–1477. [Google Scholar] [CrossRef] [PubMed]
- Shin, D.; Lee, K.W.; Brann, L.; Shivappa, N.; Hébert, J.R. Dietary inflammatory index is positively associated with serum high-sensitivity C-reactive protein in the Korean adult population. Nutrition 2018, 63–64, 155–161. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Hébert, J.R.; Karamati, M.; Shariati-Bafghi, S.-E.; Rashidkhani, B. Increased inflammatory potential of diet is associated with bone mineral density among postmenopausal women in Iran. Eur. J. Nutr. 2016, 55, 561–568. [Google Scholar] [CrossRef] [PubMed]
- Orchard, T.; Yildiz, V.; Steck, S.E.; Hébert, J.R.; Ma, Y.; Cauley, J.A.; Johnson, K.C.; Sattari, M.; LeBof, M.; Wactawski-Wende, J.; et al. Dietary inflammatory index, bone mineral density, and risk of fracture in postmenopausal women: Results from the Women’s Health Initiative. J. Bone Miner. Res. 2017, 32, 1136–1146. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.S.; Sohn, C.; Kwon, M.; Na, W.; Shivappa, N.; Hébert, J.R.; Kim, M.K. Positive association between dietary inflammatory index and the risk of osteoporosis: Results from the KoGES_Health Examinee (HEXA) cohort study. Nutrients 2018, 10, 1999. [Google Scholar] [CrossRef]
- Correa-Rodríguez, M.; Rueda-Medina, B.; González-Jiménez, E.; Correa-Bautista, J.E.; Ramírez-Vélez, R.; Schmidt-RioValle, J. Dietary inflammatory index, bone health and body composition in a population of young adults: A cross-sectional study. Int. J. Food Sci. Nutr. 2018, 69, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Ha, Y.C. Epidemiology of osteoporosis in Korea. J. Korean Med. Assoc. 2016, 59, 836–841. [Google Scholar] [CrossRef]
- Park, S.; Na, W.; Shon, C. Relationship between osteosarcopenic obesity and dietary inflammatory index in postmenopausal Korean women: 2009 to 2011 Korea National Health and Nutrition Examination Surveys. J. Clin. Biochem. Nutr. 2018, 63, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.; Han, B.G. Cohort Profile: The Korean genome and epidemiology study (KoGES) consortium. Int. J. Epidemiol. 2017, 46, e20. [Google Scholar] [CrossRef]
- Rural Resources Development Institute. Korean Food Composition Table, 7th ed.; Rural Development Administration: Kyonggi-Do, Korea, 2006; ISBN 978-89-480-0142-2[94520].
- U.S. Department of Agriculture. National Nutrient Database for Standard Reference. 2010. Available online: http://www.ars.usda.gov/nutrientdata/ (accessed on 15 May 2018).
- World Health Organization (WHO). Assessment of Fracture Risk and Its Application to Screening for Postmenopausal Osteoporosis: Report of a WHO Study Group [Meeting Held in Rome from 22 to 25 June 1992]; WHO: Geneva, Switzerland, 1994; ISBN 92-4-120843-0. [Google Scholar]
- Mazidi, M.; Shivappa, N.; Wirth, M.D.; Hebert, J.R.; Vatanparast, H.; Kengne, A.P. The association between dietary inflammatory properties and bone mineral density and risk of fracture in US adults. Eur. J. Clin. Nutr. 2017, 71, 1273–1277. [Google Scholar] [CrossRef]
- Miller, P.D.; Siris, E.S.; Barrett-Connor, E.; Faulkner, K.G.; Wehren, L.E.; Abbott, T.A.; Chen, Y.T.; Berger, M.L.; Santora, A.C.; Sherwood, M.L. Prediction of fracture risk in postmenopausal white women with peripheral bone densitometry: Evidence from the national osteoporosis risk assessment. J. Bone Miner. Res. 2002, 17, 2222–2230. [Google Scholar] [CrossRef] [PubMed]
- Cauley, J.A.; Lui, L.; Ensrud, K.E.; Zmuda, J.M.; Stone, K.L.; Hochberg, M.C.; Cumming, S.R. Bone mineral density and the risk of incident nonspinal fractures in black and white women. JAMA 2005, 293, 2102–2108. [Google Scholar] [CrossRef]
- Park, E.J.; Joo, I.W.; Jang, M.-J.; Kim, Y.T.; Oh, K.; Oh, H.J. Prevalence of osteoporosis in the Korean population based on Korea national health and nutrition examination survey (KNHANES), 2008–2011. Yonsei. Med. J. 2014, 55, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Iki, M.; Kagamimori, S.; Kagawa, Y.; Matsuzaki, T.; Yoneshima, H.; Marumo, F. Bone mineral density of the spine, hip and distal forearm in representative samples of the Japanese female population: Japanese population-based Osteoporosis (JPOS) study. Osteoporos. Int. 2001, 12, 529–537. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Jang, S.O. A study on reference values and prevalence of osteoporosis in Korea: The Korea national health and nutrition examination survey 2008–2011. J. Korean Off. Stat. 2013, 18, 42–65. [Google Scholar] [CrossRef]
- Rolland, T.; Boutroy, S.; Vilayphiou, N.; Blaizot, S.; Chapurlat, R.; Szulc, P. Poor trabecular microarchitecture at the distal radius in older men with increased concentration of high-sensitivity C-reactive protein—The Strambo study. Calcif. Tissue Int. 2012, 90, 496–506. [Google Scholar] [CrossRef] [PubMed]
- Wagner, D. Fahrleitner-Pammer, A. Levels of osteoprotegerin (OPG) and receptor activator for nuclear factor kappa B ligand (RANKL) in serum: Are they of any help? Wien. Med. Wochenschr. 2010, 160, 452–457. [Google Scholar] [CrossRef] [PubMed]
- Nowlin, S.Y.; Hammer, M.J.; D’Eramo, M.G. Diet, inflammation, and glycemic control in type 2 diabetes: An integrative review of the literature. J. Nutr. Metab. 2012, 2012, 542–698. [Google Scholar] [CrossRef] [PubMed]
- Shivappa, N.; Steck, S.E.; Hurley, T.G.; Hussey, J.R.; Ma, Y.; Ockene, I.S.; Tabung, F.; Hebert, J.R. A population-based dietary inflammatory index predicts levels of C-reactive protein in the seasonal variation of blood cholesterol study (SEASONS). Public Health Nutr. 2014, 17, 1825–1833. [Google Scholar] [CrossRef] [PubMed]
- Movassagh, E.Z.; Vatanparast, H. Current evidence on the association of dietary patterns and bone health: A scoping review. Adv. Nutr. 2017, 8, 1–16. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.N.; Jho, K.H.; Chung, N.Y. Evaluation of anthropometric characteristics, bone density, food intake frequency, nutrient intakes, and diet quality of pre- and postmenopausal women-based on 2008–2011 Korean national health and nutrition examination survey. J. East Asian Soc. Diet Life 2017, 27, 500–511. [Google Scholar] [CrossRef]


{kind=link}
| Variable | T1 a (n = 926) | T2 (n = 926) | T3 (n = 926) | p Value |
|---|---|---|---|---|
| Age (years) b | 61.28 ± 7.73 | 63.88 ± 8.76 | 65.81 ± 8.84 | <0.001 |
| Body-mass index (kg/m2) | 24.29 ± 3.07 | 24.24 ± 3.23 | 23.95 ± 3.11 | 0.046 |
| Education | <0.001 | |||
| ≤Primary | 474 (51.3) | 617 (66.8) | 689 (74.6) | |
| Middle school | 163 (17.6) | 150 (16.3) | 107 (11.6) | |
| High school | 215 (23.2) | 115 (12.5) | 99 (10.7) | |
| ≥College graduate | 73 (7.9) | 41 (4.4) | 29 (3.1) | |
| Household income | <0.001 | |||
| Low | 247 (26.9) | 350 (38.2) | 399 (43.5) | |
| Moderately low | 225 (24.5) | 249 (27.2) | 239 (26.1) | |
| Moderately high | 216 (23.5) | 174 (19.0) | 145 (15.8) | |
| High | 230 (25.1) | 144 (15.7) | 134 (14.6) | |
| Physical Activity | 0.68 | |||
| Physically active | 123 (13.3) | 93 (10.0) | 94 (10.1) | |
| Physically non-active | 803 (86.7) | 833 (90.0) | 832 (89.9) | |
| Smoking | 0.001 | |||
| None | 876 (94.7) | 852 (92.0) | 834 (90.2) | |
| Ex-smoker | 6 (0.6) | 4 (0.4) | 8 (0.9) | |
| Current smoker | 43 (4.6) | 70 (6.7) | 82 (9.0) | |
| Vitamin D level (ng/mL) | 17.92 ± 6.34 | 18.50 ± 6.94 | 17.81 ± 6.86 | <0.001 |
| Postmenopausal period (years) | 12.23 ± 9.26 | 14.65 ± 10.34 | 17.09 ± 10.76 | <0.001 |
| Female-hormone supplementation | 205 (22.1) | 146 (15.8) | 117 (12.6) | <0.001 |
| Calcium supplementation | 183 (19.8) | 160 (17.3) | 121 (13.1) | <0.001 |
| Calcium intake (mg) c | 561.19 ± 12.69 | 421.19 ± 11.37 | 300.85 ± 12.51 | <0.001 |
| DII® Score | −0.88 ± 1.03 | 1.98 ± 0.63 | 4.12 ± 0.70 | <0.001 |
| Variable | T1 a (n = 926) | T2 (n = 926) | T3 (n = 926) | p Value | p for Trend |
|---|---|---|---|---|---|
| Total femur BMD | |||||
| Crude b | 0.799 ± 0.004 | 0.771 ± 0.004 | 0.751 ± 0.004 | <0.001 | <0.001 |
| Adjusted 1 c | 0.782 ± 0.003 | 0.772 ± 0.003 | 0.767 ± 0.003 | 0.004 | <0.001 |
| Adjusted 2 d | 0.782 ± 0.003 | 0.775 ± 0.003 | 0.771 ± 0.003 | 0.07 | 0.025 |
| Femoral neck BMD | |||||
| Crude | 0.648 ± 0.004 | 0.619 ± 0.004 | 0.599 ± 0.004 | <0.001 | <0.001 |
| Adjusted 1 | 0.631 ± 0.003 | 0.62 ± 0.003 | 0.615 ± 0.003 | 0.001 | <0.001 |
| Adjusted 2 | 0.631 ± 0.003 | 0.623 ± 0.003 | 0.618 ± 0.003 | 0.01 | 0.004 |
| Lumbar-spine BMD | |||||
| Crude | 0.820 ± 0.005 | 0.794 ± 0.005 | 0.777 ± 0.005 | <0.001 | <0.001 |
| Adjusted 1 | 0.804 ± 0.004 | 0.795 ± 0.004 | 0.792 ± 0.004 | 0.08 | <0.001 |
| Adjusted 2 | 0.802 ± 0.004 | 0.797 ± 0.004 | 0.797 ± 0.004 | 0.6 | 0.36 |
| Whole-body total BMD | |||||
| Crude | 1.025 ± 0.004 | 1.001 ± 0.004 | 0.991 ± 0.004 | <0.001 | <0.001 |
| Adjusted 1 | 1.012 ± 0.004 | 1.002 ± 0.004 | 1.003 ± 0.004 | 0.11 | 0.002 |
| Adjusted 2 | 1.010 ± 0.004 | 1.001 ± 0.004 | 1.006 ± 0.004 | 0.25 | 0.39 |
| Variable | T1 a (n = 926) | T2 (n = 926) | T3 (n = 926) | p for Trend | |||
|---|---|---|---|---|---|---|---|
| Case | OR(CI) | Case | OR(CI) | Case | OR(CI) | ||
| Total femur osteopenia + osteoporosis | |||||||
| Crude b | 252 | 1 (Ref) | 373 | 1.80 (1.48, 2.19) | 415 | 3.03 (2.49, 3.70) | <0.001 |
| Adjusted 1 c | 1 | 1.42 (1.14, 1.78) | 1.35 (1.08, 1.69) | 0.007 | |||
| Adjusted 2 d | 1 | 1.39 (1.09, 1.76) | 1.27 (1.00, 1.62) | 0.04 | |||
| Femoral neck osteopenia + osteoporosis | |||||||
| Crude | 648 | 1 | 720 | 1.50 (1.21, 1.84) | 778 | 2.25 (1.80, 2.82) | <0.001 |
| Adjusted 1 | 1 | 1.23 (0.97, 1.55) | 1.53 (1.19, 1.96) | 0.11 | |||
| Adjusted 2 | 1 | 1.18 (0.93, 1.49) | 1.43 (1.10, 1.86) | 0.007 | |||
| Lumbar-spine osteopenia + osteoporosis | |||||||
| Crude | 663 | 1 | 712 | 1.32 (1.07, 1.62) | 751 | 1.70 (1.37, 2.12) | <0.001 |
| Adjusted 1 | 1 | 1.11 (0.89, 1.38) | 1.21 (0.96, 1.53) | 0.001 | |||
| Adjusted 2 | 1 | 1.03 (0.82, 1.29) | 1.11 (0.87, 1.49) | 0.42 | |||
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Na, W.; Park, S.; Shivappa, N.; Hébert, J.R.; Kim, M.K.; Sohn, C. Association between Inflammatory Potential of Diet and Bone-Mineral Density in Korean Postmenopausal Women: Data from Fourth and Fifth Korea National Health and Nutrition Examination Surveys. Nutrients 2019, 11, 885. https://doi.org/10.3390/nu11040885
Na W, Park S, Shivappa N, Hébert JR, Kim MK, Sohn C. Association between Inflammatory Potential of Diet and Bone-Mineral Density in Korean Postmenopausal Women: Data from Fourth and Fifth Korea National Health and Nutrition Examination Surveys. Nutrients. 2019; 11(4):885. https://doi.org/10.3390/nu11040885
Chicago/Turabian StyleNa, Woori, Susan Park, Nitin Shivappa, James R. Hébert, Mi Kyung Kim, and Cheongmin Sohn. 2019. "Association between Inflammatory Potential of Diet and Bone-Mineral Density in Korean Postmenopausal Women: Data from Fourth and Fifth Korea National Health and Nutrition Examination Surveys" Nutrients 11, no. 4: 885. https://doi.org/10.3390/nu11040885