Effects of Vitamin D Supplementation on Serum 25-Hydroxyvitamin D Concentrations in Cirrhotic Patients: A Randomized Controlled Trial

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
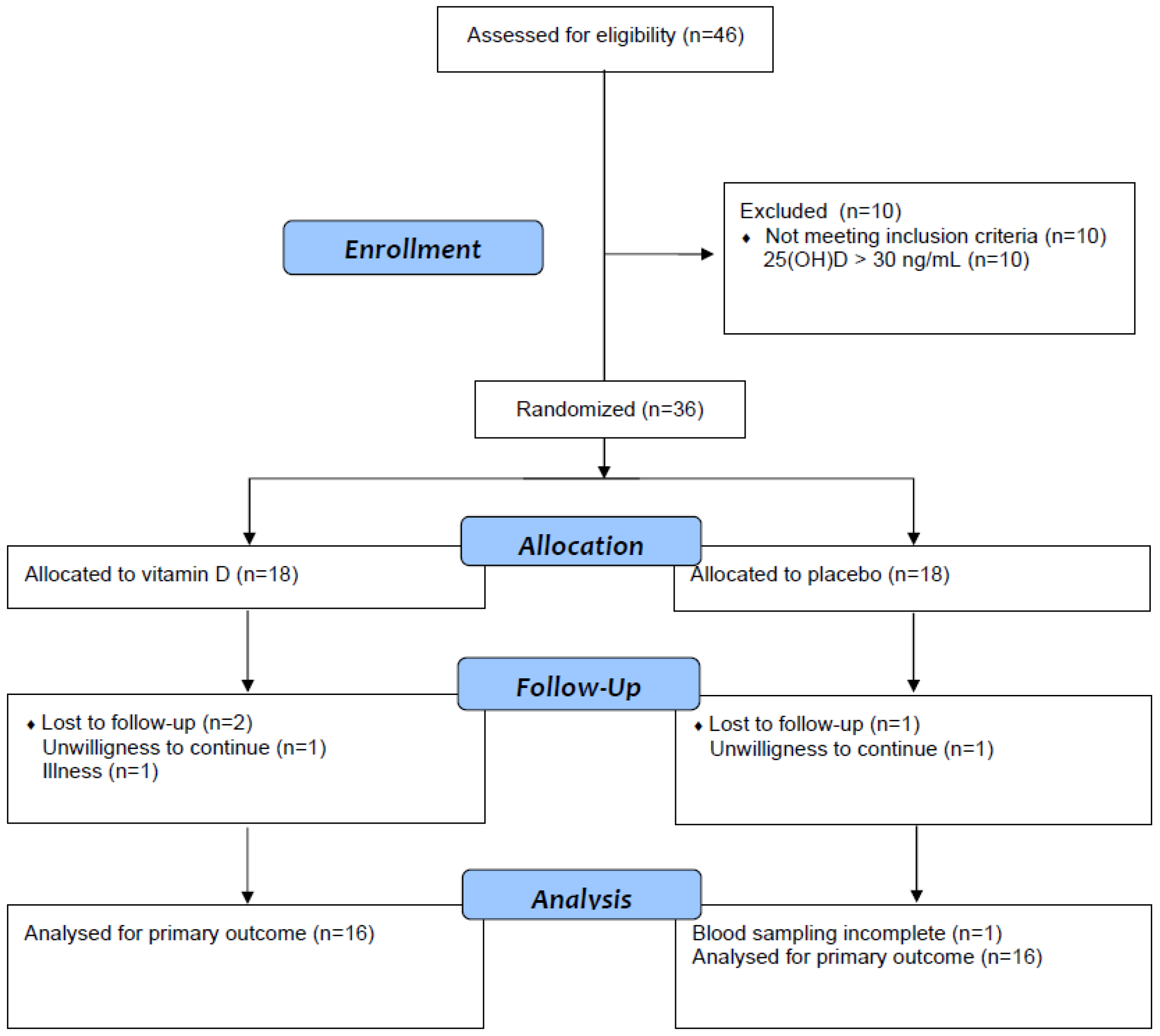
2.2. Participants
2.3. Intervention
2.4. Primary Outcome Measure
2.5. Secondary Outcome Measures
2.6. Measurements
2.7. Statistical Analysis
3. Results
4. Discussion
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Eliades, M.; Spyrou, E. Vitamin D: A new player in non-alcoholic fatty liver disease? World J. Gastroenterol. 2015, 21, 1718–1727. [Google Scholar] [CrossRef] [PubMed]
- Stokes, C.S.; Volmer, D.A.; Grünhage, F.; Lammert, F. Vitamin D in chronic liver disease. Liver Int. 2013, 33, 338–352. [Google Scholar] [CrossRef] [PubMed]
- Ross, A.C.; Manson, J.E.; Abrams, S.A.; Aloia, J.F.; Brannon, P.M.; Clinton, S.K.; Durazo-Arvizu, R.A.; Gallagher, J.C.; Gallo, R.L.; Jones, G.; et al. The 2011 report on dietary reference intakes for calcium and vitamin D from the Institute of Medicine: What clinicians need to know. J. Clin. Endocrinol. Metab. 2011, 96, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M. Guidelines for preventing and treating vitamin D deficiency and insufficiency revisited. J. Clin. Endocrinol. Metab. 2012, 97, 1153–1158. [Google Scholar] [CrossRef] [PubMed]
- Pludowski, P.; Holick, M.F.; Pilz, S.; Wagner, C.L.; Hollis, B.W.; Grant, W.B.; Shoenfeld, Y.; Lerchbaum, E.; Llewellyn, D.J.; Kienreich, K.; et al. Vitamin D effects on musculoskeletal health, immunity, autoimmunity, cardiovascular disease, cancer, fertility, pregnancy, dementia and mortality-A review of recent evidence. Autoimmun. Rev. 2013, 12, 976–989. [Google Scholar] [CrossRef] [PubMed]
- Autier, P.; Boniol, M.; Pizot, C.; Mullie, P. Vitamin D status and ill health: A systematic review. Lancet Diabetes Endocrinol. 2014, 2, 76–89. [Google Scholar] [CrossRef]
- Rosen, C.J.; Adams, J.S.; Bikle, D.D.; Black, D.M.; Demay, M.B.; Manson, J.E.; Murad, M.H.; Kovacs, C.S. The nonskeletal effects of vitamin D: An Endocrine Society scientific statement. Endocr. Rev. 2012, 33, 456–492. [Google Scholar] [CrossRef] [PubMed]
- Kienreich, K.; Tomaschitz, A.; Verheyen, N.; Pieber, T.; Gaksch, M.; Grübler, M.R.; Pilz, S. Vitamin D and cardiovascular disease. Nutrients 2013, 5, 3005–3021. [Google Scholar] [CrossRef] [PubMed]
- Mouli, V.P.; Ananthakrishnan, A.N. Review article: Vitamin D and inflammatory bowel diseases. Aliment. Pharmacol. Ther. 2014, 39, 125–136. [Google Scholar] [CrossRef] [PubMed]
- Wallace, I.R.; Wallace, H.J.; McKinley, M.C.; Bell, P.M.; Hunter, S.J. Vitamin D and insulin resistance. Clin. Endocrinol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Alvarez, J.A.; Chowdhury, R.; Jones, D.P.; Martin, G.S.; Brigham, K.L.; Binongo, J.N.; Ziegler, T.R.; Tangpricha, V. Vitamin D status is independently associated with plasma glutathione and cysteine thiol/disulphide redox status in adults. Clin. Endocrinol. (Oxf.) 2014, 81, 458–466. [Google Scholar] [CrossRef] [PubMed]
- Putz-Bankuti, C.; Pilz, S.; Stojakovic, T.; Scharnagl, H.; Pieber, T.R.; Trauner, M.; Obermayer-Pietsch, B.; Stauber, R.E. Association of 25-hydroxyvitamin D levels with liver dysfunction and mortality in chronic liver disease. Liver Int. 2012, 32, 845–851. [Google Scholar] [CrossRef] [PubMed]
- Finkelmeier, F.; Kronenberger, B.; Köberle, V.; Bojunga, J.; Zeuzem, S.; Trojan, J.; Piiper, A.; Waidmann, O. Severe 25-hydroxyvitamin D deficiency identifies a poor prognosis in patients with hepatocellular carcinoma - a prospective cohort study. Aliment. Pharmacol. Ther. 2014, 39, 1204–1212. [Google Scholar] [CrossRef] [PubMed]
- Song, B.J.; Rockey, D.C. Status of research on vitamin D supplementation in treating or preventing liver fibrosis. Liver Int. 2013, 33, 653–655. [Google Scholar] [CrossRef] [PubMed]
- Eliades, M.; Spyrou, E.; Agrawal, N.; Lazo, M.; Brancati, F.L.; Potter, J.J.; Koteish, A.A.; Clark, J.M.; Guallar, E.; Hernaez, R. Meta-analysis: Vitamin D and non-alcoholic fatty liver disease. Aliment. Pharmacol. Ther. 2013, 38, 246–254. [Google Scholar] [CrossRef] [PubMed]
- Dasarathy, J.; Periyalwar, P.; Allampati, S.; Bhinder, V.; Hawkins, C.; Brandt, P.; Khiyami, A.; McCullough, A.J.; Dasarathy, S. Hypovitaminosis D is associated with increased whole body fat mass and greater severity of non-alcoholic fatty liver disease. Liver Int. 2014, 34, e118–e127. [Google Scholar] [CrossRef] [PubMed]
- Malham, M.; Peter Jørgensen, S.; Lauridsen, A.L.; Ott, P.; Glerup, H.; Dahlerup, J.F. The effect of a single oral megadose of vitamin D provided as either ergocalciferol (D2) or cholecalciferol (D3) in alcoholic liver cirrhosis. Eur. J. Gastroenterol. Hepatol. 2012, 24, 172–178. [Google Scholar] [CrossRef] [PubMed]
- Crawford, B.A.; Labio, E.D.; Strasser, S.I.; McCaughan, G.W. Vitamin D replacement for cirrhosis-related bone disease. Nat. Clin. Pract. Gastroenterol. Hepatol. 2006, 3, 689–699. [Google Scholar] [CrossRef] [PubMed]
- Sharifi, N.; Amani, R.; Hajiani, E.; Cheraghian, B. Does vitamin D improve liver enzymes, oxidative stress, and inflammatory biomarkers in adults with non-alcoholic fatty liver disease? A randomized clinical trial. Endocrine 2014, 47, 70–80. [Google Scholar] [CrossRef] [PubMed]
- Chaney, A.; Heckman, M.G.; Diehl, N.N.; Meek, S.; Keaveny, A.P. Effectiveness and Outcomes of Current Practice in Treating Vitamin D Deficiency in Patients Listed for Liver Transplantation. Endocr. Pract. 2015, 21, 761–769. [Google Scholar] [CrossRef] [PubMed]
- Nimer, A.; Mouch, A. Vitamin D improves viral response in hepatitis C genotype 2–3 naïve patients. World J. Gastroenterol. 2012, 18, 800–805. [Google Scholar] [CrossRef] [PubMed]
- Foroughi, M.; Maghsoudi, Z.; Ghiasvand, R.; Iraj, B.; Askari, G. Effect of Vitamin D Supplementation on C-reactive Protein in Patients with Nonalcoholic Fatty Liver. Int. J. Prev. Med. 2014, 5, 969–975. [Google Scholar] [PubMed]
- Esmat, G.; El Raziky, M.; Elsharkawy, A.; Sabry, D.; Hassany, M.; Ahmed, A.; Assem, N.; El Kassas, M.; Doss, W. Impact of vitamin D supplementation on sustained virological response in chronic hepatitis C genotype 4 patients treated by pegylated interferon/ribavirin. J. Interferon Cytokine Res. 2015, 35, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Ladero, J.M.; Torrejón, M.J.; Sánchez-Pobre, P.; Suárez, A.; Cuenca, F.; de la Orden, V.; Devesa, M.J.; Rodrigo, M.; Estrada, V.; López-Alonso, G.; et al. Vitamin D deficiency and vitamin D therapy in chronic hepatitis C. Ann. Hepatol. 2013, 12, 199–204. [Google Scholar] [PubMed]
- Rostami, S.; Parsian, H. Hyaluronic Acid: From biochemical characteristics to its clinical translation in assessment of liver fibrosis. Hepat. Mon. 2013, 13, e13787. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Hopewell, S.; Schulz, K.F.; Montori, V.; Gøtzsche, P.C.; Devereaux, P.J.; Elbourne, D.; Egger, M.; Altman, D.G. CONSORT 2010 explanation and elaboration: Updated guidelines for reporting parallel group randomised trials. BMJ 2010, 340, c869. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- US National Library of Science. Clinicaltrials.gov. Available online: https://clinicaltrials.gov/ct2/show/NCT02009748 (accessed on 6 May 2016).
- Randomizer: A Web-Based Patient Randomization (Randomisation) Service for Clinical Trials Provided by the Medical University of Graz. Available online: https://www.randomizer.at/ (accessed on 6 May 2016).
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of Diet in Renal Disease Study Group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Rosenberg, W.M.; Voelker, M.; Thiel, R.; Becka, M.; Burt, A.; Schuppan, D.; Hubscher, S.; Roskams, T.; Pinzani, M.; Arthur, M.J.; et al. European Liver Fibrosis Group. Serum markers detect the presence of liver fibrosis: A cohort study. Gastroenterology 2004, 127, 1704–1713. [Google Scholar] [CrossRef] [PubMed]
- Pugh, R.N.; Murray-Lyon, I.M.; Dawson, J.L.; Pietroni, M.C.; Williams, R. Transection of the oesophagus for bleeding oesophageal varices. Br. J. Surg. 1973, 60, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Kamath, P.S.; Wiesner, R.H.; Malinchoc, M.; Kremers, W.; Therneau, T.M.; Kosberg, C.L.; D’Amico, G.; Dickson, E.R.; Kim, W.R. A model to predict survival in patients with end-stage liver disease. Hepatology 2001, 33, 464–470. [Google Scholar] [CrossRef] [PubMed]
- Vickers, A.J.; Altman, D.G. Statistics notes: Analysing controlled trials with baseline and follow up measurements. BMJ 2001, 323, 1123–1124. [Google Scholar] [CrossRef] [PubMed]
- Pilz, S.; Gaksch, M.; Kienreich, K.; Grübler, M.; Verheyen, N.; Fahrleitner-Pammer, A.; Treiber, G.; Drechsler, C.; Ó Hartaigh, B.; Obermayer-Pietsch, B.; et al. Effects of vitamin d on blood pressure and cardiovascular risk factors: A randomized controlled trial. Hypertension 2015, 65, 1195–1201. [Google Scholar] [CrossRef] [PubMed]
- Agmon-Levin, N.; Kopilov, R.; Selmi, C.; Nussinovitch, U.; Sánchez-Castañón, M.; López-Hoyos, M.; Amital, H.; Kivity, S.; Gershwin, E.M.; Shoenfeld, Y. Vitamin D in primary biliary cirrhosis, a plausible marker of advanced disease. Immunol. Res. 2015, 61, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.C.; Bikle, D.D.; Lizaola, B.; Hayssen, H.; Terrault, N.A.; Schwartz, J.B. Total 25(OH) vitamin D, free 25(OH) vitamin D and markers of bone turnover in cirrhotics with and without synthetic dysfunction. Liver Int. 2015, 35, 2294–2300. [Google Scholar] [CrossRef] [PubMed]
- Gatta, A.; Verardo, A.; Di Pascoli, M.; Giannini, S.; Bolognesi, M. Hepatic osteodystrophy. Clin. Cases Miner. Bone Metab. 2014, 11, 185–191. [Google Scholar] [CrossRef] [PubMed]
- Carter, G.D.; Jones, J.C.; Shannon, J.; Williams, E.L.; Jones, G.; Kaufmann, M.; Sempos, C. 25-Hydroxyvitamin D assays: Potential interference from other circulating vitamin D metabolites. J. Steroid Biochem. Mol. Biol. 2015. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, J.B.; Lai, J.; Lizaola, B.; Kane, L.; Weyland, P.; Terrault, N.A.; Stotland, N.; Bikle, D. Variability in free 25(OH) vitamin D levels in clinical populations. J. Steroid Biochem. Mol. Biol. 2014, 144, 156–158. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Characteristics | All (n = 36) | Vitamin D (n = 18) | Placebo (n = 18) | p Value |
|---|---|---|---|---|
| Females (%) | 25 | 33 | 17 | 0.248 |
| Age (years) | 61 ± 9 | 63 ± 9 | 58 ± 9 | 0.110 |
| Body mass index (kg/m²) | 26.9 ± 4.4 | 27.9 ± 5.2 | 26.0 ± 3.3 | 0.204 |
| Alcoholic cirrhosis (%) | 64 | 67 | 61 | 0.729 |
| MELD score | 9 (8–12) | 10 (8–12) | 9 (7–10) | 0.136 |
| Child Pugh score | 5 (5-6) | 5 (5–6) | 5 (5–5) | 0.570 |
| AST (IU/L) | 39 (30–61) | 52 (32–61) | 37 (26–59) | 0.448 |
| ALT (IU/L) | 34 (22–46) | 35 (27–44) | 29 (20–49) | 0.874 |
| GGT (IU/L) | 106 (71–201) | 97 (46–240) | 113 (74–180) | 0.967 |
| AP (IU/L) | 99 (79–127) | 105 (78–149) | 93 (80–114) | 0.341 |
| Albumin (g/dL) | 4.0 ± 0.5 | 4.0 ± 0.4 | 4.0 ± 0.6 | 0.642 |
| INR | 1.21 (1.09–1.35) | 1.29 (1.15–1.36) | 1.17 (1.08–1.32) | 0.102 |
| Bilirubin (mg/dL) | 0.8 (0.6–1.3) | 1.0 (0.7–1.4) | 0.7 (0.5–1.1) | 0.104 |
| Hyaluronic acid (ng/mL) | 270 (83–536) | 328 (166–1000) | 266 (67–488) | 0.164 |
| ELF score | 11.2 ± 1.3 | 11.5 ± 1.3 | 10.9 ± 1.1 | 0.125 |
| Creatinine (mg/dL) | 0.85 (0.78–0.99) | 0.85 (0.76–0.99) | 0.86 (0.77–1.01) | 0.864 |
| eGFR (ml/min/1.73 m²) | 92 ± 25 | 89 ± 23 | 94 ± 27 | 0.521 |
| Platelet count (109/L) | 116 (87–153) | 116 (70–155) | 121 (90–162) | 0.661 |
| Triglycerides (mg/dL) | 118 (76–149) | 105 (69–150) | 121 (89–146) | 0.944 |
| HDL-cholesterol (mg/dL) | 44 ± 15 | 42 ± 17 | 45 ± 13 | 0.557 |
| LDL-cholesterol (mg/dL) | 100 ± 32 | 95 ± 31 | 105 ± 34 | 0.396 |
| Total cholesterol (mg/dL) | 172 ± 41 | 166 ± 43 | 178 ± 40 | 0.420 |
| CRP (mg/L) | 3.2 (1.2–7.4) | 2.7 (1.2–7.9) | 3.7 (1.1–6.8) | 0.988 |
| 25(OH)D (ng/mL) | 15.7 ± 7.2 | 15.9 ± 7.5 | 15.5 ± 7.0 | 0.882 |
| PTH (pg/mL) | 40.7 ± 15.5 | 39.2 ± 11.2 | 42.1 ± 19.0 | 0.596 |
| Total plasma calcium (mmol/L) | 2.33 ± 0.11 | 2.32 ± 0.09 | 2.35 ± 0.12 | 0.557 |
| Free plasma calcium (mmol/L) | 1.16 ± 0.05 | 1.16 ± 0.05 | 1.16 ± 0.04 | 1.000 |
| Plasma phosphate (mmol/L) | 1.01 ± 0.19 | 1.00 ± 0.22 | 1.02 ± 0.16 | 0.834 |
| Urinary calcium/creatinine ratio | 0.26 (0.16–0.36) | 0.31 (0.14–0.46) | 0.25 (0.16–0.30) | 0.608 |
| Plasma sodium (mmol/L) | 139 (137–141) | 139 (138–140) | 139 (137–141) | 0.869 |
| Calcium/Vitamin D supplement (%) | 6 | 11 | 0 | 0.486 |
| Diuretics (%) | 53 | 61 | 44 | 0.317 |
| Characteristics | Baseline | Follow-up | Mean Change from Baseline | Treatment Effect | p Value |
|---|---|---|---|---|---|
| 25-hydroxyvitamin D (ng/mL) | |||||
| Vitamin (n = 16) | 15.8 ± 7.8 | 33.8 ± 10.3 | 18.0 (11.4 to 24.6) | 15. 2 (8.0 to 22.4) | <0.001 |
| Placebo (n = 16) | 15.8 ± 7.4 | 18.6 ± 9.9 | 2.8 (−2.3 to 7.9) | ||
| AST (IU/L) # | |||||
| Vitamin (n = 16) | 52 (33–62) | 51 (35–67) | 1 (−7 to 10) | 0 (−13 to 13) | 0.663 |
| Placebo (n = 17) | 37 (25–61) | 47 (28–61) | 2 (−12 to 16) | ||
| ALT (IU/L) # | |||||
| Vitamin (n = 16) | 39 (29–46) | 36 (29–52) | 0 (−5 to 6) | −1 (−17 to 14) | 0.962 |
| Placebo (n = 17) | 28 (20–46) | 30 (20–39) | 1 (−13 to 16) | ||
| GGT (IU/L) # | |||||
| Vitamin (n = 16) | 97 (44–314) | 100 (55–288) | 4 (−17 to 24) | 1 (−36 to 38) | 0.440 |
| Placebo (n = 17) | 122 (74–192) | 139 (56–225) | 4 (−27 to 35) | ||
| AP (IU/L) # | |||||
| Vitamin (n=16) | 112 (79–176) | 124 (75–180) | 5 (−8 to 18) | 8 (−10 to 25) | 0.700 |
| Placebo (n=17) | 88 (80–118) | 98 (75–105) | −2 (−13 to 8) | ||
| Albumin (g/dL) | |||||
| Vitamin (n = 16) | 4.0 ± 0.4 | 3.9 ± 0.5 | −0.2 (−0.4 to 0.0) | −0.1 (−0.3 to 0.1) | 0.366 |
| Placebo (n = 17) | 4.0 ± 0.6 | 4.0 ± 0.5 | −0.1 (−0.2 to 0.2) | ||
| INR # | |||||
| Vitamin (n = 16) | 1.27 (1.14–1.39) | 1.24 (1.12–1.45) | 0.08 (−0.11 to 0.26) | 0.06 (−0.14 to 0.25) | 0.610 |
| Placebo (n = 15) | 1.18 (1.08–1.39) | 1.18 (1.10–1.29) | 0.00 (−0.05 to 0.04) | ||
| Bilirubin (mg/dL) # | |||||
| Vitamin (n = 16) | 1.1 (0.8–1.5) | 1.0 (0.8–1.4) | −0.2 (−0.5 to 0.2) | 0.2 (−0.1 to 0.4) | 0.628 |
| Placebo (n = 17) | 0.7 (0.5–1.1) | 0.6 (0.5–1.0) | −0.2 (−0.4 to 0.1) | ||
| Hyaluronic acid (ng/mL) # | |||||
| Vitamin (n = 16) | 328 (182–911) | 367 (135–844) | 30 (−44 to 104) | −39 (−155 to 77) | 0.599 |
| Placebo (n = 15) | 266 (72–517) | 411 (78–593) | 75 (−16 to 166) | ||
| ELF score | |||||
| Vitamin (n = 16) | 11.5 ± 1.2 | 11.7 ± 1.2 | 0.2 (−0.1 to 0.4) | 0.0 (−0.4 to 0.3) | 0.836 |
| Placebo (n = 16) | 10.9 ± 1.1 | 11.1 ± 1.2 | 0.2 (0.0 to 0.5) | ||
| Characteristics | Baseline | Follow-up | Mean Change from Baseline | Treatment Effect | p Value |
|---|---|---|---|---|---|
| PTH (pg/mL) | |||||
| Vitamin (n = 16) | 38.8 ± 11.3 | 38.5 ± 15.1 | −0.3 (−8.0 to 7.3) | −2.3 (−10.0 to 5.4) | 0.548 |
| Placebo (n = 16) | 41.5 ± 20.1 | 42.6 ± 15.3 | 1.1 (−3.3 to 5.5) | ||
| Total plasma calcium (mmol/L) | |||||
| Vitamin (n = 16) | 2.33 ± 0.09 | 2.27 ± 0.07 | −0.06 (−1.0 to −0.02) | 0.00 (−0.05 to 0.04) | 0.849 |
| Placebo (n = 17) | 2.34 ± 0.11 | 2.28 ± 0.12 | −0.05 (-0.09 to 0.02) | ||
| Free plasma calcium (mmol/L) | |||||
| Vitamin (n = 16) | 1.15 ± 0.05 | 1.15 ± 0.05 | −0.01 (−0.03 to 0.02) | 0.02 (−0.02 to 0.05) | 0.254 |
| Placebo (n = 17) | 1.15 ± 0.05 | 1.13 ± 0.06 | −0.02 (−0.05 to 0.00) | ||
| Urinary midstream calcium to creatinine ratio # | |||||
| Vitamin (n = 13) | 0.31 (0.12–0.43) | 0.29 (0.14–0.54) | −0.06 (−0.31 to 0.18) | 0.00 (−0.27 to 0.28) | 0.354 |
| Placebo (n = 17) | 0.25 (0.19–0.31) | 0.19 (0.09–0.29) | 0.04 (−0.18 to 0.25) | ||
| Plasma phosphate (mmol/L) | |||||
| Vitamin (n = 16) | 0.99 ± 0.22 | 1.03 ± 0.20 | 0.04 (−0.05 to 0.12) | 0.04 (−0.60 to 0.13) | 0.448 |
| Placebo (n = 17) | 1.02 ± 0.17 | 1.01 ± 0.14 | −0.01 (−0.09 to 0.07) | ||
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pilz, S.; Putz-Bankuti, C.; Gaksch, M.; Spindelboeck, W.; Haselberger, M.; Rainer, F.; Posch, A.; Kreuzer, P.; Stojakovic, T.; Stadlbauer, V.; et al. Effects of Vitamin D Supplementation on Serum 25-Hydroxyvitamin D Concentrations in Cirrhotic Patients: A Randomized Controlled Trial. Nutrients 2016, 8, 278. https://doi.org/10.3390/nu8050278
Pilz S, Putz-Bankuti C, Gaksch M, Spindelboeck W, Haselberger M, Rainer F, Posch A, Kreuzer P, Stojakovic T, Stadlbauer V, et al. Effects of Vitamin D Supplementation on Serum 25-Hydroxyvitamin D Concentrations in Cirrhotic Patients: A Randomized Controlled Trial. Nutrients. 2016; 8(5):278. https://doi.org/10.3390/nu8050278
Chicago/Turabian StylePilz, Stefan, Csilla Putz-Bankuti, Martin Gaksch, Walter Spindelboeck, Marius Haselberger, Florian Rainer, Andreas Posch, Philipp Kreuzer, Tatjana Stojakovic, Vanessa Stadlbauer, and et al. 2016. "Effects of Vitamin D Supplementation on Serum 25-Hydroxyvitamin D Concentrations in Cirrhotic Patients: A Randomized Controlled Trial" Nutrients 8, no. 5: 278. https://doi.org/10.3390/nu8050278