
Probiotics for the Prevention of Ventilator-Associated Pneumonia: An Updated Systematic Review and Meta-Analysis of Randomised Controlled Trials

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Sources and Searches
2.2. Eligibility Criteria
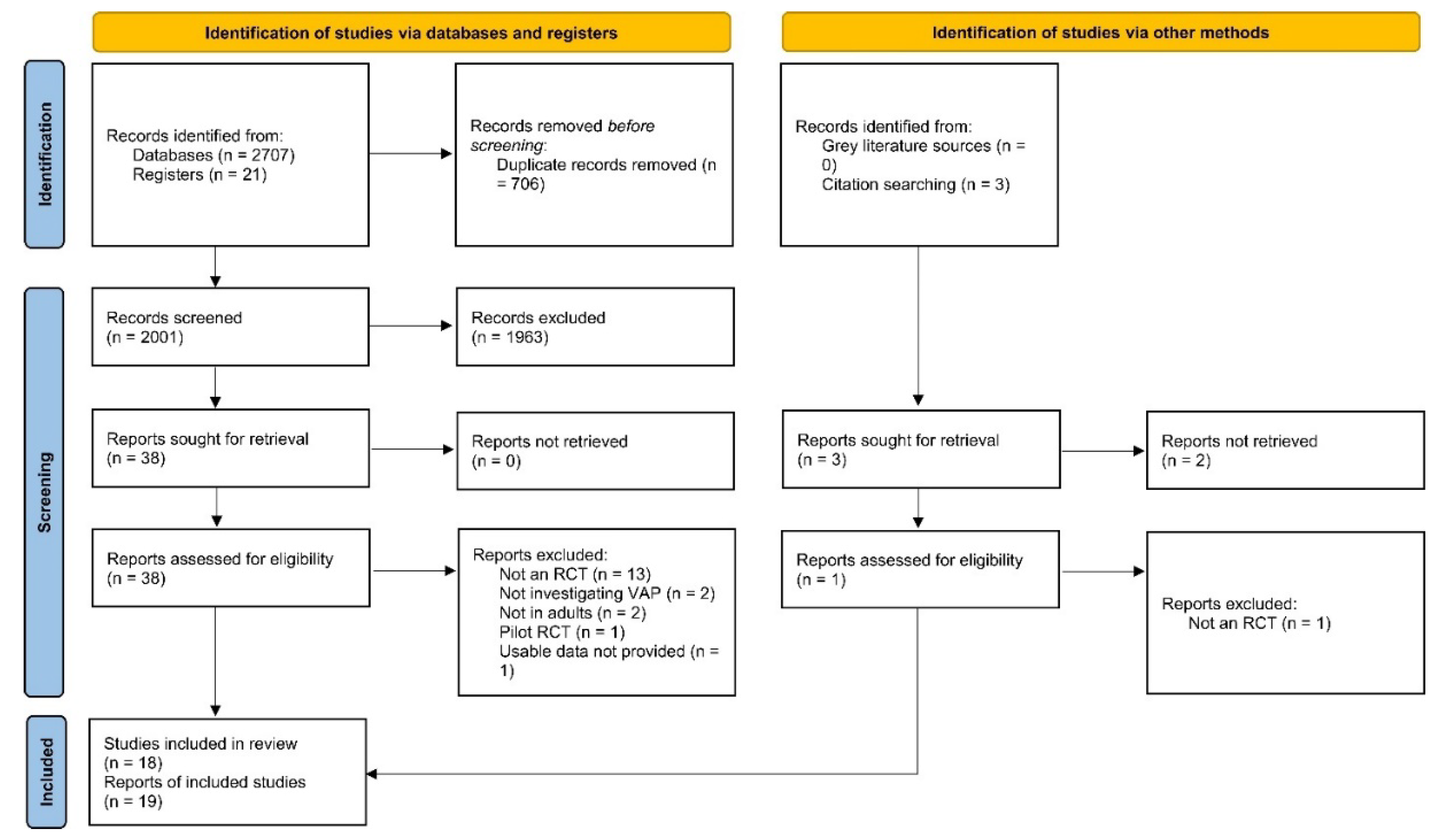
2.3. Study Selection and Data Abstraction
2.4. Outcome Measures
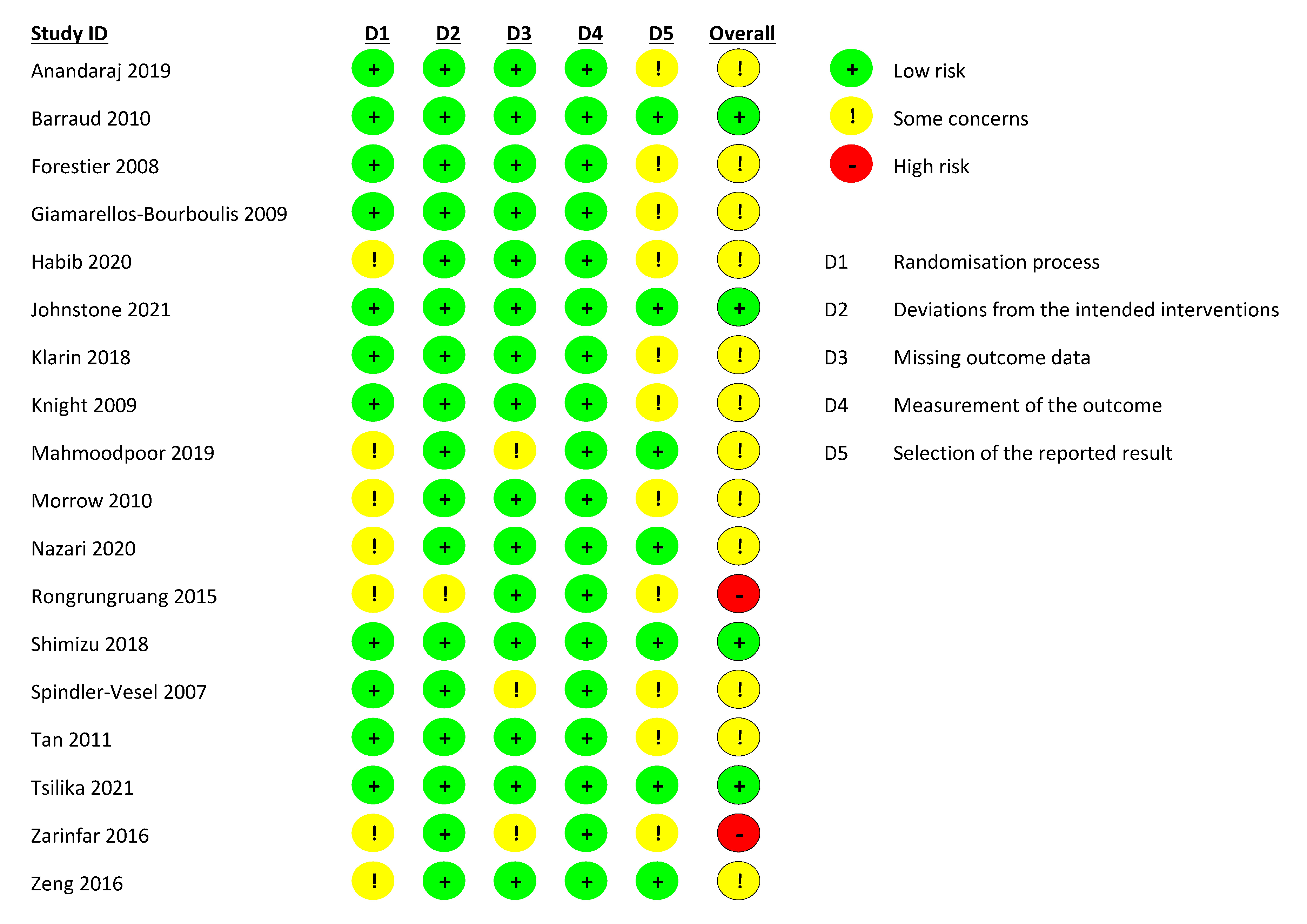
2.5. Risk of Bias Assessment
2.6. Data Synthesis
2.7. Subgroup and Sensitivity Analyses
2.8. Certainty of Evidence Assessment
3. Results
3.1. Risk of Bias in Included Studies
3.2. Effects of Interventions
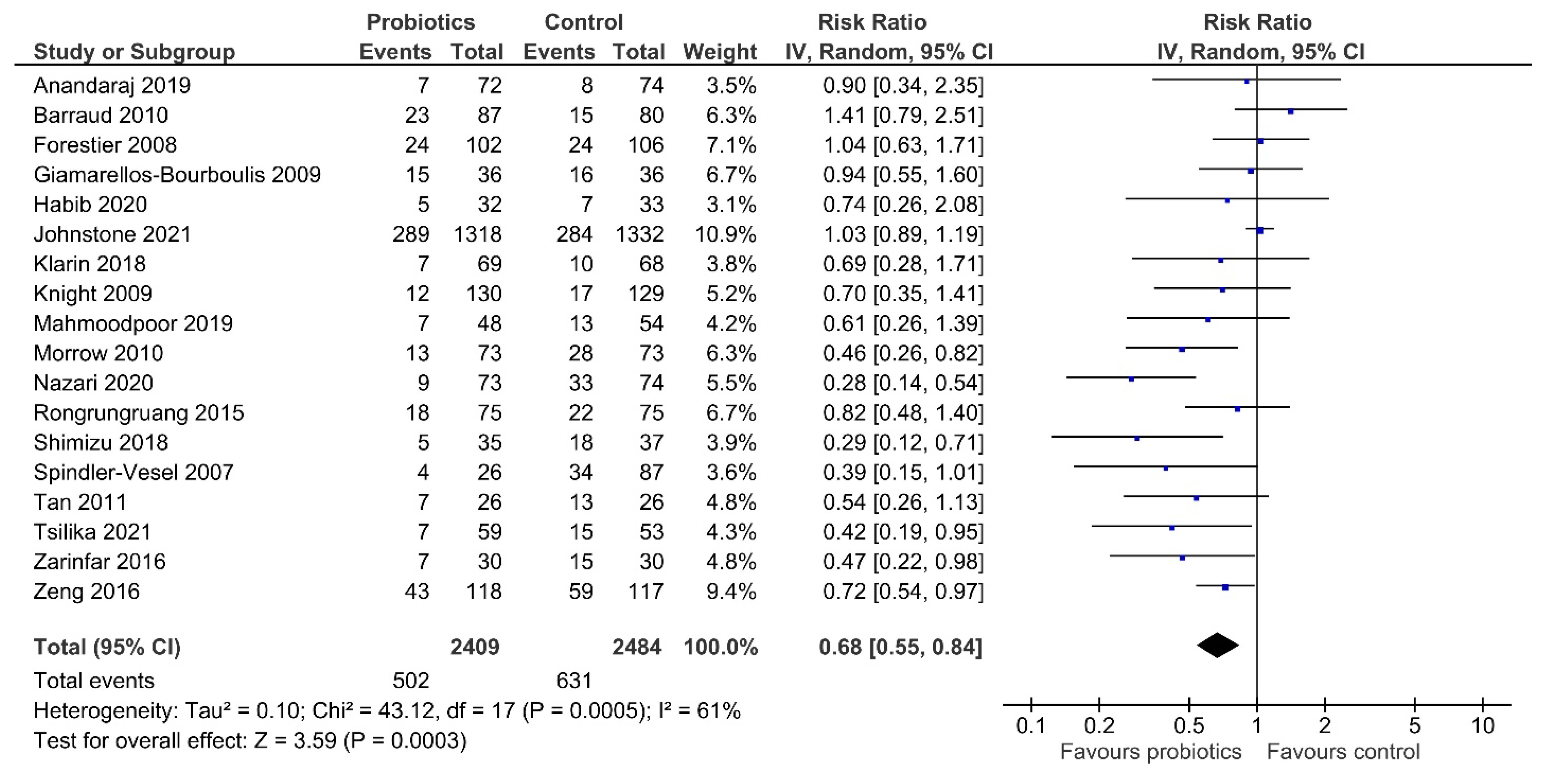
Primary Outcome: Incidence of VAP
4. Secondary Outcomes
4.1. Duration of Mechanical Ventilation
4.2. Length of ICU Stay
4.3. Length of Hospital Stay
4.4. ICU, Hospital and 28/30-Day Mortality
4.5. Duration of Antibiotic Use
4.6. Incidence of Diarrhoea
4.7. Any Adverse Effects of the Probiotics or Synbiotics
4.8. Subgroup Analysis
4.8.1. Blinding
4.8.2. Type of Intervention
4.8.3. Type of Comparator
4.8.4. Diagnostic Criteria for VAP
4.9. Sensitivity Analysis
5. Discussion
6. Strengths and Limitations
7. Implications for Practice and Research
8. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Papazian, L.; Klompas, M.; Luyt, C.E. Ventilator-associated pneumonia in adults: A narrative review. Intensiv. Care Med. 2020, 46, 888–906. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seguin, P.; Laviolle, B.; Dahyot-Fizelier, C.; Dumont, R.; Veber, B.; Gergaud, S.; Asehnoune, K.; Mimoz, O.; Donnio, P.Y.; Bellissant, E.; et al. Effect of oropharyngeal povidone-iodine preventive oral care on ventilator-associated pneumonia in severely brain-injured or cerebral hemorrhage patients: A multicenter, randomised controlled trial. Crit. Care Med. 2014, 42, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Reignier, J.; Mercier, E.; Le Gouge, A.; Boulain, T.; Desachy, A.; Bellec, F.; Clavel, M.; Frat, J.P.; Plantefeve, G.; Quenot, J.P.; et al. Effect of not monitoring residual gastric volume on risk of ventilator-associated pneumonia in adults receiving mechanical ventilation and early enteral feeding: A randomised controlled trial. JAMA 2013, 309, 249–256. [Google Scholar] [CrossRef] [PubMed]
- Torres, A.; Niederman, M.S.; Chastre, J.; Ewig, S.; Fernandez-Vandellos, P.; Hanberger, H.; Kollef, M.; Bassi, G.L.; Luna, C.M.; Martin-Loeches, I.; et al. International ERS/ESICM/ESCMID/ALAT guidelines for the management of hospital-acquired pneumonia and ventilator-associated pneumonia. Eur. Respir. J. 2017, 50, 1700582. [Google Scholar] [CrossRef]
- Walker, W.A. Mechanisms of action of probiotics. Clin. Infect. Dis. 2008, 46 (Suppl. S2), S87–S91. [Google Scholar] [CrossRef]
- Isolauri, E.; Sütas, Y.; Kankaanpää, P.; Arvilommi, H.; Salminen, S. Probiotics: Effects on immunity. Am. J. Clin. Nutr. 2001, 73 (Suppl. S2), 444s–450s. [Google Scholar] [CrossRef] [Green Version]
- van der Kleij, D.; Latz, E.; Brouwers, J.F.; Kruize, Y.C.; Schmitz, M.; Kurt-Jones, E.A.; Espevik, T.; de Jong, E.C.; Kapsenberg, M.L.; Golenbock, D.T.; et al. A novel host-parasite lipid cross-talk. Schistosomal lyso-phosphatidylserine activates toll-like receptor 2 and affects immune polarisation. J. Biol. Chem. 2002, 277, 48122–48129. [Google Scholar] [CrossRef] [Green Version]
- Chapat, L.; Chemin, K.; Dubois, B.; Bourdet-Sicard, R.; Kaiserlian, D. Lactobacillus casei reduces CD8+ T cell-mediated skin inflammation. Eur. J. Immunol. 2004, 34, 2520–2528. [Google Scholar] [CrossRef]
- Manley, K.J.; Fraenkel, M.B.; Mayall, B.C.; Power, D.A. Probiotic treatment of vancomycin-resistant enterococci: A randomised controlled trial. Med. J. Aust. 2007, 186, 454–457. [Google Scholar] [CrossRef]
- Morrow, L.E.; Kollef, M.H.; Casale, T.B. Probiotic Prophylaxis of Ventilator-associated Pneumonia. Am. J. Respir. Crit. Care Med. 2010, 182, 1058–1064. [Google Scholar] [CrossRef] [Green Version]
- Nazari, B.; Amani, L.; Ghaderi, L.; Gol, M.K. Effects of Probiotics on Prevalence of Ventilator-Associated Pneumonia in Multitrauma Patients Hospitalised in Neurosurgical Intensive Care Unit: A Randomised Clinical Trial. Trauma Mon. 2020, 25, 262–268. [Google Scholar]
- Ji, T.; Zhu, X.; Shang, F.; Zhang, X. Preventive Effect of Probiotics on Ventilator-Associated Pneumonia: A Meta-analysis of 2428 Patients. Ann. Pharmacother. 2021, 55, 949–962. [Google Scholar] [CrossRef] [PubMed]
- Su, M.; Jia, Y.; Li, Y.; Zhou, D.; Jia, J. Probiotics for the Prevention of Ventilator-Associated Pneumonia: A Meta-Analysis of Randomised Controlled Trials. Respir. Care 2020, 65, 673–685. [Google Scholar] [CrossRef] [PubMed]
- Batra, P.; Soni, K.D.; Mathur, P. Efficacy of probiotics in the prevention of VAP in critically ill ICU patients: An updated systematic review and meta-analysis of randomised control trials. J. Intensiv. Care 2020, 8, 81. [Google Scholar] [CrossRef]
- Johnstone, J.; Meade, M.; Lauzier, F.; Marshall, J.; Duan, E.; Dionne, J.; Arabi, Y.M.; Heels-Ansdell, D.; Thabane, L.; Lamarche, D.; et al. Effect of Probiotics on Incident Ventilator-Associated Pneumonia in Critically Ill Patients. JAMA 2021, 326, 1024–1033. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley Blackwell: Hoboken, NJ, USA, 2019. [Google Scholar]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Syst. Rev. 2021, 10, 89. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- Wan, X.; Wang, W.; Liu, J.; Tong, T. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med. Res. Methodol. 2014, 14, 135. [Google Scholar] [CrossRef] [Green Version]
- Viechtbauer, W. Conducting Meta-Analyses in R with the metafor Package. J. Stat. Softw. 2010, 36, 1–48. [Google Scholar] [CrossRef] [Green Version]
- Furuya-Kanamori, L.; Barendregt, J.J.; Doi, S.A.R. A new improved graphical and quantitative method for detecting bias in meta-analysis. Int. J. Evid. Based Healthc. 2018, 16, 195–203. [Google Scholar] [CrossRef]
- Richardson, M.; Garner, P.; Donegan, S. Interpretation of subgroup analyses in systematic reviews: A tutorial. Clin. Epidemiol. Glob. Heal. 2018, 7, 192–198. [Google Scholar] [CrossRef] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924–926. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Schünemann, H.J. GRADE: What is “quality of evidence” and why is it important to clinicians? BMJ 2008, 336, 995–998. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Brozek, J.; Alonso-Coello, P.; Rind, D.; Devereaux, P.J.; Montori, V.M.; Freyschuss, B.; Vist, G.; et al. GRADE guidelines 6. Rating the quality of evidence—imprecision. J. Clin. Epidemiol. 2011, 64, 1283–1293. [Google Scholar] [CrossRef]
- Mahmoodpoor, A.; Hamishehkar, H.; Asghari, R.; Abri, R.; Shadvar, K.; Sanaie, S. Effect of a Probiotic Preparation on Ventilator-Associated Pneumonia in Critically Ill Patients Admitted to the Intensive Care Unit: A Prospective Double-Blind Randomised Controlled Trial. Nutr. Clin. Pract. 2019, 34, 156–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rongrungruang, Y.; Krajangwittaya, D.; Thamlikitkul, V.; Pholtawornkulchai, K.; Tiengrim, S. Randomised controlled study of probiotics containing Lactobacillus casei (Shirota strain) for prevention of ventilator-associated pneumonia. J. Med. Assoc. Thail. 2015, 98, 253–259. [Google Scholar]
- Shimizu, K.; Yamada, T.; Ogura, H.; Mohri, T.; Kiguchi, T.; Fujimi, S.; Asahara, T.; Yamada, T.; Ojima, M.; Ikeda, M.; et al. Synbiotics modulate gut microbiota and reduce enteritis and ventilator-associated pneumonia in patients with sepsis: A randomised controlled trial. Crit. Care 2018, 22, 239. [Google Scholar] [CrossRef] [Green Version]
- Spindler-Vesel, A.; Bengmark, S.; Vovk, I.; Cerovic, O.; Kompan, L. Synbiotics, Prebiotics, Glutamine, or Peptide in Early Enteral Nutrition: A Randomised Study in Trauma Patients. J. Parenter. Enteral Nutr. 2007, 31, 119–126. [Google Scholar] [CrossRef]
- Tan, M.; Zhu, J.-C.; Du, J.; Zhang, L.-M.; Yin, H.-H. Effects of probiotics on serum levels of Th1/Th2 cytokine and clinical outcomes in severe traumatic brain-injured patients: A prospective randomised pilot study. Crit. Care. 2011, 15, R290. [Google Scholar] [CrossRef] [Green Version]
- Tsilika, M.; Thoma, G.; Aidoni, Z.; Tsaousi, G.; Fotiadis, K.; Stavrou, G.; Malliou, P.; Chorti, A.; Massa, H.; Antypa, E.; et al. A four-probiotic preparation for ventilator-associated pneumonia in multi-trauma patients: Results of a randomised clinical trial. Int. J. Antimicrob. Agents 2021, 59, 106471. [Google Scholar] [CrossRef]
- Zarinfar, N.; Sharafkhah, M.; Amiri, M.; Rafeie, M. Probiotic effects in prevention from ventilator-associated pneumonia. Koomesh 2016, 17, 803–813. [Google Scholar]
- Zeng, J.; Wang, C.T.; Zhang, F.S.; Qi, F.; Wang, S.F.; Ma, S.; Wu, T.J.; Tian, H.; Tian, Z.T.; Zhang, S.L.; et al. Effect of probiotics on the incidence of ventilator-associated pneumonia in critically ill patients: A randomised controlled multicenter trial. Intensiv. Care Med. 2016, 42, 1018–1028. [Google Scholar] [CrossRef]
- Forestier, C.; Guelon, D.; Cluytens, V.; Gillart, T.; Sirot, J.; De Champs, C. Oral probiotic and prevention of Pseudomonas aeruginosa infections: A randomised, double-blind, placebo-controlled pilot study in intensive care unit patients. Crit. Care 2008, 12, R69. [Google Scholar] [CrossRef] [Green Version]
- Anandaraj, A.M.; Pichamuthu, K.K.; Hansdak, S.G.; Samuel, P.; Irodi, A.; Valsa, S.; Peter, J.V. A Randomised Controlled Trial of Lactobacillus in the Prevention of Ventilator Associated Pneumonia. J. Clin. Diagn. Res. 2019, 13, 1–4. [Google Scholar] [CrossRef]
- Barraud, D.; Blard, C.; Hein, F.; Marçon, O.; Cravoisy, A.; Nace, L.; Alla, F.; Bollaert, P.-E.; Gibot, S. Probiotics in the critically ill patient: A double blind, randomised, placebo-controlled trial. Intensiv. Care Med. 2010, 36, 1540–1547. [Google Scholar] [CrossRef]
- Giamarellos-Bourboulis, E.J.; Bengmark, S.; Kanellakopoulou, K.; Kotzampassi, K. Pro- and Synbiotics to Control Inflammation and Infection in Patients With Multiple Injuries. J. Trauma Inj. Infect. Crit. Care 2009, 67, 815–821. [Google Scholar] [CrossRef] [Green Version]
- Kotzampassi, K.; Giamarellos-Bourboulis, E.J.; Voudouris, A.; Kazamias, P.; Eleftheriadis, E. Benefits of a Synbiotic Formula (Synbiotic 2000Forte®) in Critically Ill Trauma Patients: Early Results of a Randomised Controlled Trial. World J. Surg. 2006, 30, 1848–1855. [Google Scholar] [CrossRef]
- Habib, T.; Kassem, A.B.; Ahmed, I. Early probiotics in preventing ventilator-associated pneumonia after multiple trauma. Asian J. Pharm. Clin. Res. 2020, 83–85. [Google Scholar] [CrossRef]
- Klarin, B.; Adolfsson, A.; Torstensson, A.; Larsson, A. Can probiotics be an alternative to chlorhexidine for oral care in the mechanically ventilated patient? A multicentre, prospective, randomised controlled open trial. Crit. Care 2018, 22, 272. [Google Scholar] [CrossRef] [Green Version]
- Knight, D.J.W.; Gardiner, D.; Banks, A.; Snape, S.E.; Weston, V.C.; Bengmark, S.; Girling, K.J. Effect of synbiotic therapy on the incidence of ventilator associated pneumonia in critically ill patients: A randomised, double-blind, placebo-controlled trial. Intensiv. Care Med. 2008, 35, 854–861. [Google Scholar] [CrossRef]
- Bo, L.; Li, J.; Tao, T.; Bai, Y.; Ye, X.; Hotchkiss, R.S.; Kollef, M.H.; Crooks, N.H.; Deng, X. Probiotics for preventing ventilator-associated pneumonia. Cochrane Database Syst. Rev. 2014, CD009066. [Google Scholar] [CrossRef]
- Song, H.; Hu, W.; Zhou, X.; Tao, J.; Zhang, S.; Su, X.; Wu, W. Clinical Benefits From Administering Probiotics to Mechanical Ventilated Patients in Intensive Care Unit: A PRISMA-Guided Meta-Analysis. Front. Nutr. 2022, 8, 798827. [Google Scholar] [CrossRef]
- Zhang, Z.; Xu, X.; Ni, H. Small studies may overestimate the effect sizes in critical care meta-analyses: A meta-epidemiological study. Crit. Care 2013, 17, R2. [Google Scholar] [CrossRef] [Green Version]
- Sivakumar, H.; Peyton, P.J. Poor agreement in significant findings between meta-analyses and subsequent large randomised trials in perioperative medicine. Br. J. Anaesth. 2016, 117, 431–441. [Google Scholar] [CrossRef] [Green Version]
- Pildal, J.; Hróbjartsson, A.; Jørgensen, K.J.; Hilden, J.; Altman, D.G.; Gøtzsche, P.C. Impact of allocation concealment on conclusions drawn from meta-analyses of randomised trials. Int. J. Epidemiol. 2007, 36, 847–857. [Google Scholar] [CrossRef]
- Li, C.; Liu, L.; Gao, Z.; Zhang, J.; Chen, H.; Ma, S.; Liu, A.; Mo, M.; Wu, C.; Chen, D.; et al. Synbiotic Therapy Prevents Nosocomial Infection in Critically Ill Adult Patients: A Systematic Review and Network Meta-Analysis of Randomised Controlled Trials Based on a Bayesian Framework. Front. Med. 2021, 8, 693188. [Google Scholar] [CrossRef]
- Pun, B.T.; Balas, M.C.; Barnes-Daly, M.A.; Thompson, J.L.; Aldrich, J.M.; Barr, J.; Byrum, D.; Carson, S.S.; Devlin, J.W.; Engel, H.J.; et al. Caring for Critically Ill Patients with the ABCDEF Bundle. Crit. Care Med. 2019, 47, 3–14. [Google Scholar] [CrossRef]
- Pugh, R.; Harrison, W.; Harris, S.; Roberts, H.; Scholey, G.; Szakmany, T.; The WICSARG Investigators and WHAIP; Battle, C.; Brown, C.; Curtis, E.; et al. Is HELICS the Right Way? Lack of Chest Radiography Limits Ventilator-Associated Pneumonia Surveillance in Wales. Front. Microbiol. 2016, 7, 1271. [Google Scholar] [CrossRef] [Green Version]
- Klompas, M. Ventilator-Associated Events: What They Are and What They Are Not. Respir. Care 2019, 64, 953–961. [Google Scholar] [CrossRef]
- Walsh, T.S.; Morris, A.C.; Simpson, A.J.V. Ventilator associated pneumonia: Can we ensure that a quality indicator does not become a game of chance? BJA Br. J. Anaesth. 2013, 111, 333–337. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Study ID (First Author, Year) | Country of Origin | Trial Design | Study Follow-Up Duration | No. of Patients (Total [Probiotic Group vs. Control]) * | Age (Years) *† | Male (%) * | Disease Types | Method of Administration | Experimental Intervention | Comparator Intervention | Diagnostic Criteria for VAP |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Spindler-Vesel and colleagues, 2007 [36] | Solvenia | SC, SB | ICU stay | 113 (26 vs. 87) | 45.8 ± 22.9 vs. 37.1 ± 36.4 | 77.9 (total) | Multi trauma | Intragastric tube | Synbiotic 2000 FORTE | Group A: glutamine; Group B: fermentable fibres; Group C: peptide diet | Inexplicable |
| Forestier and colleagues, 2008 [41] | France | SC, DB | ICU stay | 208 (102 vs. 106) | 60 (18–91) vs. 57 (18–80) | 63.7 vs. 76.4 | Multidisease and trauma | Nasogastric tube/oral | L. casei rhamnosus (109), bid | Placebo (growth medium without bacteria), bid | Microbiologically confirmed |
| Giamarellos-Bourboulis and colleagues, 2009 [28,29] | Greece | MC, DB | 28 days | 72 (36 vs. 36) | 52.9 ± 19.0 vs. 55.9 ± 18.0 | NA | Multi trauma | Nasogastric tube/gastrostomy | Synbiotic 2000 FORTE, qd | Placebo | Clinically diagnosed |
| Knight and colleagues, 2009 [32] | UK | SC, DB | Hospital stay | 259 (130 vs. 129) | 49.5 ± 19.6 vs. 50.0 ± 18.5 | 62.3 vs. 62.0 | Multi-disease | Nasogastric/orogastric tube | Synbiotic 2000 FORTE, bid | Crystalline cellulose-based placebo | Microbiologically confirmed |
| Barraud and colleagues, 2010 [27] | France | SC, DB | 90 days | 167 (87 vs. 80) | 59.1 ± 15.9 vs. 61.8 ± 15.5 | 86.8 vs. 79.5 | Multi-disease | Enteral feeding tube | Ergyphilus capsules | Placebo | Microbiologically confirmed |
| Morrow and colleagues, 2010 [10] | Nebraska | SC, DB | 25 days | 138 (68 vs. 70) | 52.5 ± 19.3 vs. 54.6 ± 16.3 | 58.9 vs. 58.9 | Multi-disease and Trauma | Slurry to oropharynx/Nasogastric tube | Lactobacillus rhamnosus GG, bid | Plant starch inulin | Microbiologically confirmed |
| Tan and colleagues, 2011 [37] | China | SC, SB | 21 days | 52 (26 vs. 26) | 40.5 ± 13.0 vs. 40.8 ± 12.8 | 73.1 vs. 80.8 | Severe traumatic brain-injured | nasogastric tube/oral | Golden bifid 7 sachets, tid | Placebo | Microbiologically confirmed |
| Rongrungruang and colleagues, 2015 [34] | Thailand | SC, OP | 90 days | 150 (75 vs. 75) | 73.1 ± 13.2 vs. 69.0 ± 18.5 | 40.0 vs. 42.7 | Multi-disease | Oral care and enteral feeding tube | Lactobacillus, 80 mL, oral care, qd, 80 mL, enteral feeding, qd | Placebo | Clinically diagnosed |
| Zarinfar and colleagues, 2016 [39] | Iran | SC, DB | NA | 60 (30 vs. 30) | 41.4 ± 18.8 vs. 48.2 ± 18.9 | 70.0 vs. 66.7 | Multi-disease | Slurry to oropharynx | Lactobacillus rhamnosus GG, 3 × 109 CFU, tid | Placebo | Clinically diagnosed |
| Zeng and colleagues, 2016 [40] | China | MC, OP | 14 days | 235 (118 vs. 117) | 50.2 ± 18.2 vs. 54.6 ± 17.9 | 61.9 vs. 55.6 | Multi-disease | nasogastric tube | Probiotics capsule containing live Bacillus subtilis and Enterococcus faecalis (Medilac-S) 0.5 g three times daily plus standard preventive strategies | Standard preventive strategies | Microbiologically confirmed |
| Klarin and colleagues, 2018 [31] | Sweden | MC, OP | 180 days | 137 (69 vs. 68) | 66 (57–76) vs. 65.5 (53.75–75) | 58.0 vs. 52.9 | Multi-Disease | Oral care | Lactobacillus plantarum 299, 1010 CFU, bid | standard 0.1% CHX solution plus toothpaste | Clinically diagnosed |
| Shimizu and colleagues, 2018 [35] | Japan | SC, SB | 28 days | 72 (35 vs. 37) | 74 (64–82) vs. 74 (64–81) | 71.4 vs. 59.5 | Sepsis | Nasogastric tube/orally | Synbiotics: Seichoyaku, 3 g and galactooligosaccharides 10 g, qd | No treatment | Inexplicable |
| Anandaraj and colleagues, 2019 [26] | India | SC, DB | ICU stay | 146 (72 vs. 74) | 42.0 ± 17.0 vs. 43.0 ± 17.0 | 60.0 vs. 57.0 | Multi-disease | Oral slurry/nasogastric | Lactobacillus 2 × 109 CFU, bid | Inert Powder | Clinically diagnosed |
| Mahmoodpoor and colleagues, 2019 [33] | Iran | MC, DB | 14 days | 100 (48 vs. 52) | 59.1 ± 12.9 vs. 57.5 ± 14.5 | 54.2 vs. 53.7 | Multi-disease | Nasogastric tube | LactoCare capsule (synbiotic), bid | Placebo (sterile maize starch) | Microbiologically confirmed |
| Habib and colleagues, 2020 [30] | Egypt | SC, DB | ICU stay | 65 (32 vs. 33) | 39.5 ± 7.7 (total) | 80.0 (total) | Multi trauma | Orogastric/nasogastric tube | Lacteol Forte Sachet, tid | Placebo sachet | Inexplicable |
| Nazari and colleagues, 2020 [11] | Iran | MC, SB | ICU stay | 147 (73 vs. 74) | 52.2 ± 4.1 vs. 53.0 ± 4.0 | 67.1 vs. 70.3 | Multi-trauma | Nasogastric tube | LactoCare capsule (synbiotic), bid | Starch | Clinically diagnosed |
| Johnstone and colleagues, 2021 [15] | Canada, USA, Saudi Arabia | MC, DB | Hospital stay | 2650 (1318 vs. 1332) | 60.1 ± 16.2 vs. 59.6 ± 16.8 | 59.0 vs. 60.8 | Multi-disease | Nasogastric/orogastric/nasoduodenal/oroduodenal tube | Lactobacillus rhamnosus GG, 1010 CFU, bid | Microcrystalline cellulose | Clinically diagnosed |
| Tsilika and colleagues, 2021 [38] | Greece | MC, DB | 30 days | 112 (59 vs. 53) | 38.1 ± 17.2 vs. 43.8 ± 14.4 | 91.5 vs. 75.5 | Multi-trauma | Nasogastric/gastrostomy tube | LactoLevure (a four-probiotic preparation), bid | Powdered glucose polymer | Microbiologically confirmed |
| Outcome | No. of Participants (Studies) | Effect Estimate (95% CI) | Risk Of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Quality of Evidence (GRADE) |
|---|---|---|---|---|---|---|---|---|
| VAP incidence | 4893 (18) | RR 0.68 (0.55–0.84) | Not serious | Serious | Not serious | Not serious | Suspected | ⊕⊕⊖⊖ LOW |
| Duration of mechanical ventilation (days) | 4182 (12) | MD −1.22 (−3.25–0.81) | Not serious | Serious | Not serious | Serious | Undetected | ⊕⊕⊖⊖ LOW |
| Length of ICU stay (days) | 4493 (15) | MD −2.22 (−4.17 to −0.28) | Not serious | Serious | Not serious | Not serious | Undetected | ⊕⊕⊕⊖ MODERATE |
| Length of hospital stay (days) | 3907 (9) | MD −1.47 (−4.06–1.12) | Not serious | Serious | Not serious | Serious | Suspected | ⊕⊖⊖⊖ VERY LOW |
| ICU mortality | 3872 (9) | RR 0.96 (0.85–1.09) | Not serious | Not serious | Not serious | Serious | Undetected | ⊕⊕⊕⊖ MODERATE |
| Hospital mortality | 3673 (8) | RR 0.94 (0.84–1.05) | Not serious | Not serious | Not serious | Serious | Suspected | ⊕⊕⊖⊖ LOW |
| 28/30-day mortality | 553 (5) | RR 0.94 (0.66–1.32) | Not serious | Not serious | Not serious | Serious | Suspected | ⊕⊕⊖⊖ LOW |
| Duration of antibiotic use (days) | 497 (4) | MD −1.25 (−1.86 to −0.64) | Not serious | Not serious | Not serious | Not serious | Suspected | ⊕⊕⊕⊖ MODERATE |
| Incidence of diarrhea | 3710 (9) | RR 0.98 (0.86–1.11) | Not serious | Not serious | Not serious | Not serious | Suspected | ⊕⊕⊕⊖ MODERATE |
| Subgroup | Incidence of VAP | Duration of Mechanical Ventilation (Days) | Length of ICU Stay (Days) | Length of Hospital Stay (Days) | |||||
|---|---|---|---|---|---|---|---|---|---|
| RR (95% CI) | p-Value for Subgroup Differences | MD (95% CI) | p-Value for Subgroup Differences | MD (95% CI) | p-Value for Subgroup Differences | MD (95% CI) | p-Value for Subgroup Differences | ||
| Trial Design | 0.002 | 0.45 | 0.58 | 0.90 | |||||
| Double-blind | 0.80 (0.63, 1.01) | −1.34 (−4.94, 2.25) | −2.83 (−6.49, 0.82) | −2.07 (−4.80, 0.65) | |||||
| Single-blind | 0.36 (0.24, 0.53) | 0.21 (−0.23, 0.65) | −1.65 (−2.56, −0.74) | Not estimable | |||||
| Open-label | 0.74 (0.58, 0.95) | −2.85 (−9.15, 3.45) | 3.03 (−8.05, 14.11) | −3.37 (−24.36, 17.62) | |||||
| Type of Intervention | 0.09 | 0.75 | 0.73 | 0.67 | |||||
| Probiotic | 0.77 (0.63, 0.96) | −1.43 (−5.63, 2.78) | −1.73 (−5.25, 1.80) | −0.73 (−2.97, 1.51) | |||||
| Synbiotic | 0.50 (0.32, 0.79) | −0.71 (−2.24, 0.82) | −2.45 (−4.50, −0.40) | −2.67 (−11.38, 6.04) | |||||
| Type of comparator | 0.55 | 0.96 | 0.47 | 0.90 | |||||
| Placebo | 0.71 (0.54, 0.94) | −1.12 (−3.41, 1.16) | −2.71 (−5.07, −0.34) | −2.07 (−4.80, 0.65) | |||||
| Others | 0.64 (0.49, 0.82) | −1.27 (−6.83, 4.28) | −0.95 (−5.09, 3.19) | −3.37 (−24.36, 17.62) | |||||
| Definition of VAP | 0.20 | NA | NA | NA | |||||
| Clinically undiagnosed | 0.71 (0.49, 1.02) | ||||||||
| Microbiologically confirmed | 0.72 (0.55, 0.94) | ||||||||
| Inexplicable diagnostic criteria | 0.42 (0.24, 0.72) | ||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheema, H.A.; Shahid, A.; Ayyan, M.; Mustafa, B.; Zahid, A.; Fatima, M.; Ehsan, M.; Athar, F.; Duric, N.; Szakmany, T. Probiotics for the Prevention of Ventilator-Associated Pneumonia: An Updated Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients 2022, 14, 1600. https://doi.org/10.3390/nu14081600
Cheema HA, Shahid A, Ayyan M, Mustafa B, Zahid A, Fatima M, Ehsan M, Athar F, Duric N, Szakmany T. Probiotics for the Prevention of Ventilator-Associated Pneumonia: An Updated Systematic Review and Meta-Analysis of Randomised Controlled Trials. Nutrients. 2022; 14(8):1600. https://doi.org/10.3390/nu14081600
Chicago/Turabian StyleCheema, Huzaifa Ahmad, Abia Shahid, Muhammad Ayyan, Biah Mustafa, Afra Zahid, Maurish Fatima, Muhammad Ehsan, Farwa Athar, Natalie Duric, and Tamas Szakmany. 2022. "Probiotics for the Prevention of Ventilator-Associated Pneumonia: An Updated Systematic Review and Meta-Analysis of Randomised Controlled Trials" Nutrients 14, no. 8: 1600. https://doi.org/10.3390/nu14081600