Glycemic Responses, Appetite Ratings and Gastrointestinal Hormone Responses of Most Common Breads Consumed in Spain. A Randomized Control Trial in Healthy Humans


 , and
, and 
Abstract
:1. Introduction
2. Participants and Methods
2.1. Study Design

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Energy (kcal/100 g) | Protein (%) | Fat (%) | CHO (%) | Fibre (%) | Ash (%) | Moisture (%) | AV-CHO (g) | AV-CHO per Serving (40 g) γ | Bread Provided (g (kcal)) * | |
|---|---|---|---|---|---|---|---|---|---|---|
| Ordinary | 283 | 9.3 | 1.3 | 56.5 | 4.1 | 2.3 | 30 | 52.4 | 21.0 | 95 (270) |
| Precooked-Frozen | 271 | 8.8 | 1.2 | 54.2 | 4.3 | 2 | 33.7 | 49.9 | 20.0 | 100 (270) |
| Candeal-flour | 275 | 7.6 | 1.3 | 56.6 | 3.3 | 2.2 | 32.2 | 53.3 | 21.3 | 94 (258) |
| Alfacar | 282 | 9.3 | 1.3 | 56.6 | 3.5 | 2 | 30.5 | 53.1 | 21.2 | 94 (266) |
| Wholemeal | 243 | 8.8 | 1.2 | 45.3 | 7.9 | 1.8 | 41.6 | 37.4 | 15.0 | 134 (325) |
2.2. Subject Selection
2.3. Assessed Breads
2.4. Study Performance
3. Methodology
3.1. Analytical Methods
3.2. GI, GL and InI Calculations
3.3. Appetite Profile Determination
3.4. Statistical Analysis
4. Results
4.1. Baseline Subject Characteristics
| Mean ± SEM | |
|---|---|
| Gender (Male/Female) | (12/10) |
| Age (years) | 26 ± 1 |
| BMI (kg/m2) | 23.8 ± 0.5 |
| Waist circumference (cm) | 76 ± 2 |
| Body fat (kg) | 15.2 ± 1.2 |
| Lean body mass (kg) | 53.1 ± 2.2 |
| Fat free body mass (kg) | 50.4 ± 2.1 |
| Total water (kg) | 37.2 ± 1.5 |
| Bone mass (kg) | 2.7 ± 0.1 |
| Basal metabolic rate (kcal) | 1594 ± 59 |
| Values are expressed as the mean ± SEM (n = 22). | |
4.2. GI, GL and InI
| Ordinary | Precooked-Frozen | Candeal-Flour | Alfacar | Wholemeal | |
|---|---|---|---|---|---|
| Mean (CI 95%) | Mean (CI 95%) | Mean (CI 95%) | Mean (CI 95%) | Mean (CI 95%) | |
| GI | 76 (59/92) | 78(54/89) | 86 (70/103) | 68 * (51/83) | 61 * (44/76) |
| GL | 16 b* (12/18) | 16 b* (11/18) | 18 b* (15/22) | 14 ab* (11/18) | 9 a* (6/12) |
| InI | 68 * (59–81) | 68 * (57/78) | 69 * (59/80) | 70 * (60/81) | 73 * (63/84) |
| Mean ± SEM | Mean ± SEM | Mean ± SEM | Mean ± SEM | Mean ± SEM | |
| Glucose AUC (mg/dL·min) | 910 ± 125 | 854 ± 135 | 1133 ± 127 | 886 ± 125 | 828 ± 125 |
| Insulin AUC (mU/mL·min) | 2020 ± 247 | 1810 ± 254 | 1955 ± 248 | 1939 ± 248 | 2190 ± 248 |
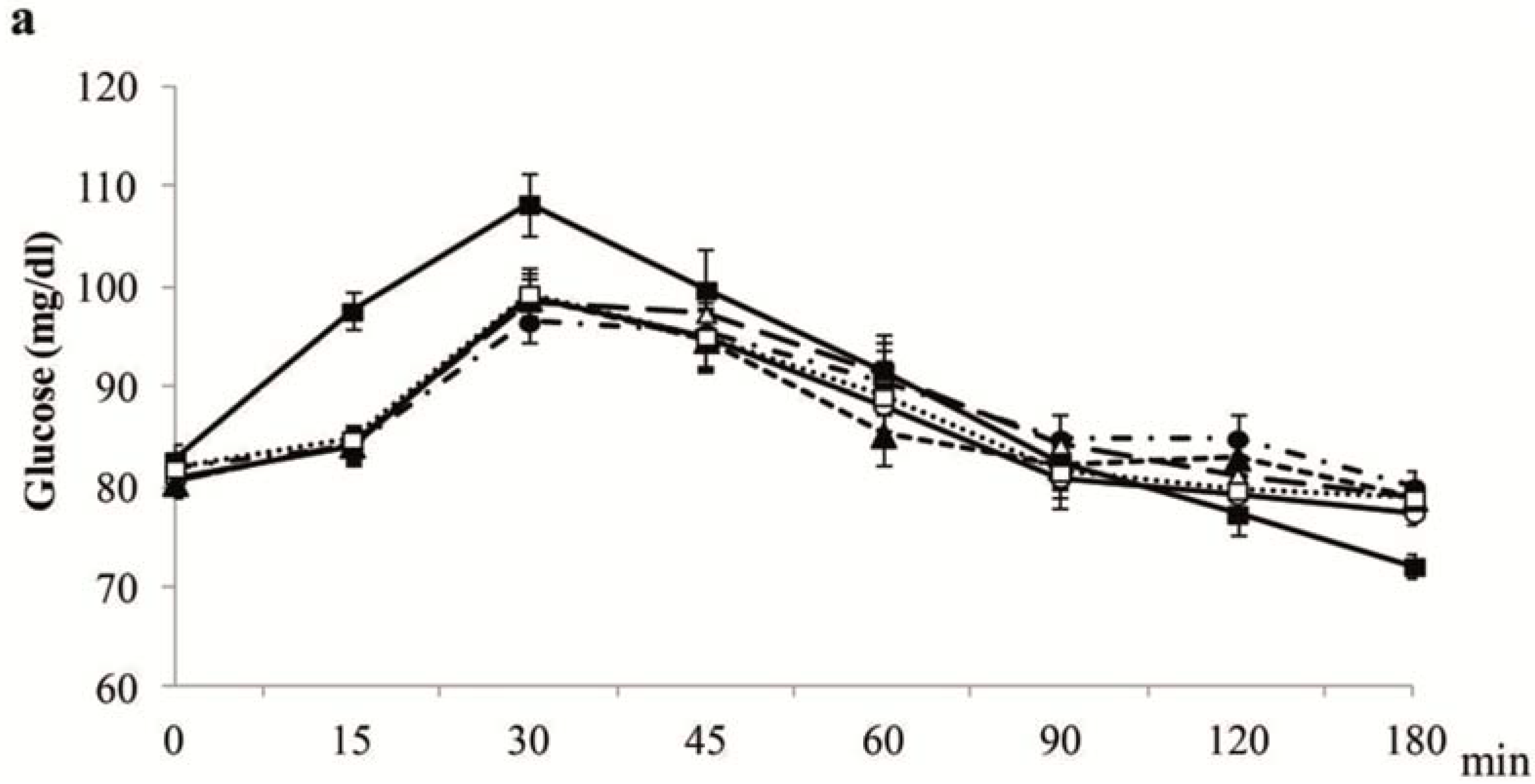
4.3. Plasma Glucose and Insulin Postprandial Concentrations


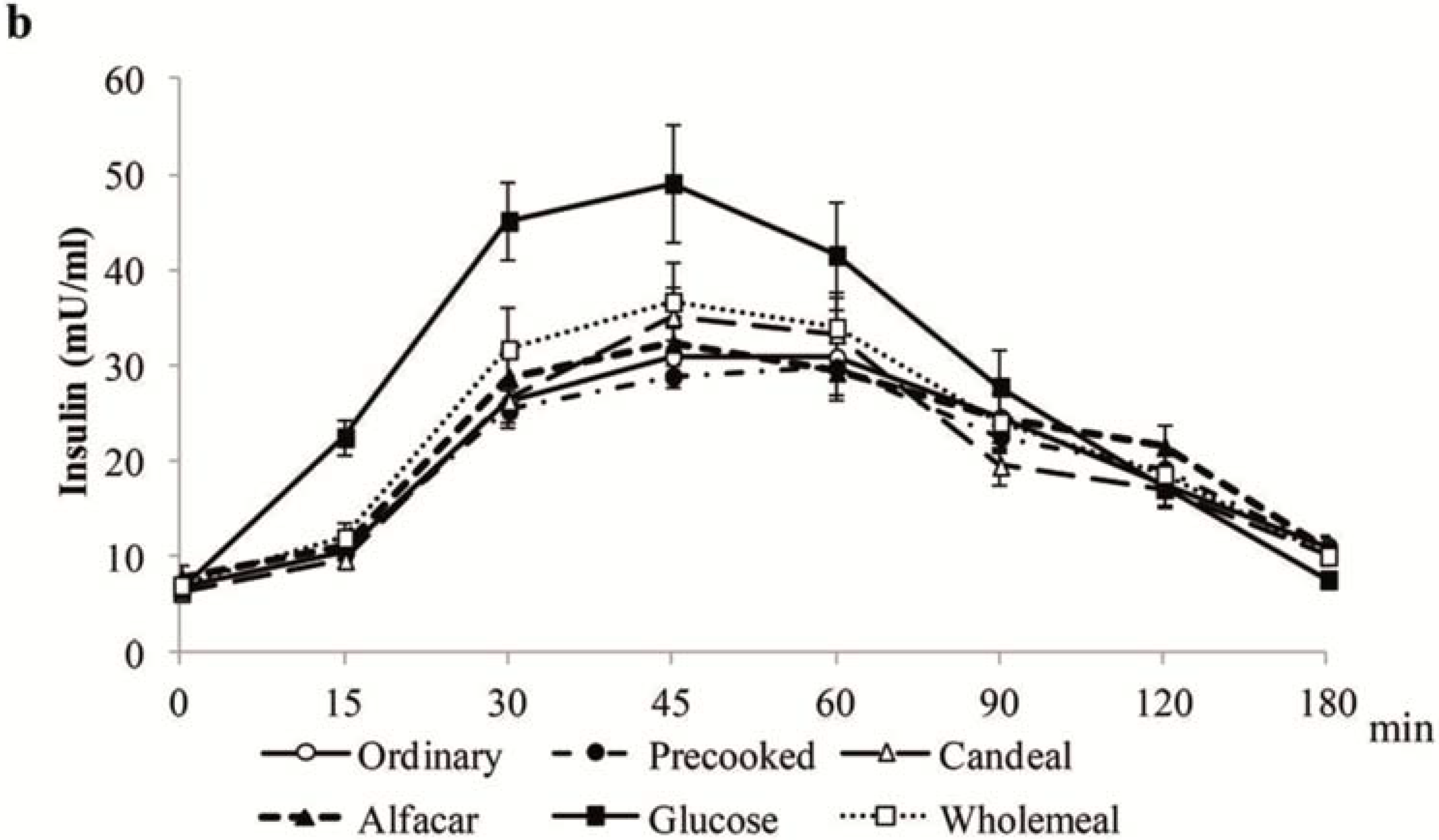
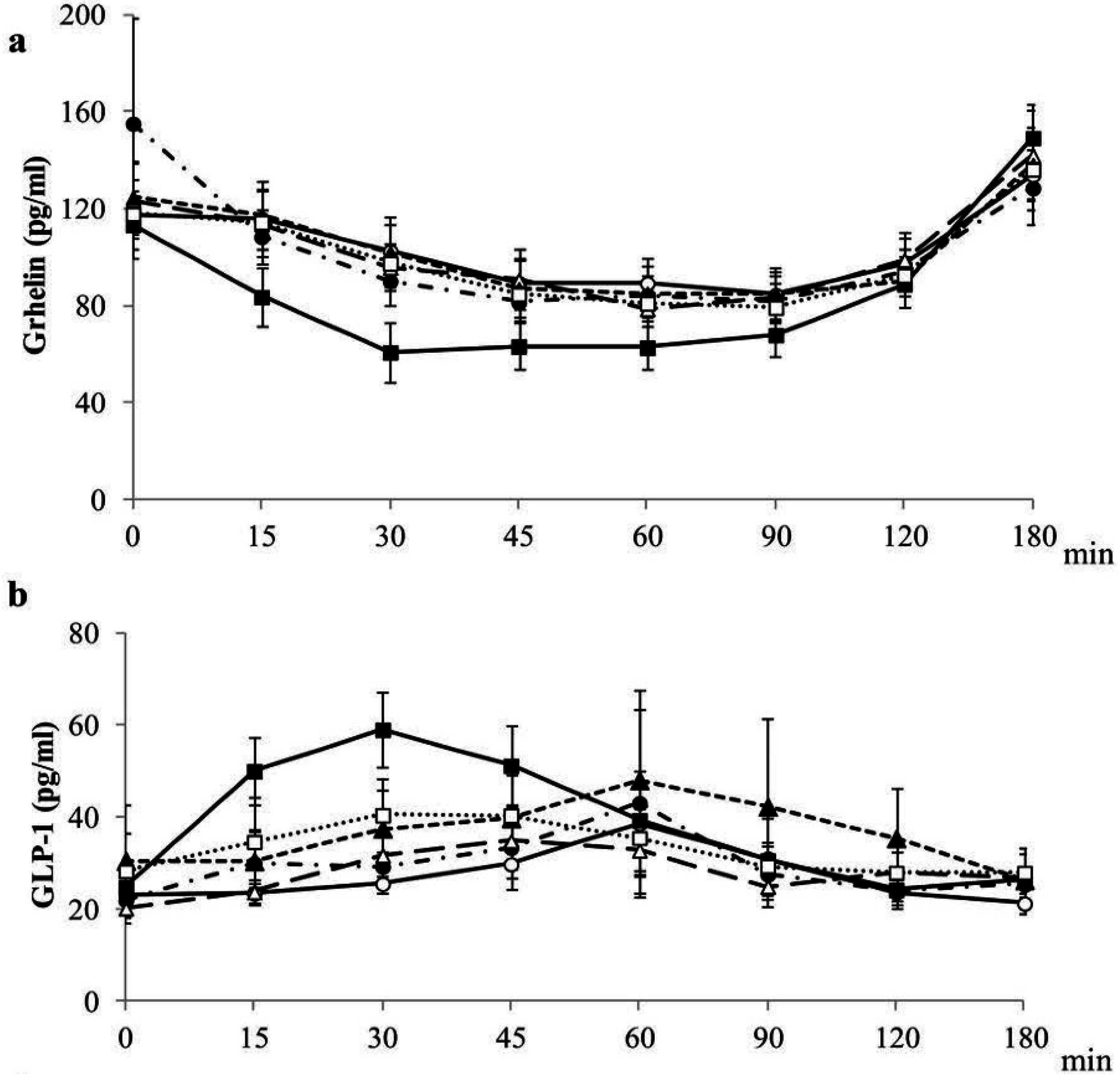
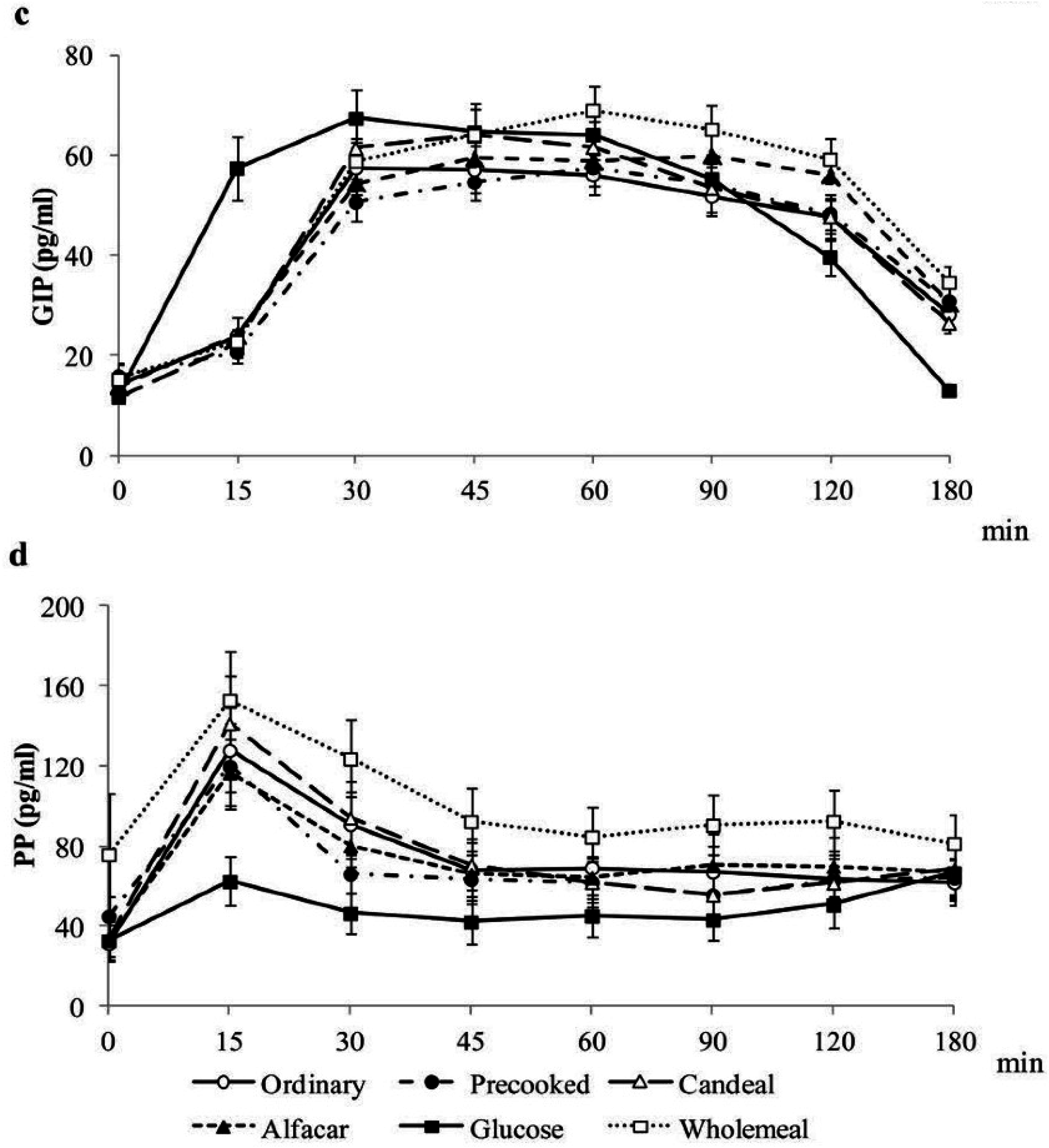
4.4. Postprandial Gastrointestinal Hormones Plasma Concentrations


| GI | GL | InI | |
|---|---|---|---|
| EI | 0.013 | 0.116 ** | 0.127 * |
| Hunger neg | 0.025 | 0.038 | −0.034 |
| Satiety | 0.162 * | 0.248 | 0.026 |
| Fullness | 0.183 * | 0.297 * | 0.069 |
| Prospective consumption neg | 0.066 | 0.086 | 0.039 |
| CAS | 0.118 | 0.18 | 0.017 |
| Ghrelin neg | −0.069 | 0.059 | −0.023 |
| GLP-1 | 0.221 ** | 0.182 ** | 0.489 *** |
| GIP | −0.07 | −0.029 | 0.151 * |
| PP | −0.111 | −0.245 *** | −0.043 |
| PYY | 0.14 | −0.017 | 0.347 *** |
4.5. Appetite Ratings and Sensory Acceptance
4.6. Correlations between GI, GL, InI, Gastrointestinal Hormones Postprandial Concentrations, ad libitum Energy Intake and Appetite Scores
5. Discussion
6. Conclusions
Supplementary Files
Supplementary File 1Acknowledgments
Author Contributions
Conflicts of Interest
References
- Castro-Quezada, I.; Román-Viñas, B.; Serra-Majem, L. The Mediterranean diet and nutritional adequacy: A review. Nutrients 2014, 6, 231–248. [Google Scholar] [CrossRef] [PubMed]
- Kantor, L.S.; Variyam, J.N.; Allshouse, J.E. Choose a variety of grains daily, especially whole grains: A challenge for consumers. J. Nutr. 2001, 131, 473S–486S. [Google Scholar] [PubMed]
- Serra-Majem, L.; Raido Quintana, B. Consumo de pan en el mundo y en España (Bread consumption in the world and in Spain). In Libro Blanco del Pan (Bread’s White Book); Gil, A., Serra-Majem, L., Eds.; Ed. Med. Panamericana: Madrid, Spain, 2010; pp. 63–77. [Google Scholar]
- Varela-Moreiras, G.; Ruiz, E.; Valero, T.; Avila, J.M.; del Pozo, S. The Spanish diet: An update. Nutr. Hosp. 2013, 28, 13–20. [Google Scholar] [PubMed]
- Gallus, S.; Lugo, A.; Murisic, B.; Bosetti, C.; Boffetta, P.; la Vecchia, C. Overweight and obesity in 16 European countries. Eur. J. Nutr. 2014, 5. [Google Scholar] [CrossRef]
- Greenwood, D.C.; Threapleton, D.E.; Evans, C.E.; Cleghorn, C.L.; Nykjaer, C.; Woodhead, C.; Burley, V.J. Glycemic index, glycemic load, carbohydrates, and type 2 diabetes. Systematic review and dose-response meta-analysis of prospective studies. Diabetes Care 2013, 36, 4166–4171. [Google Scholar] [CrossRef] [PubMed]
- Barclay, A.W.; Petocz, P.; McMillan-Price, J.; Flood, V.M.; Prvan, T.; Mitchell, P.; Brand-Miller, J.C. Glycemic index, glycemic load, and chronic disease risk—A meta analysis of observational studies. Am. J. Clin. Nutr. 2008, 87, 627–637. [Google Scholar] [PubMed]
- Sacks, F.M.; Carey, V.J.; Anderson, C.A.; Miller, E.R.; Copeland, T.; Charleston, J.; Harshfield, B.J.; Laranjo, N.; McCarron, P.; Swain, J.; et al. Effects of high vs. low glycemic index of dietary carbohydrate on cardiovascular disease risk factors and insulin sensitivity: The OmniCarb randomized clinical trial. JAMA 2014, 312, 2531–2541. [Google Scholar] [CrossRef] [PubMed]
- Mendez, M.A.; Covas, M.I.; Marrugat, J.; Vila, J.; Schröder, H. Glycemic load, glycemic index, and body mass index in Spanish adults. Am. J. Clin. Nutr. 2009, 89, 316–322. [Google Scholar] [CrossRef] [PubMed]
- Aziz, A. The glycemic index: Methodological aspects related to the interpretation of health effects and to regulatory labeling. J. AOAC Int. 2009, 92, 879–887. [Google Scholar] [PubMed]
- DeVries, J.W. Glycemic index: The analytical perspective. Cereal Foods World 2007, 52, 45–49. [Google Scholar]
- Wolever, T.M. Is glycaemic index (GI) a valid measure of carbohydrate quality? Eur. J. Clin. Nutr. 2013, 67, 522–531. [Google Scholar] [CrossRef] [PubMed]
- Bao, J.; Atkinson, F.; Petocz, P.; Willett, W.C.; Brand-Miller, J.C. Prediction of postprandial glycemia and insulinemia in lean, young, healthy adults: Glycemic load compared with carbohydrate content alone. Am. J. Clin. Nutr. 2011, 93, 984–996. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.S.; Singhania, P.R. Glycemic and insulinemic responses to carbohydrate rich whole foods. J. Food. Sci. Technol. 2014, 51, 347–352. [Google Scholar]
- Jenkins, D.J.; Wesson, V.; Wolever, T.M.; Jenkins, A.L.; Kalmusky, J.; Guidici, S.; Csima, A.; Josse, R.G.; Wong, G.S. Wholemeal versus wholegrain breads: Proportion of whole or cracked grain and the glycaemic response. BMJ 1988, 297, 958–960. [Google Scholar] [CrossRef] [PubMed]
- Fardet, A.; Leenhardt, F.; Lioger, D.; Scalbert, A.; Rémésy, C. Parameters controlling the glycemic response to breads. Nutr. Res. Rev. 2006, 19, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Rizkalla, S.W.; Laromiguiere, M.; Champ, M.; Bruzzo, F.; Boillot, J.; Slama, G. Effect of baking process on postprandial metabolic consequences: Randomized trials in normal and type 2 diabetic subjects. Eur. J. Clin. Nutr. 2007, 61, 75–183. [Google Scholar] [CrossRef]
- De Angelis, M.; Rizzello, C.G.; Alfonsi, G.; Arnault, P.; Cappelle, S.; Di Cagno, R.; Gobbetti, M. Use of sourdough lactobacilli and oat fibre to decrease the glycaemic index of white wheat bread. Br. J. Nutr. 2007, 98, 1196–1205. [Google Scholar] [CrossRef] [PubMed]
- Lau, E.; Soong, Y.Y.; Zhou, W.; Henry, J. Can bread processing conditions alter glycaemic response? Food. Chem. 2015, 173, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Cappelleri, J.C.; Bushmakin, A.G.; Gerber, R.A.; Leidy, N.K.; Sexton, C.C.; Lowe, M.R.; Karlsson, J. Psychometric analysis of the Three-Factor Eating Questionnaire-R21: Results from a large diverse sample of obese and non-obese participants. Int. J. Obes. 2009, 33, 611–620. [Google Scholar] [CrossRef]
- Brouns, F.; Bjorck, I.; Frayn, K.N.; Gibbs, A.L.; Lang, V.; Slama, G.; Wolever, T.M. Glycaemic index methodology. Nutr. Res. Rev. 2005, 18, 145–171. [Google Scholar] [CrossRef] [PubMed]
- Blundell, J.; de Graaf, C.; Hulshof, T.; Jebb, S.; Livingstone, B.; Lluch, A.; Mela, D.; Salah, S.; Schuring, E.; van der Knaap, H.; et al. Appetite control: Methodological aspects of the evaluation of foods. Obes. Rev. 2010, 11, 251–270. [Google Scholar] [CrossRef] [PubMed]
- Gonzalez-Anton, C.; Lopez-Millan, B.; Rico, M.C.; Sanchez-Rodriguez, E.; Ruiz-Lopez, M.D.; Gil, A.; Mesa, M.D. An enriched, cereal-based bread affects appetite ratings and glycemic, insulinemic, and gastrointestinal hormone responses in healthy adults in a randomized controlled trial. J. Nutr. 2015, 145, 231–238. [Google Scholar] [CrossRef] [PubMed]
- The R Project for Statistical Computing. Available online: http://www.r-project.org/ (accessed on 21 January 2015).
- Gil, A.; Ruiz-Lopez, M.D.; Fernandez-Gonzalez, M.; Martinez de Victoria, E. The FINUT healthy lifestyles guide: Beyond the food pyramid. Adv. Nutr. 2014, 14, 358S–367S. [Google Scholar] [CrossRef]
- Joint FAO/WHO Expert Consultation. Carbohydrates in Human Nutrition: A Summary of the Joint FAO/WHO Expert Consultation; Food and Agriculture Organization (United Nations): Rome, Italy, 1997. [Google Scholar]
- Barclay, A.W.; Brand-Miller, J.C.; Wolever, T.M. Glycemic index, glycemic load, and glycemic response are not the same. Diabetes Care 2005, 28, 1839–1840. [Google Scholar] [CrossRef] [PubMed]
- Flint, A.; Raben, A.; Blundell, J.E.; Astrup, A. Reproducibility, power and validity of visual analogue scales in assessment of appetite sensations in single test meal studies. Int. J. Obes. 2000, 24, 38–48. [Google Scholar] [CrossRef]
- Burton, P.M.; Monro, J.A.; Alvarez, L.; Gallagher, E. Glycemic Impact and Health: New Horizons in White Bread Formulations. Crit. Rev. Food. Sci. 2011, 51, 965–982. [Google Scholar] [CrossRef]
- Yusof, B.N.; Abd Talib, R.; Karim, N.A.; Kamarudin, N.A.; Arshad, F. Glycaemic index of four commercially available breads in Malaysia. Int. J. Food. Sci. Nutr. 2009, 60, 487–496. [Google Scholar] [CrossRef] [PubMed]
- Scazzina, F.; Siebenhandl-Ehn, S.; Pellegrini, N. The effect of dietary fibre on reducing the glycaemic index of bread. Br. J. Nutr. 2013, 109, 1163–1174. [Google Scholar] [CrossRef] [PubMed]
- Burton, P.; Lightowler, H.J. Influence of bread volume on glycaemic response and satiety. Br. J. Nutr. 2006, 96, 877–882. [Google Scholar] [CrossRef] [PubMed]
- Ronda, F.; Gomez, M.; Quilez, J. Prolonged frozen storage of partially-baked wheat bread increases in vitro slowly digestible starch after final bake. Int. J. Food. Sci. Nutr. 2010, 61, 624–629. [Google Scholar] [CrossRef] [PubMed]
- Novotni, D.; Curić, D.; Bituh, M.; Colić Barić, I.; Skevin, D.; Cukelj, N. Glycemic index and phenolics of partially-baked frozen bread with sourdough. Int. J. Food. Sci. Nutr. 2011, 62, 26–33. [Google Scholar] [CrossRef] [PubMed]
- Najjar, A.M.; Parsons, P.M.; Duncan, A.M.; Robinson, L.E.; Yada, R.Y.; Graham, T.E. The acute impact of ingestion of breads of varying composition on blood glucose, insulin and incretins following first and second meals. Br. J. Nutr. 2009, 101, 391–398. [Google Scholar] [CrossRef] [PubMed]
- Mofidi, A.; Ferraro, Z.M.; Stewart, K.A.; Tulk, H.M.; Robinson, L.E.; Duncan, A.M.; Graham, T.E. The acute impact of ingestion of sourdough and whole-grain breads on blood glucose, insulin, and incretins in overweight and obese men. J. Nutr. Metable 2012, 2012, 184710. [Google Scholar]
- Juntunen, K.S.; Laaksonen, D.E.; Poutanen, K.S.; Niskanen, L.K.; Mykkänen, H.M. High-fiber rye bread and insulin secretion and sensitivity in healthy postmenopausal women. Am. J. Clin. Nutr. 2003, 77, 385–391. [Google Scholar] [PubMed]
- Keogh, J.; Atkinson, F.; Eisenhauer, B.; Inamdar, A.; Brand-Miller, J. Food intake, postprandial glucose, insulin and subjective satiety responses to three different bread-based test meals. Appetite 2011, 57, 707–710. [Google Scholar] [CrossRef] [PubMed]
- Hartvigsen, M.L.; Gregersen, S.; Lærke, H.N.; Holst, J.J.; Bach Knudsen, K.E.; Hermansen, K. Effects of concentrated arabinoxylan and β-glucan compared with refined wheat and whole grain rye on glucose and appetite in subjects with the metabolic syndrome: A randomized study. Eur. J. Clin. Nutr. 2014, 68, 84–90. [Google Scholar] [CrossRef] [PubMed]
- Mursu, J.; Virtanen, J.K.; Rissanen, T.H.; Tuomainen, T.P.; Nykänen, I.; Laukkanen, J.A.; Kortelainen, R.; Voutilainen, S. Glycemic index, glycemic load, and the risk of acute myocardial infarction in Finnish men: The Kuopio Ishcaemic Heart Disease Risk Factor Study. Nutr. Metab. Cardiovasc. Dis. 2011, 21, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Oh, K.; Hu, F.B.; Cho, E.; Rexrode, K.M.; Stampfer, M.J.; Manson, J.E.; Liu, S.; Willett, W.C. Carbohydrate intake, glycemic index, glycemic load, and dietary fiber in relation to risk of stroke in women. Am. J. Epidemiol. 2005, 161, 161–169. [Google Scholar] [CrossRef] [PubMed]
- Oba, S.; Nagata, C.; Nakamura, K.; Fujii, K.; Kawachi, T.; Takatsuka, N.; Shimizu, H. Dietary glycemic index, glycemic load, and intake of carbohydrate and rice in relation to risk of mortality from stroke and its subtypes in Japanese men and women. Metabolism 2010, 59, 1574–1582. [Google Scholar] [CrossRef] [PubMed]
- McKeown, N.M.; Meigs, J.B.; Liu, S.; Saltzman, E.; Wilson, P.W.F.; Jacques, P.F. Carbohydrate nutrition, insulin resistance, and the prevalence of the metabolic syndrome in the Framingham Offspring Cohort. Diabetes Care 2004, 27, 538–546. [Google Scholar] [CrossRef] [PubMed]
- Venn, B.J.; Green, T.J. Glycemic index and glycemic load: Measurement issues and their effect on diet-disease relationships. Eur. J. Clin. Nutr. 2007, 61, S122–S131. [Google Scholar] [CrossRef] [PubMed]
- Hannah, B.; Mallard, S.; Venn, B. Glycemic differences between white and whole grain bread but no differences in glycemic response between sandwiches made with these breads, implications for dietetic advice. J. Diabetes Metab. 2014, 5. [Google Scholar] [CrossRef]
- Vitaglione, P.; Lumaga, R.B.; Stanzione, A.; Scalfi, L.; Fogliano, V. beta-Glucan-enriched bread reduces energy intake and modifies plasma ghrelin and peptide YY concentrations in the short term. Appetite 2009, 53, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Weickert, M.O.; Spranger, J.; Holst, J.J.; Otto, B.; Koebnick, C.; Möhlig, M.; Pfeiffer, A.F. Wheat-fibre-induced changes of postprandial peptide YY and ghrelin responses are not associated with acute alterations of satiety. Br. J. Nutr. 2006, 96, 795–798. [Google Scholar] [CrossRef] [PubMed]
- An, Z.M.; Zhang, L.; Zhang, M.; Huang, M.J.; Xiong, Z.Y.; Zhang, G.F. The response of serum ghrelin and PYY to oral glucose and steamed-bread tolerance test in nonobese and obese patients with type 2 diabetes. Sichuan Da Xue Xue Bao Yi Xue Ban 2008, 39, 772–775. [Google Scholar] [PubMed]
- Skrabanja, V.; Liljeberg Elmståhl, H.G.; Kreft, I.; Björck, I.M. Nutritional properties of starch in buckwheat products: Studies in vitro and in vivo. J. Agric. Food. Chem. 2001, 49, 490–496. [Google Scholar] [CrossRef] [PubMed]
- Holt, S.H.; Brand-Miller, J.C.; Stitt, P.A. The effects of equal-energy portions of different breads on blood glucose levels, feeling of fullness and subsequent food intake. J. Am. Diet. Assoc. 2006, 101, 767–773. [Google Scholar] [CrossRef]
- Lee, Y.P.; Mori, T.A.; Sipsas, S.; Barden, A.; Puddey, I.B.; Burke, V.; Hall, R.S.; Hodgson, J.M. Lupin-enriched bread increases satiety and reduces energy intake acutely. Am. J. Clin. Nutr. 2006, 84, 975–980. [Google Scholar] [PubMed]
- Kristensen, M.; Jensen, M.G.; Riboldi, G.; Petronio, M.; Bügel, S.; Toubro, S.; Tetens, I.; Astrup, A. Wholegrain versus refined wheat bread and pasta. Effect on postprandial glycemia, appetite, and subsequent ad libitum energy intake in young healthy adults. Appetite 2010, 54, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Isaksson, H.; Rakha, A.; Andersson, R.; Fredriksson, H.; Olsson, J.; Aman, P. Rye kernel breakfast increases satiety in the afternoon—An effect of food structure. Nutr. J. 2011, 11, 10–31. [Google Scholar]
- Forsberg, T.; Åman, P.; Landberg, R. Effects of whole grain rye crisp bread for breakfast on appetite and energy intake in a subsequent meal: Two randomised controlled trials with different amounts of test foods and breakfast energy content. Nutr. J. 2014, 25, 13–26. [Google Scholar]
- Johnson, S.K.; Thomas, S.J.; Hall, R.S. Palatability and glucose, insulin and satiety responses of chickpea flour and extruded chickpea flour bread eaten as part of a breakfast. Eur. J. Clin. Nutr. 2005, 59, 169–176. [Google Scholar] [CrossRef] [PubMed]
- Bodinham, C.L.; Hitchen, K.L.; Youngman, P.J.; Frost, G.S.; Robertson, M.D. Short-term effects of whole-grain wheat on appetite and food intake in healthy adults: A pilot study. Br. J. Nutr. 2011, 106, 327–330. [Google Scholar] [CrossRef] [PubMed]
- Breen, C.; Ryan, M.; Gibney, M.J.; Corrigan, M.; O’Shea, D. Glycemic, insulinemic, and appetite responses of patients with type 2 diabetes to commonly consumed breads. Diabetes Educ. 2013, 39, 376–386. [Google Scholar] [CrossRef] [PubMed]
- Encuesta Nacional de Ingesta Dietética Española (ENIDE) 2011. Agencia Española de Consumo, Seguridad Alimentaria y Nutrición (AESAN). Available online: http://aesan.msssi.gob.es/AESAN/docs/docs/notas_prensa/Presentacion_ENIDE.pdf (accessed on 27 January 2015).
- Sørensen, L.B.; Møller, P.; Flint, A.; Martens, M.; Raben, A. Effect of sensory perception of foods on appetite and food intake: A review of studies on humans. Int. J. Obes. Relat. Metab. Disord. 2003, 27, 1152–1166. [Google Scholar] [CrossRef] [PubMed]
- Leeman, M.; Ostman, E.; Björck, I. Glycaemic and satiating properties of potato products. Eur. J. Clin. Nutr. 2008, 62, 87–95. [Google Scholar] [CrossRef] [PubMed]
- Clegg, M.E.; Ranawana, V.; Shafat, A.; Henry, C.J. Soups increase satiety through delayed gastric emptying yet increased glycaemic response. Eur. J. Clin. Nutr. 2013, 67, 8–11. [Google Scholar] [CrossRef] [PubMed]
- Holt, S.; Brand, J.; Soveny, C.; Hansky, J. Relationship of satiety to postprandial glycaemic, insulin and cholecystokinin responses. Appetite 1992, 18, 129–141. [Google Scholar] [CrossRef] [PubMed]
- Gibbons, C.; Caudwell, P.; Finlayson, G.; Webb, D.L.; Hellström, P.M.; Näslund, E.; Blundell, J.E. Comparison of postprandial profiles of ghrelin, active GLP-1, and total PYY to meals varying in fat and carbohydrate and their association with hunger and the phases of satiety. J. Clin. Endocrinol. Metab. 2013, 98, 847–855. [Google Scholar] [CrossRef]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gonzalez-Anton, C.; Rico, M.C.; Sanchez-Rodriguez, E.; Ruiz-Lopez, M.D.; Gil, A.; Mesa, M.D. Glycemic Responses, Appetite Ratings and Gastrointestinal Hormone Responses of Most Common Breads Consumed in Spain. A Randomized Control Trial in Healthy Humans. Nutrients 2015, 7, 4033-4053. https://doi.org/10.3390/nu7064033
Gonzalez-Anton C, Rico MC, Sanchez-Rodriguez E, Ruiz-Lopez MD, Gil A, Mesa MD. Glycemic Responses, Appetite Ratings and Gastrointestinal Hormone Responses of Most Common Breads Consumed in Spain. A Randomized Control Trial in Healthy Humans. Nutrients. 2015; 7(6):4033-4053. https://doi.org/10.3390/nu7064033
Chicago/Turabian StyleGonzalez-Anton, Carolina, Maria C. Rico, Estefania Sanchez-Rodriguez, Maria D. Ruiz-Lopez, Angel Gil, and Maria D. Mesa. 2015. "Glycemic Responses, Appetite Ratings and Gastrointestinal Hormone Responses of Most Common Breads Consumed in Spain. A Randomized Control Trial in Healthy Humans" Nutrients 7, no. 6: 4033-4053. https://doi.org/10.3390/nu7064033