Consumption of Sugar-Sweetened Beverages Is Associated with Components of the Metabolic Syndrome in Adolescents

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Data Collection
2.3. Anthropometric and Clinical Measurements
2.4. Definitions of Metabolic Syndrome
2.5. Statistical Analysis
3. Results

{kind=link}
| Factors | Girls | Boys | ||||||
|---|---|---|---|---|---|---|---|---|
| Nonintake | 1–500 | >500 | p 3 | Nonintake | 1-500 | >500 | p 3 | |
| Study subjects (no.) 1 | 196 | 961 | 242 | 120 | 802 | 406 | ||
| Population distribution 2 | ||||||||
| Consumer pattern (%) | 15.6 | 65.9 | 18.5 | 8.8 | 59.1 | 32.1 | ||
| Age, years (Mean ± SE) | 13.6 ± 0.1 | 13.5 ± 0.1 | 13.7 ± 0.1 | 0.574 | 13.6 ± 0.1 | 13.5 ± 0.1 | 13.7 ± 0.1 | 0.058 |
| Area (%) | ||||||||
| Kaohsiung city | 19.4 | 63.2 | 17.4 | 0.033 | 9.3 | 57.8 | 32.9 | 0.746 |
| Pingtung county | 10.6 | 68.3 | 21.2 | 7.7 | 60.6 | 31.7 | ||
| Taitung county | 11.0 | 74.2 | 14.8 | 9.2 | 62.8 | 28.0 | ||
| Physical activity, MET-min/week (%) | ||||||||
| <952.4 | 16.1 | 63.1 | 20.8 | 0.324 | 9.4 | 54.8 | 35.8 | 0.106 |
| 952.5–2140.4 | 16.7 | 68.0 | 15.3 | 11.5 | 55.8 | 32.7 | ||
| ≥2140.5 | 12.0 | 65.9 | 22.1 | 6.0 | 63.9 | 30.1 | ||
| Total calories, kcal/day (Mean ± SE) | 1835.3 ± 61.3 | 1903.4 ± 29.9 | 2044.8 ± 45.3 | <0.001 | 2083.7 ± 60.8 | 2151.5 ± 39.9 | 2448.2 ± 67.2 | <0.001 |
| Factors | Girls | Boys | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Nonintake | 1–500 | >500 | Nonintake | 1–500 | >500 | |||||||||||||
| aMean | SE | aMean | SE | aMean | SE | adj. β | SE | ptrend | aMean | SE | aMean | SE | aMean | SE | adj. β | SE | ptrend | |
| Waist circumference, cm | 68.0 | 0.9 | 69.4 | 0.7 | 71.1 * | 0.8 | 1.5 | 0.6 | 0.011 | 72.6 | 0.9 | 75.0 * | 0.6 | 76.3 * | 0.9 | 1.6 | 0.7 | 0.039 |
| HDL cholesterol, mg/dL | 58.8 | 1.3 | 59.0 | 1.2 | 57.6 | 1.6 | −0.6 | 0.9 | 0.528 | 56.0 | 1.3 | 56.3 | 0.7 | 54.9 | 1.6 | −0.9 | 1.0 | 0.401 |
| Triglyceride, mg/dL | 74.4 | 2.3 | 76.0 | 1.9 | 79.3 | 3.2 | 2.5 | 1.7 | 0.160 | 70.4 | 3.2 | 78.4 * | 1.6 | 78.6 * | 2.8 | 2.6 | 2.4 | 0.278 |
| Plasma glucose, mg/dL | 89.1 | 0.9 | 89.6 | 0.7 | 90.6 | 0.9 | 0.7 | 0.5 | 0.119 | 92.1 | 1.0 | 93.1 | 0.6 | 91.4 | 1.0 | −0.9 | 0.6 | 0.167 |
| SBP, mmHg | 106.2 | 1.3 | 106.5 | 0.6 | 107.7 | 1.2 | 0.8 | 0.6 | 0.174 | 111.9 | 1.3 | 112.2 | 0.9 | 114.3 | 0.6 | 1.6 | 0.7 | 0.043 |
| DBP, mmHg | 65.2 | 0.8 | 64.5 | 0.3 | 65.3 | 0.7 | 0.1 | 0.5 | 0.890 | 65.5 | 1.1 | 65.3 | 0.6 | 65.1 | 0.6 | −0.2 | 0.6 | 0.753 |
| Total cholesterol, mg/dL | 161.1 | 3.9 | 164.2 | 2.4 | 166.1 | 3.7 | 2.5 | 2.2 | 0.274 | 154.2 | 2.4 | 158.1 | 1.5 | 156.5 | 4.4 | 0.1 | 2.8 | 0.984 |
| Hip circumference, cm | 89.8 | 0.6 | 90.1 | 0.4 | 92.3 * | 0.7 | 1.3 | 0.4 | 0.007 | 90.2 | 0.8 | 91.7 | 0.5 | 93.8 * | 0.7 | 2.0 | 0.6 | 0.002 |
| Body fat, % | 26.1 | 0.5 | 26.7 | 0.3 | 28.5 * | 0.5 | 1.2 | 0.4 | 0.005 | 17.7 | 1.0 | 19.8 * | 0.5 | 20.8 * | 0.6 | 1.3 | 0.6 | 0.030 |
| Body adiposity index, % | 27.6 | 0.3 | 27.9 | 0.2 | 29.1 * | 0.3 | 0.8 | 0.2 | 0.001 | 24.9 | 0.4 | 26.2 * | 0.2 | 26.7 * | 0.3 | 0.8 | 0.3 | 0.005 |
| Body mass index, kg/m2 | 20.3 | 0.3 | 20.7 | 0.2 | 21.5 * | 0.3 | 0.6 | 0.2 | 0.007 | 21.0 | 0.4 | 22.0 * | 0.2 | 22.7 * | 0.3 | 0.8 | 0.3 | 0.009 |
| Factors | Girls | Boys | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Prevalence, % | 1–500 vs. NI | >500 vs. NI | Prevalence, % | 1–500 vs. NI | >500 vs. NI | |||||||||||
| NI | 1–500 | >500 | aOR | (95% CI) | aOR | (95% CI) | ptrend | NI | 1–500 | >500 | aOR | (95% CI) | aOR | (95% CI) | ptrend | |
| IDF criteria | ||||||||||||||||
| Large WC | 8.2 | 13.4 | 22.7 | 2.0 | (0.99–3.9) | 4.1 | (1.9–8.8) | <0.001 | 7.4 | 12.1 | 18.7 | 2.0 | (0.8–5.1) | 3.0 | (1.2–7.6) | 0.011 |
| Low HDL-C | 5.2 | 9.1 | 11.2 | 1.8 | (0.8–4.4) | 2.1 | (0.7–6.7) | 0.194 | 4.3 | 9.5 | 13.5 | 2.4 | (0.7–8.1) | 3.9 | (0.9–16.4) | 0.067 |
| Elevated TG | 2.3 | 4.0 | 4.6 | 1.9 | (0.8–4.4) | 2.1 | (0.7–6.8) | 0.197 | 3.9 | 5.5 | 7.1 | 1.3 | (0.5–3.7) | 1.7 | (0.6–5.1) | 0.289 |
| Increased FPG | 9.0 | 10.8 | 11.8 | 1.3 | (0.6–2.5) | 1.5 | (0.9–2.4) | 0.203 | 17.2 | 19.4 | 17.3 | 1.2 | (0.6–2.4) | 1.1 | (0.6–2.2) | 0.908 |
| High BP | 3.6 | 4.3 | 4.9 | 1.2 | (0.3–4.3) | 1.5 | (0.5–5.2) | 0.423 | 12.9 | 10.8 | 15.5 | 0.8 | (0.3–2.3) | 1.2 | (0.5–3.1) | 0.244 |
| Component (c) no. | ||||||||||||||||
| 1c | 21.8 | 29.6 | 27.7 | 23.2 | 26.6 | 27.8 | ||||||||||
| 2c | 3.3 | 4.3 | 10.6 | 10.4 | 9.1 | 13.1 | ||||||||||
| 3c | 0.0 | 1.1 | 2.1 | 0.6 | 2.2 | 5.5 | ||||||||||
| MetS (WC + ≥2c) | 0.0 | 1.1 | 2.1 | 3.8 2 | (0.6–∞) | 6.5 2 | (0.9–∞) | 0.049 2 | 0.6 | 3.5 | 5.4 | 6.9 | (0.7–63.2) | 10.3 | (1.2–90.2) | 0.007 |
| Cook criteria | ||||||||||||||||
| Large WC | 6.1 | 10.7 | 10.5 | 2.1 | (1.0–4.4) | 2.3 | (1.1–4.8) | 0.014 | 5.9 | 9.7 | 14.7 | 2.1 | (0.9–5.0) | 3.1 | (1.4–6.9) | 0.008 |
| Low HDL-C | 5.2 | 9.1 | 11.3 | 1.8 | (0.8–4.4) | 2.2 | (0.7–6.7) | 0.184 | 4.9 | 9.5 | 13.5 | 2.1 | (0.7–6.7) | 3.4 | (0.8–14.0) | 0.083 |
| Elevated TG | 9.2 | 12.9 | 15.0 | 1.6 | (0.9–2.9) | 1.9 | (0.96–3.7) | 0.065 | 9.7 | 16.3 | 18.9 | 1.9 | (0.9–4.0) | 2.3 | (1.1–5.0) | 0.045 |
| High FPG | 1.4 | 1.9 | 1.8 | 1.9 | (0.7–4.9) | 1.6 | (0.2–10.8) | 0.690 | 0.0 | 1.9 | 1.5 | 3.6 2 | (0.6–-∞) | 2.0 2 | (0.3–∞) | 1.000 2 |
| Raised BP | 12.5 | 16.2 | 23.0 | 1.3 | (0.8–2.1) | 2.1 | (1.3–3.7) | 0.015 | 18.0 | 17.3 | 22.0 | 0.9 | (0.4–1.9) | 1.2 | (0.6–2.6) | 0.266 |
| Component (c) no. | ||||||||||||||||
| 1c | 22.5 | 29.1 | 21.1 | 26.6 | 24.8 | 31.5 | ||||||||||
| 2c | 5.1 | 8.0 | 14.7 | 4.4 | 8.3 | 11.6 | ||||||||||
| 3c | 0.6 | 1.7 | 2.5 | 1.0 | 3.1 | 4.5 | ||||||||||
| MetS (≥3c) | 0.6 | 1.9 | 3.4 | 3.2 | (0.6–17.8) | 5.9 | (0.8–43.8) | 0.085 | 1.0 | 4.1 | 5.1 | 4.9 | (1.1–21.1) | 5.1 | (1.01–25.5) | 0.251 |
| Factors | Girls | Boys | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Prevalence, % | 1–500 vs. NI | >500 vs. NI | Prevalence, % | 1–500 vs. NI | >500 vs. NI | |||||||||||
| NI | 1–500 | >500 | aOR | (95% CI) | aOR | (95% CI) | ptrend | NI | 1–500 | >500 | aOR | (95% CI) | aOR | (95% CI) | ptrend | |
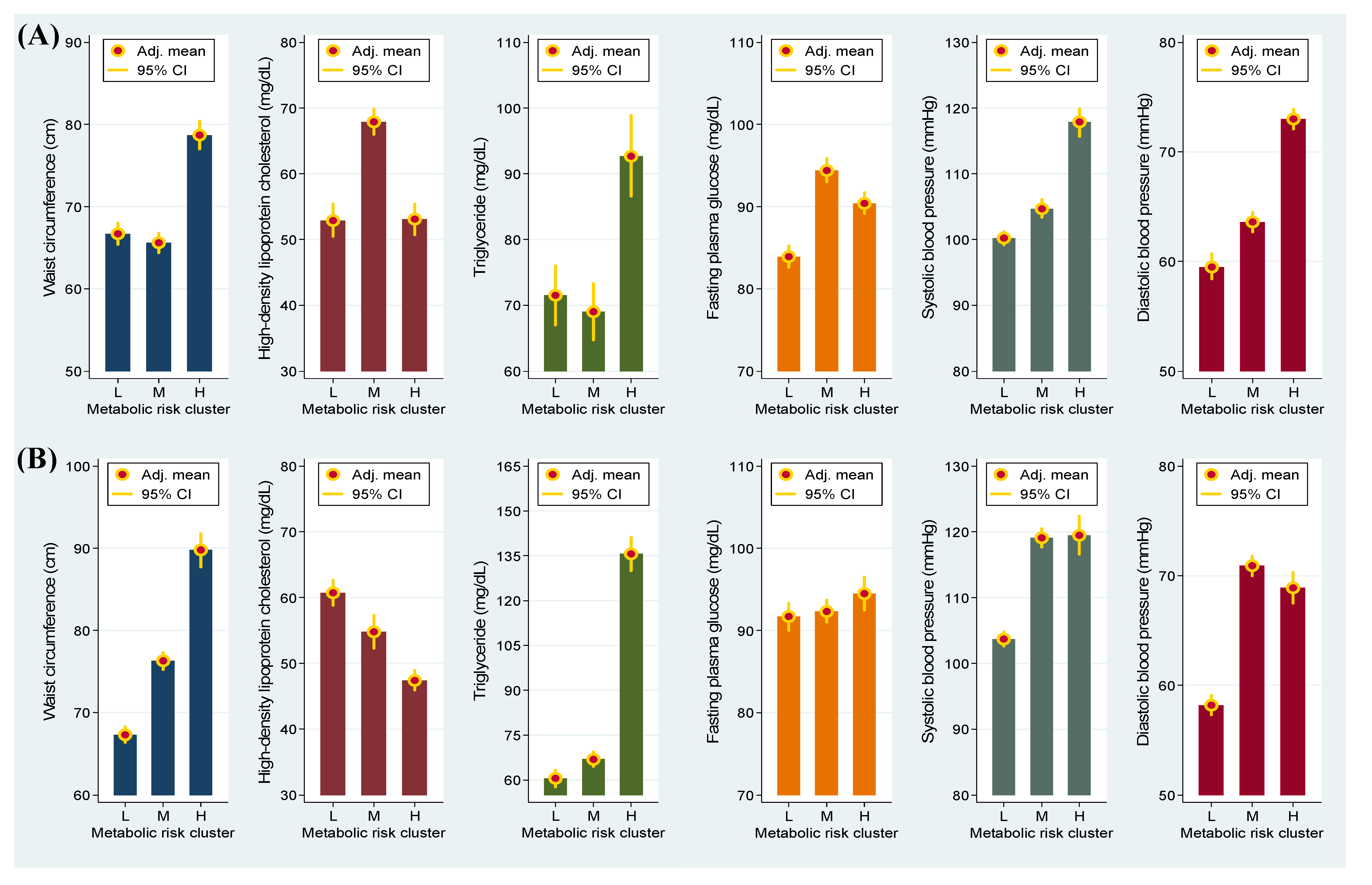
| Metabolic risk cluster 2 | ||||||||||||||||
| Low | 35.2 | 34.7 | 33.5 | 1.0 | 1.0 | 42.8 | 43.6 | 37.1 | 1.0 | 1.0 | ||||||
| Median | 42.0 | 38.5 | 34.5 | 1.2 | (0.8–1.8) | 1.2 | (0.7–2.2) | 0.433 | 47.4 | 36.6 | 40.9 | 0.8 | (0.5–1.3) | 1.0 | (0.6–1.6) | 0.530 |
| High | 22.8 | 26.9 | 32.1 | 1.4 | (0.9–2.3) | 1.9 | (1.1–3.1) | 0.020 | 9.8 | 19.8 | 22.1 | 2.2 | (1.0–4.8) | 2.7 | (1.3–5.7) | 0.038 |

4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Abbreviations
| aOR | adjusted odds ratio |
| BAI | body adiposity index |
| BMI | body mass index |
| CI | confidence interval |
| DBP | diastolic blood pressure |
| FPG | fasting plasma glucose |
| HC | hip circumference |
| HDL-C | high-density lipoprotein cholesterol |
| IDF | International Diabetes Federation |
| LDL-C | low-density lipoprotein cholesterol |
| MET | metabolic equivalent task |
| MetS | metabolic syndrome |
| SSB | sugar-sweetened beverage |
| SBP | systolic blood pressure |
| TG | triglycerides |
| WC | waist circumference |
Conflicts of interest
References
- Bao, W.; Srinivasan, S.R.; Valdez, R.; Greenlund, K.J.; Wattigney, W.A.; Berenson, G.S. Longitudinal changes in cardiovascular risk from childhood to young adulthood in offspring of parents with coronary artery disease: The Bogalusa Heart Study. JAMA 1997, 278, 1749–1754. [Google Scholar] [CrossRef]
- Lin, W.T.; Huang, H.L.; Huang, M.C.; Chan, T.F.; Ciou, S.Y.; Lee, C.Y.; Chiu, Y.W.; Duh, T.H.; Lin, P.L.; Wang, T.N.; et al. Effects on uric acid, body mass index and blood pressure in adolescents of consuming beverages sweetened with high-fructose corn syrup. Int. J. Obes. 2013, 37, 532–539. [Google Scholar] [CrossRef]
- Ambrosini, G.L.; Oddy, W.H.; Huang, R.C.; Mori, T.A.; Beilin, L.J.; Jebb, S.A. Prospective associations between sugar-sweetened beverage intakes and cardiometabolic risk factors in adolescents. Am. J. Clin. Nutr. 2013, 98, 327–334. [Google Scholar] [CrossRef]
- Alberti, K.G.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.C.; James, W.P.; Loria, C.M.; Smith, S.C., Jr. Harmonizing the metabolic syndrome: A joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [CrossRef]
- Isomaa, B.; Almgren, P.; Tuomi, T.; Forsen, B.; Lahti, K.; Nissen, M.; Taskinen, M.R.; Groop, L. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care 2001, 24, 683–689. [Google Scholar] [CrossRef]
- Stern, M.P.; Williams, K.; Gonzalez-Villalpando, C.; Hunt, K.J.; Haffner, S.M. Does the metabolic syndrome improve identification of individuals at risk of type 2 diabetes and/or cardiovascular disease? Diabetes Care 2004, 27, 2676–2681. [Google Scholar]
- Zimmet, P.; Alberti, K.G.; Kaufman, F.; Tajima, N.; Silink, M.; Arslanian, S.; Wong, G.; Bennett, P.; Shaw, J.; Caprio, S. The metabolic syndrome in children and adolescents—An IDF consensus report. Pediatr. Diabetes 2007, 8, 299–306. [Google Scholar] [CrossRef]
- Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z. The metabolic syndrome. Lancet 2005, 365, 1415–1428. [Google Scholar] [CrossRef]
- Goodman, E.; Daniels, S.R.; Morrison, J.A.; Huang, B.; Dolan, L.M. Contrasting prevalence of and demographic disparities in the World Health Organization and National Cholesterol Education Program Adult Treatment Panel III definitions of metabolic syndrome among adolescents. J. Pediatr. 2004, 145, 445–451. [Google Scholar] [CrossRef]
- Johnson, W.D.; Kroon, J.J.; Greenway, F.L.; Bouchard, C.; Ryan, D.; Katzmarzyk, P.T. Prevalence of risk factors for metabolic syndrome in adolescents: National Health and Nutrition Examination Survey (NHANES), 2001–2006. Arch. Pediatr. Adolesc. Med. 2009, 163, 371–377. [Google Scholar] [CrossRef]
- Morrison, J.A.; Friedman, L.A.; Gray-McGuire, C. Metabolic syndrome in childhood predicts adult cardiovascular disease 25 years later: The Princeton Lipid Research Clinics Follow-up Study. Pediatrics 2007, 120, 340–345. [Google Scholar] [CrossRef]
- Morrison, J.A.; Friedman, L.A.; Wang, P.; Glueck, C.J. Metabolic syndrome in childhood predicts adult metabolic syndrome and type 2 diabetes mellitus 25 to 30 years later. J. Pediatr. 2008, 152, 201–206. [Google Scholar] [CrossRef]
- Reedy, J.; Krebs-Smith, S.M. Dietary sources of energy, solid fats, and added sugars among children and adolescents in the United State. J. Am. Diet. Assoc. 2010, 110, 1477–1484. [Google Scholar] [CrossRef]
- Popkin, B.M.; Armstrong, L.E.; Bray, G.M.; Caballero, B.; Frei, B.; Willett, W.C. A new proposed guidance system for beverage consumption in the United States. Am. J. Clin. Nutr. 2006, 83, 529–542. [Google Scholar]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Despres, J.P.; Hu, F.B. Sugar-sweetened beverages, obesity, type 2 diabetes mellitus, and cardiovascular disease risk. Circulation 2010, 121, 1356–1364. [Google Scholar] [CrossRef]
- Malik, V.S.; Pan, A.; Willett, W.C.; Hu, F.B. Sugar-sweetened beverages and weight gain in children and adults: A systematic review and meta-analysis. Am. J. Clin. Nutr. 2013, 98, 1084–1102. [Google Scholar] [CrossRef]
- Richelsen, B. Sugar-sweetened beverages and cardio-metabolic disease risks. Curr. Opin. Clin. Nutr. Metab. Care 2013, 16, 478–484. [Google Scholar] [CrossRef]
- Cassady, B.A.; Considine, R.V.; Mattes, R.D. Beverage consumption, appetite, and energy intake: What did you expect? Am. J. Clin. Nutr. 2012, 95, 587–593. [Google Scholar] [CrossRef]
- Pan, A.; Hu, F.B. Effects of carbohydrates on satiety: Differences between liquid and solid food. Curr. Opin. Clin. Nutr. Metab. Care 2011, 14, 385–390. [Google Scholar] [CrossRef]
- Woodward-Lopez, G.; Kao, J.; Ritchie, L. To what extent have sweetened beverages contributed to the obesity epidemic? Public Health Nutr. 2011, 14, 499–509. [Google Scholar] [CrossRef]
- Chu, N.F. Prevalence of obesity in Taiwan. Obes. Rev. 2005, 6, 271–274. [Google Scholar] [CrossRef]
- Taiwanese Food and Nutrients Databank. Available online: https://consumer.fda.gov.tw/ FoodAnalysis/ingredients.htm (accessed on 10 October 2012).
- Bergman, R.N.; Stefanovski, D.; Buchanan, T.A.; Sumner, A.E.; Reynolds, J.C.; Sebring, N.G.; Xiang, A.H.; Watanabe, R.M. A better index of body adiposity. Obesity 2011, 19, 1083–1089. [Google Scholar] [CrossRef]
- Cole, T.J.; Bellizzi, M.C.; Flegal, K.M.; Dietz, W.H. Establishing a standard definition for child overweight and obesity worldwide: International survey. BMJ 2000, 320, 1240–1243. [Google Scholar] [CrossRef]
- Allain, C.C.; Poon, L.S.; Chan, C.S.; Richmond, W.; Fu, P.C. Enzymatic determination of total serum cholesterol. Clin. Chem. 1974, 20, 470–475. [Google Scholar]
- Cook, S.; Auinger, P.; Li, C.; Ford, E.S. Metabolic syndrome rates in United States adolescents, from the National Health and Nutrition Examination Survey, 1999–2002. J. Pediatr. 2008, 152, 165–170. [Google Scholar] [CrossRef]
- Mickey, R.M.; Greenland, S. The impact of confounder selection criteria on effect estimation. Am. J. Epidemiol. 1989, 129, 125–137. [Google Scholar]
- Lee, C.H.; Yang, S.F.; Peng, C.Y.; Li, R.N.; Chen, Y.C.; Chan, T.F.; Tsai, E.M.; Kuo, F.C.; Huang, J.J.; Tsai, H.T.; et al. The precancerous effect of emitted cooking oil fumes on precursor lesions of cervical cancer. Int. J. Cancer 2010, 127, 932–941. [Google Scholar]
- Huang, R.C.; Mori, T.A.; Burke, V.; Newnham, J.; Stanley, F.J.; Landau, L.I.; Kendall, G.E.; Oddy, W.H.; Beilin, L.J. Synergy between adiposity, insulin resistance, metabolic risk factors, and inflammation in adolescents. Diabetes Care 2009, 32, 695–701. [Google Scholar] [CrossRef]
- Lee, C.H.; Wu, D.C.; Lee, J.M.; Wu, I.C.; Goan, Y.G.; Kao, E.L.; Huang, H.L.; Chan, T.F.; Chou, S.H.; Chou, Y.P.; et al. Anatomical subsite discrepancy in relation to the impact of the consumption of alcohol, tobacco and betel quid on esophageal cancer. Int. J. Cancer 2007, 120, 1755–1762. [Google Scholar] [CrossRef]
- Vartanian, L.R.; Schwartz, M.B.; Brownell, K.D. Effects of soft drink consumption on nutrition and health: A systematic review and meta-analysis. Am. J. Public Health 2007, 97, 667–675. [Google Scholar] [CrossRef]
- Malik, V.S.; Schulze, M.B.; Hu, F.B. Intake of sugar-sweetened beverages and weight gain: A systematic review. Am. J. Clin. Nutr. 2006, 84, 274–288. [Google Scholar]
- Gibson, S. Sugar-sweetened soft drinks and obesity: A systematic review of the evidence from observational studies and interventions. Nutr. Res. Rev. 2008, 21, 134–147. [Google Scholar] [CrossRef]
- Kosova, E.C.; Auinger, P.; Bremer, A.A. The relationships between sugar-sweetened beverage intake and cardiometabolic markers in young children. J. Acad. Nutr. Diet. 2013, 113, 219–227. [Google Scholar] [CrossRef]
- Bremer, A.A.; Auinger, P.; Byrd, R.S. Relationship between insulin resistance-associated metabolic parameters and anthropometric measurements with sugar-sweetened beverage intake and physical activity levels in US adolescents: Findings from the 1999–2004 National Health and Nutrition Examination Survey. Arch. Pediatr. Adolesc. Med. 2009, 163, 328–335. [Google Scholar] [CrossRef]
- Chan, T.F.; Lin, W.T.; Chen, Y.L.; Huang, H.L.; Yang, W.Z.; Lee, C.Y.; Chen, M.H.; Wang, T.N.; Huang, M.C.; Chiu, Y.W.; et al. Elevated serum triglyceride and retinol-binding protein 4 levels associated with fructose-sweetened beverages in adolescents. PLoS One 2014, 9, e82004. [Google Scholar]
- Nguyen, S.; Choi, H.K.; Lustig, R.H.; Hsu, C.Y. Sugar-sweetened beverages, serum uric acid, and blood pressure in adolescents. J. Pediatr. 2009, 154, 807–813. [Google Scholar] [CrossRef]
- Malik, A.H.; Akram, Y.; Shetty, S.; Malik, S.S.; Njike, V. Impact of sugar-sweetened beverages on blood pressure. Am. J. Cardiol. 2014, 113, 1574–1580. [Google Scholar] [CrossRef]
© 2014 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/3.0/).
Share and Cite
Chan, T.-F.; Lin, W.-T.; Huang, H.-L.; Lee, C.-Y.; Wu, P.-W.; Chiu, Y.-W.; Huang, C.-C.; Tsai, S.; Lin, C.-L.; Lee, C.-H. Consumption of Sugar-Sweetened Beverages Is Associated with Components of the Metabolic Syndrome in Adolescents. Nutrients 2014, 6, 2088-2103. https://doi.org/10.3390/nu6052088
Chan T-F, Lin W-T, Huang H-L, Lee C-Y, Wu P-W, Chiu Y-W, Huang C-C, Tsai S, Lin C-L, Lee C-H. Consumption of Sugar-Sweetened Beverages Is Associated with Components of the Metabolic Syndrome in Adolescents. Nutrients. 2014; 6(5):2088-2103. https://doi.org/10.3390/nu6052088
Chicago/Turabian StyleChan, Te-Fu, Wei-Ting Lin, Hsiao-Ling Huang, Chun-Ying Lee, Pei-Wen Wu, Yu-Wen Chiu, Chun-Chi Huang, Sharon Tsai, Chih-Lung Lin, and Chien-Hung Lee. 2014. "Consumption of Sugar-Sweetened Beverages Is Associated with Components of the Metabolic Syndrome in Adolescents" Nutrients 6, no. 5: 2088-2103. https://doi.org/10.3390/nu6052088