Poor Knowledge and Practices Related to Iodine Nutrition during Pregnancy and Lactation in Australian Women: Pre- and Post-Iodine Fortification

 ,
,  ,
,
Abstract
:1. Introduction
2. Experimental Section
3. Results

{kind=link}
{kind=link}
| Study (Year) | Survey (Year) | |||
|---|---|---|---|---|
| Pre-Fortification | Post-Fortification | |||
| Non-Pregnant [19] | Pregnant [13] | Lactating [23,24] | Pregnant | |
| (2007–2008) N = 76 | (2008) N = 139 | (2010) N = 60 | (2011) N = 147 | |
| Age | ||||
| Mean (SD) | 38.3 (10.6) | 28.4 (5.7) | 32 (3.9) | 28 (5.0) |
| Range | 19–56 | 16–45 | 23–39 | 16–40 |
| Highest Level of Education Attained | ||||
| Some High School | - | 17% | - | 23% |
| Completed High School (Year 12) | 13% | 30% | 13% | 19% |
| TAFE (Technical and further education or apprenticeship) | 21% | 31.00% | 17% | 32% |
| University Degree (Undergraduate Level) | 32% | 13% | 38% | 21% |
| University Degree (Postgraduate Level) | 35% | 9% | 32% | 6% |
| Trimester | ||||
| 1 (0–12 weeks) | - | 2% | - | 2% |
| 2 (13–24 weeks) | - | 13% | - | 37% |
| 3 (>25 weeks) | - | 85% | - | 61% |
| First Pregnancy/Birth | - | 41% | 88% | 46% |
| Intention to Breastfeed | - | 84% | All breastfeeding | 88% |
| Previous Miscarriage | - | 29% | - | 25% |
3.1. Supplement Use
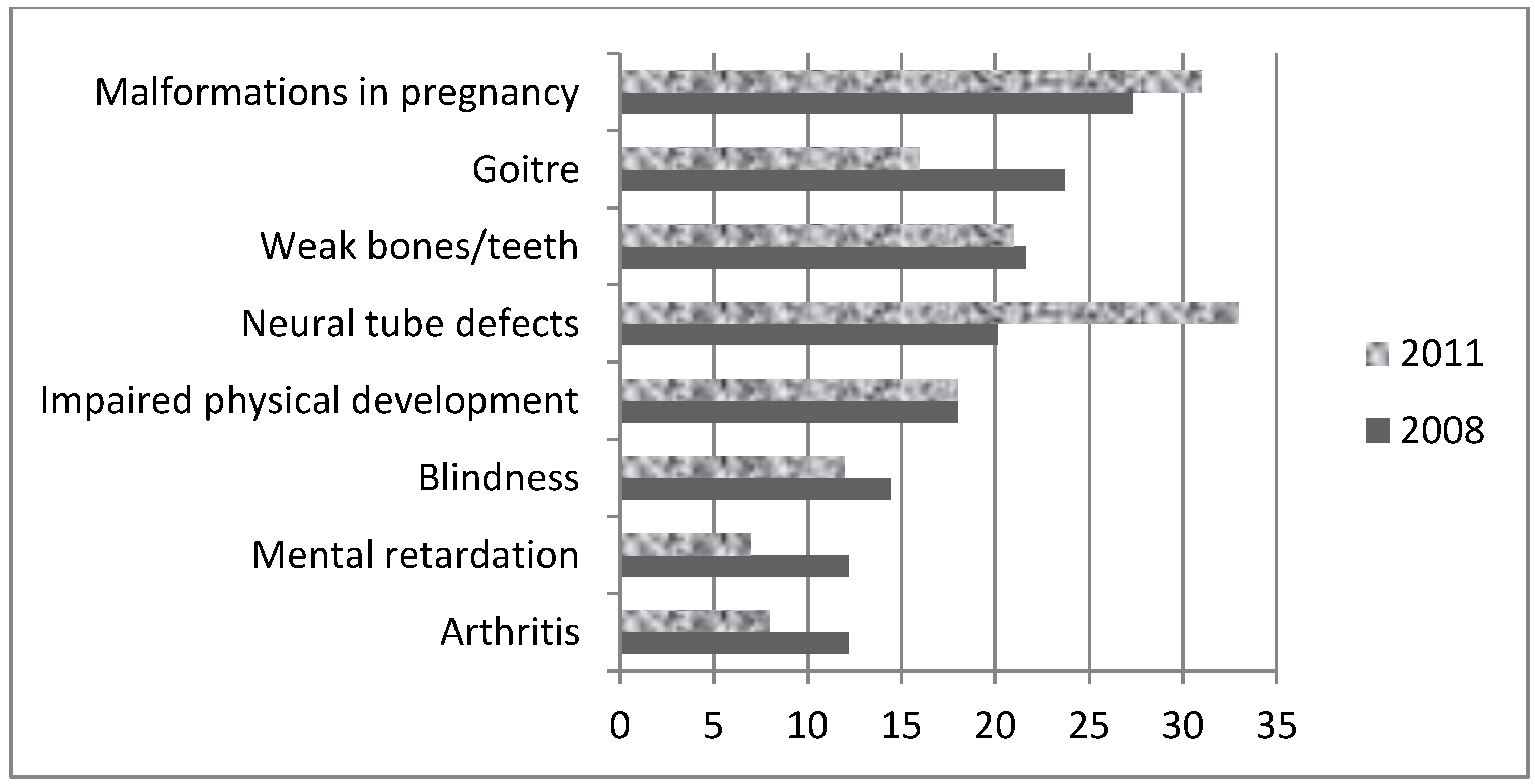
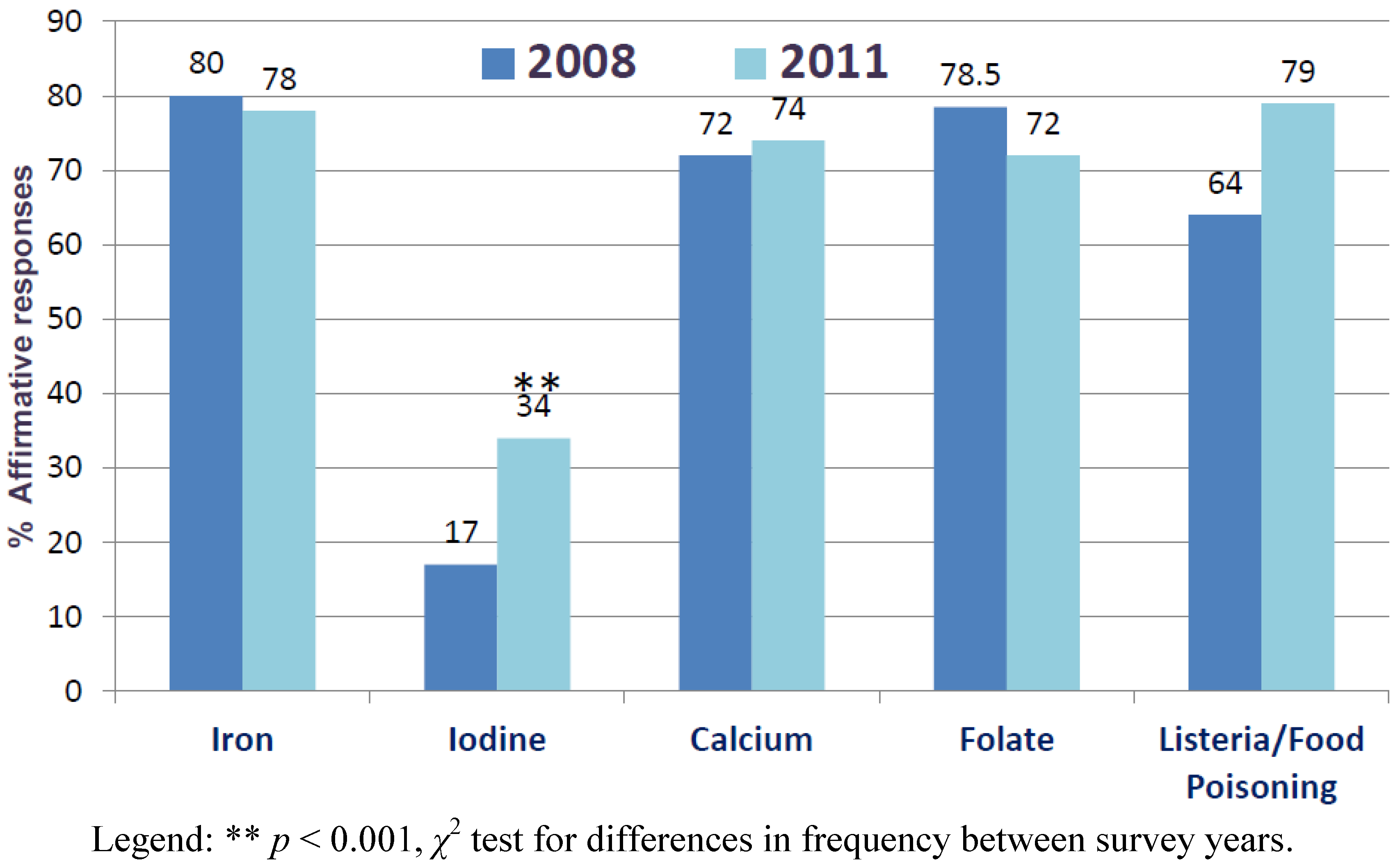
3.2. Knowledge
| Food Source | Good Source b | Do not know | ||
|---|---|---|---|---|
| Pre- ( n = 139) | Post- ( n = 145) | Pre- ( n = 139) | Post- ( n = 145) | |
| Meat | 49% | 50% | 48% | 48% |
| Milk* | 26% | 26% | 64% | 63% |
| Bread*,c | 18% | 27% | 72% | 61% |
| Fish and Seafood* | 58% | 50% | 39% | 43% |
| Fruit | 37% | 27% | 58% | 65% |
| Vegetables | 59% | 55% | 39% | 42% |
| Eggs* | 23% | 32% | 67% | 63% |
| Salt*,d | 52% | 51% | 36% | 40% |


| Source of Advice | Iron | Iodine | Calcium | Healthy Eating | Folate | Listeria and Food Poisoning |
|---|---|---|---|---|---|---|
| Healthcare Professional Advice (Verbal) | 72 | 53 | 81 | 101 | 75 | 99 |
| Healthcare Professional Advice (Written) | 48 | 18 | 31 | 52 | 51 | 43 |
| Newspaper | 3 | 1 | 2 | 3 | 3 | 4 |
| Magazine | 18 | 7 | 19 | 20 | 12 | 14 |
| Television | 7 | 1 | 7 | 7 | 7 | 4 |
| Radio | 0 | 0 | 1 | 0 | 1 | 0 |
| Internet | 23 | 11 | 16 | 27 | 19 | 32 |
| Did not receive any information | 24 | 51 | 26 | 8 | 20 | 16 |
3.3. Practices
| Total iodine intake (Mean ± SD) | Lactating (2010) [24] N = 60 | Pregnant (2011) N = 130 |
|---|---|---|
| EAR | 190 µg/day | 160 µg/day |
| With bread | 182 ± 63 μg/day | 211 ± 98 µg/day |
| Without bread | 146 ± 58 μg/day ** | 176 ± 92 µg/day * |
| % <EAR (with bread) | 60% | 35% |
4. Discussion
5. Conclusions
Acknowledgments
Conflict of Interest
References
- Glinoer, D. The importance of iodine nutrition during pregnancy. Public Health Nutr. 2007, 10, 1542–1546. [Google Scholar]
- Zimmermann, M.B.; Jooste, P.L.; Pandav, C.S. Iodine-deficiency disorders. Lancet 2008, 372, 1251–1262. [Google Scholar] [CrossRef]
- Simpson, J.L.; Bailey, L.B.; Pietrzik, K.; Shane, B.; Holzgreve, W. Micronutrients and women of reproductive potential: Required dietary intake and consequences of dietary deficienty or excess. Part II—Vitamin D, vitamin A, Iron, Zinc, Iodine, essential fatty acids. J. Matern. FetalNeonatal Med. 2011, 24, 1–24. [Google Scholar]
- Nutrient Reference Values for Australia and New Zealand Including Recommended Dietary Intakes. Available online: http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/n35.pdf (accessed on 25 August 2012).
- Bleichrodt, N.; Born, M.P. A Meta-Analysis of Research on Iodine and Its Relationship to Cognitive Development. In The Damaged Brain of Iodine Deficiency; Stanbury, J.B., Ed.; Cognizant Communication: New York, NY, USA, 1994; pp. 195–200. [Google Scholar]
- Qian, M.; Wang, D.; Watkins, W.E.; Gebski, V.; Yan, Y.Q.; Li, M.; Chen, Z.P. The effects of iodine on intelligence in children: A meta-analysis of studies conducted in China. Asia Pac. J. Clin. Nutr. 2005, 14, 32–42. [Google Scholar]
- Gordon, R.C.; Rose, M.C.; Skeaff, S.A.; Gray, A.R.; Morgan, K.M.D.; Ruffman, T. Iodine supplementation improves cognition in mildly iodine-deficient children. Am. J. Clin. Nutr. 2009, 90, 1264–1271. [Google Scholar] [CrossRef]
- Zimmermann, M.B. Iodine deficiency in industrialised countries. Clin. Endocrinol. (Oxf.) 2011, 75, 287–288. [Google Scholar] [CrossRef]
- Iodine Status Worldwide: WHO Global Database on Iodine Deficiency. Available online: http://whqlibdoc.who.int/publications/2004/9241592001.pdf (accessed on 25 August 2012).
- McDonnell, C.M.; Harris, M.; Zacharin, M.R. Iodine deficiency and goitre in schoolchildren in Melbourne, 2001. Med. J. Aust. 2003, 178, 159–162. [Google Scholar]
- Burgess, J.R.; Seal, J.A.; Stilwell, G.M.; Reynolds, P.J.; Taylor, E.R.; Parameswaran, V. A case for universal salt iodisation to correct iodine deficiency in pregnancy: Another salutary lesson from Tasmania. Med. J. Aust. 2007, 186, 574–576. [Google Scholar]
- Nguyen, B.; Baker, D.; Southcott, E.; Potter, J.; Sneddon, A.; Hickman, P.E. Iodine deficiency in pregnant women in the ACT. Aust. N. Z. J. Obstet. Gynaecol. 2010, 50, 539–542. [Google Scholar] [CrossRef]
- Charlton, K.E.; Gemming, L.; Yeatman, H.; Ma, G. Suboptimal iodine status of Australian pregnant women reflects poor knowledge and practices related to iodine nutrition. Nutrition 2010, 26, 963–968. [Google Scholar] [CrossRef]
- Hamrosi, M.A.; Wallace, E.M.; Riley, M.D. Iodine status in pregnant women living in Melbourne differs by ethnic group. Asia Pac. J. Clin. Nutr. 2005, 14, 27–31. [Google Scholar]
- Charlton, K.; Skeaff, S. Iodine fortification: Why, when, what, how, and who? Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 618–624. [Google Scholar] [CrossRef]
- Proposal P1003. Mandatory Iodine Fortification for Australia Approval Report. Available online: http://www.foodstandards.gov.au/_srcfiles/AppR_P1003_Mandatory_Iodine_Fortification_Aust%20AppR.pdf (accessed on 26 August 2012).
- Li, M.; Chapman, S.; Agho, K.; Eastman, C.J. Can even minimal news coverage influence consumer health-related behaviour? A case study of iodized salt sales, Australia. Health Educ. Res. 2008, 23, 543–548. [Google Scholar] [CrossRef]
- Eastman, C.J. Where has all our iodine gone? Med. J. Aust. 1999, 171, 455–456. [Google Scholar]
- Charlton, K.E.; Yeatman, H.R.; Houweling, F. Poor iodine status and knowledge related to iodine on the eve of mandatory iodine fortification in Australia. Asia Pac. J. Clin. Nutr. 2010, 19, 250–255. [Google Scholar]
- Australian Government, Cereals and Cereal Products. In Australia New Zealand Food Standard Code, Standard 2.1.1; ComLaw: Canberra, Australia, 2009.
- Iodine Supplementation during Pregnancy and Lactation. Available online: http://www.nhmrc.gov.au/_files_nhmrc/publications/attachments/new45_literature_review.pdf (accessed on 26 August 2012).
- Charlton, K.E.; Yeatman, H.; Ma, G. Has Iodine Status Improved in Australian Women Following Mandatory Iodine Fortification Introduction? In Program & Abstract Book: Public Health Association Australia 2nd National Food Futures Conference; Public Health Association of Australia Inc.: Curtin, Australia, 2011; p. 29. [Google Scholar]
- Axford, S.; Charlton, K.; Yeatman, H.; Ma, G. Improved iodine status in breastfeeding women following mandatory fortification. Aust. N. Z. J. Public Health 2011, 35, 579–580. [Google Scholar] [CrossRef]
- Axford, S.; Charlton, K.; Yeatman, H.; Ma, G. Poor knowledge and dietary practices related to iodine in breastfeeding mothers a year after introduction of mandatory fortification. Nutr. Diet. 2012, 69, 91–94. [Google Scholar] [CrossRef]
- Tan, L.; Charlton, K.E.; Ma, G.; Batterham, M. Validation of an iodine-specific Food Frequency Questionnaire to estimate dietary iodine intake in older Australians. Nutr. Diet. 2012. [Google Scholar] [CrossRef]
- Food Standards Australia New Zealand, Australian Food, Supplement & Nutrient Database 2007 for Estimation of Population Nutrient Intakes; FSANZ: Canberra, Australia, 2007.
- Thurlow, S. Questionnaire Assessing Public Opinion of Proposed Iodine Fortification Strategies; University of Otago: Dunedin, New Zealand, 2006. [Google Scholar]
- Jooste, P.L.; Upson, N.; Charlton, K.E. Knowledge of iodine nutrition in the South African adult population. Public Health Nutr. 2005, 8, 382–386. [Google Scholar]
- Food Standards Australia New Zealand, The 22nd Australian Total Diet Study; FSANZ: Canberra, Australia, 2008.
- Gallego, G.; Goodall, S.; Eastman, C.J. Iodine deficiency in Australia: Is iodine supplementation for pregnant and lactating women warranted? Med. J. Aust. 2010, 192, 461–463. [Google Scholar]
- Kamien, M. The repeating history of objections to the fortification of bread and alcohol: From iron filings to folic acid. Med. J. Aust. 2006, 184, 638–640. [Google Scholar]
- Sinikovic, D.S.; Yeatman, H.R.; Cameron, D.; Meyer, B.J. Women’s awareness of the importance of long-chain omega-3 polyunsaturated fatty acid consumption during pregnancy: Knowledge of risks, benefits and information accessibility. Public Health Nutr. 2009, 12, 562–569. [Google Scholar] [CrossRef]
- Oken, E.; Wright, R.O.; Kleinman, K.P.; Bellinger, D.; Amarasiriwardena, C.J.; Hu, H.; Rich-Edwards, J.W.; Gillman, M.W. Maternal fish consumption, hair mercury, and infant cognition in a U.S. cohort. Environ. Health Perspect. 2005, 113, 1376–1380. [Google Scholar] [CrossRef]
- Food Safety during Pregnancy. Available online: http://www.foodauthority.nsw.gov.au/_Documents/consumer_pdf/pregnancy-brochure.pdf (accessed on 25 August 2012).
- Mercury in Fish. Available online: http://www.foodstandards.gov.au/consumerinformation/mercuryinfish.cfm (accessed on 25 August 2012).
- Dietitians Association of Australia. Iodine. Available online: http://daa.asn.au/for-the-public/smart-eating-for-you/nutrition-a-z/iodine-2/ (accessed on 25 August 2012).
- Better Health Channel. Pregnancy and Diet. Available online: http://www.betterhealth.vic.gov.au/bhcv2/bhcarticles.nsf/pages/Pregnancy_and_diet (accessed on 25 August 2012).
- Diet and Pregnancy. Available online: http://www.healthinsite.gov.au/topics/Diet_and_Pregnancy (accessed on 25 August 2012).
© 2012 by the authors; licensee MDPI, Basel, Switzerland. This article is an open-access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Charlton, K.; Yeatman, H.; Lucas, C.; Axford, S.; Gemming, L.; Houweling, F.; Goodfellow, A.; Ma, G. Poor Knowledge and Practices Related to Iodine Nutrition during Pregnancy and Lactation in Australian Women: Pre- and Post-Iodine Fortification. Nutrients 2012, 4, 1317-1327. https://doi.org/10.3390/nu4091317
Charlton K, Yeatman H, Lucas C, Axford S, Gemming L, Houweling F, Goodfellow A, Ma G. Poor Knowledge and Practices Related to Iodine Nutrition during Pregnancy and Lactation in Australian Women: Pre- and Post-Iodine Fortification. Nutrients. 2012; 4(9):1317-1327. https://doi.org/10.3390/nu4091317
Chicago/Turabian StyleCharlton, Karen, Heather Yeatman, Catherine Lucas, Samantha Axford, Luke Gemming, Fiona Houweling, Alison Goodfellow, and Gary Ma. 2012. "Poor Knowledge and Practices Related to Iodine Nutrition during Pregnancy and Lactation in Australian Women: Pre- and Post-Iodine Fortification" Nutrients 4, no. 9: 1317-1327. https://doi.org/10.3390/nu4091317