1. Introduction
In the late nineties, in a regional Asian effort to advocate on the importance of malnutrition, the United Nations Children’s Emergency Fund (UNICEF) and the Asian Development bank assessed the impact of malnutrition on the economy in seven countries. It was concluded that malnutrition, with its insidious effect over the life span of a child, will cost the economies at least 3% of their gross domestic product (GDP) [
1]. Malnutrition, such as micronutrient deficiencies, has been more and more associated with economic productivity losses [
2,
3]. The World Bank estimated that the combined economic cost of iron deficiency, iodine deficiency, and vitamin A deficiency in developing countries could waste as much as 5% of the GDP [
4], while Horton and Ross estimated that iron-deficiency anemia alone could cost an average loss of 4.5% of the GDP [
2]. The recently published Global Nutrition Report 2015 reported on a study estimating a reduction of 10.3% in GDP in Malawi due to malnutrition [
5].
Cambodia’s expanding economy, along with rising incomes and easier access to food, is expected to contribute to the reduction of currently high rates of malnutrition, as reported in 2010 [
6]. According to an economic estimation of the burden of malnutrition in Cambodia using the 2010 Cambodian Demographic Health Survey (CDHS) data led by the Council for Agricultural and Rural Development (CARD), the negative health outcomes from child malnutrition present a heavy economic burden of increased health expenditure coupled with decreased productivity and affect the rights of women and children to be healthy participants in society. The Royal Government of Cambodia, with the support of UNICEF/WFP, estimated that malnutrition has caused an annual loss of over USD 250–400 million to Cambodia’s gross domestic product [
7].
The 2014 CDHS [
8] shows that in nutrition, Cambodia did not meet the 2015 Cambodia Millennium Development Goal (CMDG) targets [
9]. 32.4% and 23.9% of children are still respectively stunted and underweight—in comparison to the set target of 24.5% and 19.2% by 2015. Therefore, the government is currently working to expand a range of low-cost effective nutrition interventions to break the current cycle of increased mortality and poor health, impaired cognitive and physical growth, reduced learning capacity, and ultimately lower work performance, productivity, and earnings.
Regardless of the recent attention in the national policy dialogue and strategies, the nutrition agenda remains under-resourced both by the government and donors, constraining the much-needed scale-up of a life-cycle approach, particularly towards children under 5 years of age. The aim of this article was to re-examine and update the economic implications of malnutrition in Cambodia and lay the ground work for a general consensus among Government and donors on the need to invest in nutrition.
4. Discussion
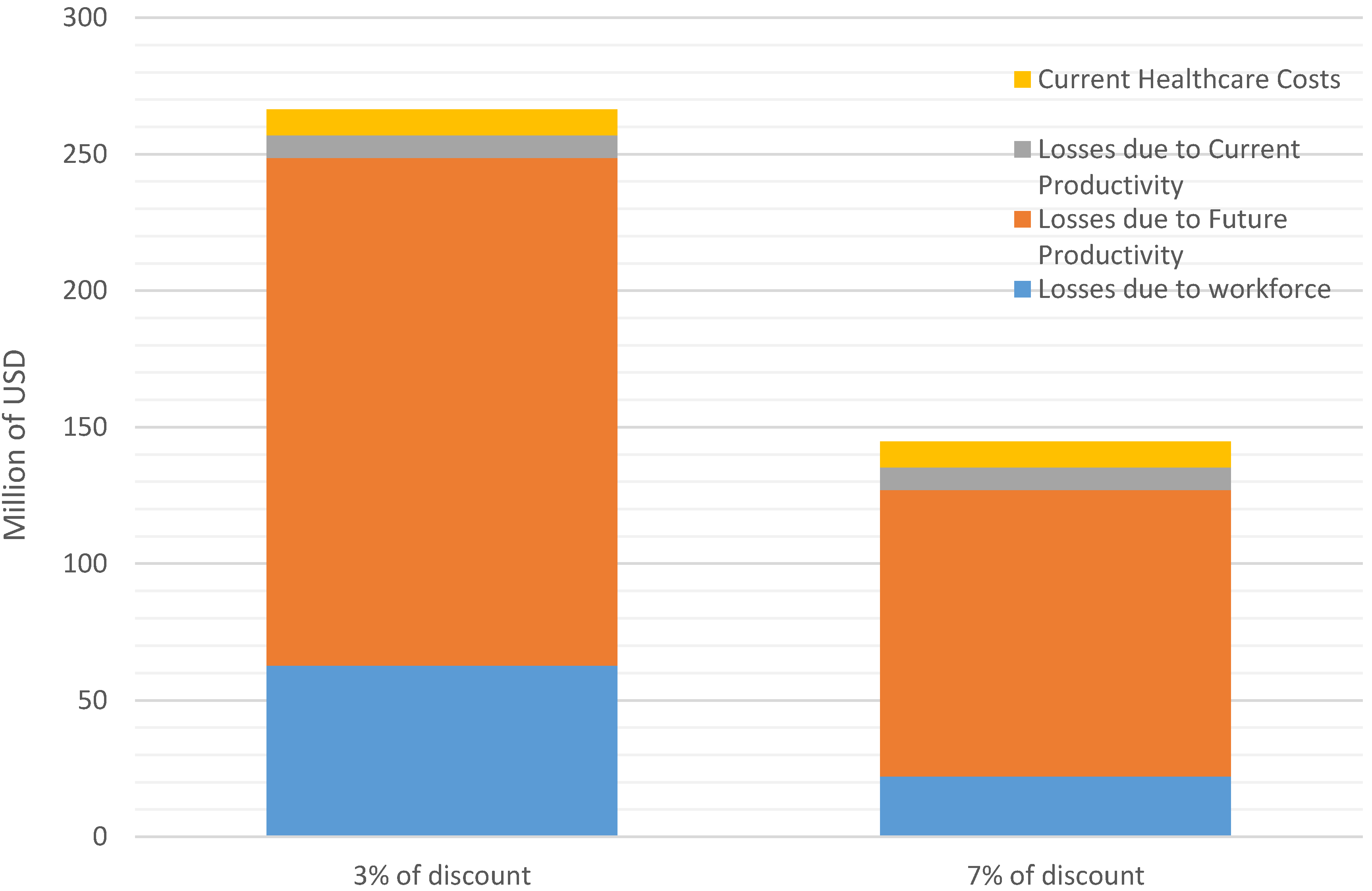
Most of Cambodia’s children face higher than normal risks of dying before their fifth birthday. More than four thousand deaths annually—nearly one-third of all child mortality—is linked to their mother’s nutrition status and breastfeeding behavior, along with child underweight or vitamin and mineral deficiencies. The present value of this lost future workforce is estimated at more than 60 million USD annually (with 3% discount rate). 2.6 million annual cases of diarrhea and respiratory infection among children are attributed to poor breastfeeding practices and zinc deficiencies, resulting in excess costs to the health care system and individual families reaching nearly $8.6 million (with 3% discount rate). Finally, children with less than normal height, iron deficiency or iodine deficiencies suffer deficits in mental and physical development, perform less well in school and consequently, will be less productive as adults, reducing GDP by 186 million USD per year (with 3% discount rate).
In total, according to the 2014 CDHS [
8] and depending on the discount rate, 0.9%–1.7% of the GDP (145–266 million USD) is and will be lost every year due to malnutrition indicators if not tackled. This is below estimations made in other countries such as Laos in Asia (2.4% of the GDP) [
10] and Malawi in Africa (above 10% of GDP) [
5].
The findings of our assessment represent an improvement of 100 million USD less lost in comparison to the previous calculation done with indicators from the 2010 CDHS [
6,
7]. One of the reasons is due to the use of iron deficiency to estimate the economic loss of productivity instead of anemia. It has been assumed that iron deficiency was one of the principal causes for anemia [
34], but recent data have shown that it is not as straight-forward [
23]. A recent published paper in 2015 showed that genetic hemoglobin disorders, rather than iron deficiency, are a major predictor of hemoglobin concentration in women aged 18–45 years in Prey Veng, Cambodia [
35]. The 2014 CDHS is also finding high levels of hemo-globinopathy with only 22% of the children and 47% of the women having a “normal hemoglobin” (hemoglobin A1 > 95%). Therefore, in 2010 there might have been an overestimation of the economic burden of anemia due to iron deficiency. However, the loss of productivity because of anemia remains. The anemia prevalence has not declined from 2010 to 2014 [
6,
8], but most of it has no relationship with nutrition deficiencies.
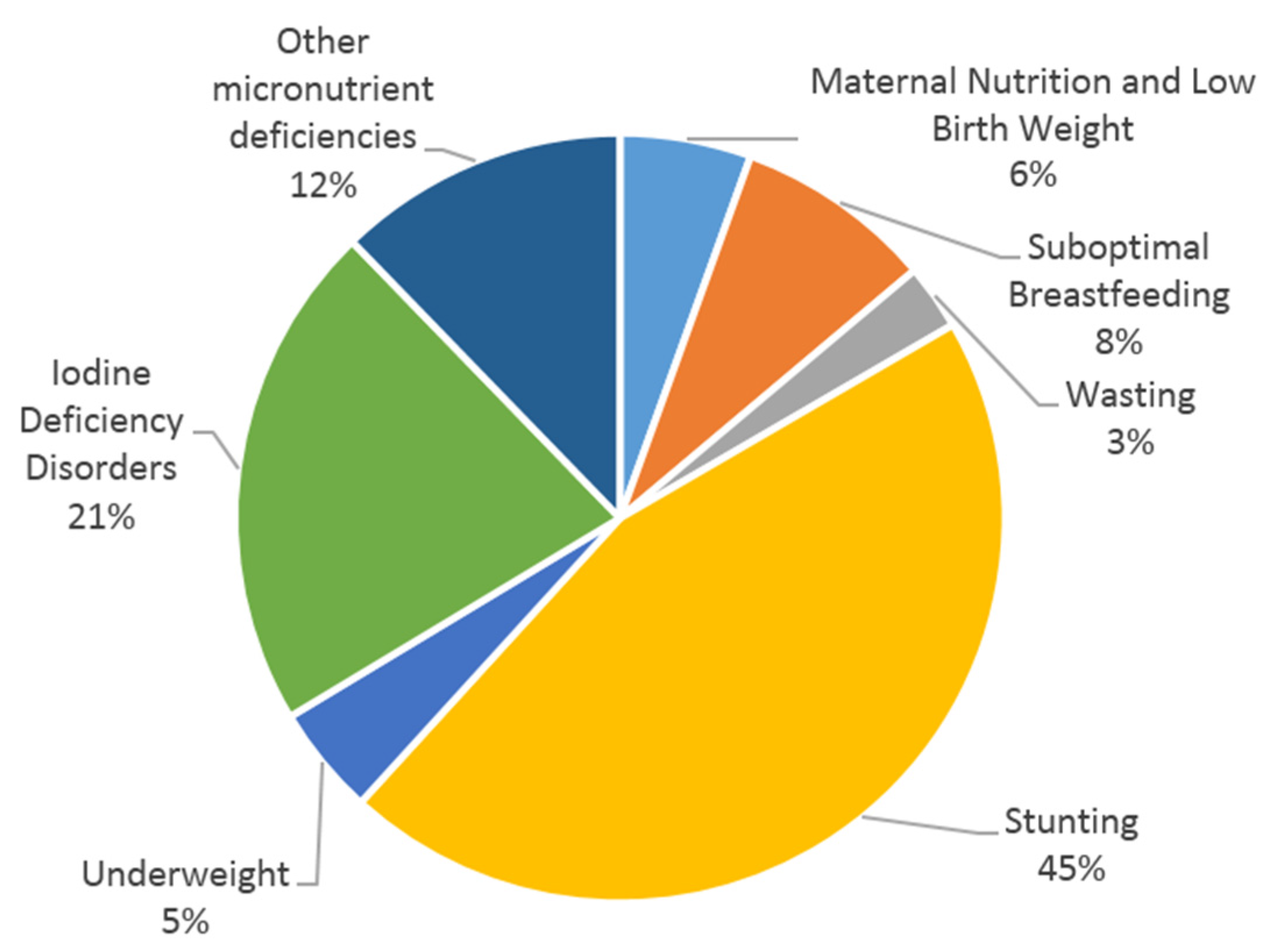
Most of the projected losses (45%) are linked to stunting. Similar findings were observed in Albania, where stunting represented also approximately 50% of the economic losses [
11]. Childhood stunting is one of the most significant obstacles to human development, as it is a well-established risk marker of poor child development [
36]. If Cambodia follows the 40% goal reduction in stunting, set forward for 2025 by the World Health Assembly [
36], the government could prevent a yearly loss of approximately 50 million USD. To do so, many complementary strategies to improve nutrition need to be considered, including: (i) reduce wasting [
37]; (ii) reduce low birth weight; and (iii) increase appropriate feeding practices during pregnancy and in children under 5 years of age [
38,
39]. It is also important to address relevant agriculture and health related issues, but also water, sanitation, and hygiene (WASH) in a more comprehensive and integrated way. which makes the prevention of stunting more complex. For example, Cambodia is still among countries with a high prevalence of the population without access to adequate sanitation (44%) [
8], which could negatively impact all efforts made towards stunting reduction if WASH interventions are not implemented.
Even if in Cambodia, less than 3% of the 266 million USD in annual economic burden is associated with acute malnutrition requiring in-patient or out-patient clinical life-saving medical care, it is essential to continue the efforts to treat those affected children. Evidence suggests episodes of wasting negatively affect linear growth and, therefore, undermine child growth and development [
37]. During a workshop in 2014, experts agreed that wasting and stunting share many common risk factors and therefore clearer policy directives are needed to encourage and facilitate practical links for more integrated programming [
40].
As highlighted in
Figure 1, the second biggest cause of the economic burden is due to iodine deficiency disorders, and several interventions have been implemented in Cambodia over the last decade. Since the 2003 Government’s Sub-Decree No. 69 on mandatory iodization of salt and several related regulations, Cambodia’s supply of iodized salt has increased greatly to reach approximately 70 per cent of households around 5 years ago [
41]. Unfortunately, to date, the current levels of iodine added to tested salt are unsatisfactory as 92% of those salts do not meet the government’s iodization requirements (99.6% of the coarse salt and 82.4% of the fine salt) [
41]. This inappropriate iodization has a direct causality with the drastic reduction of urinary iodine concentration observed over the last few years [
33]. A minimum investment of 750,000 USD/year in Cambodia (0.05 USD/person/year) could resolve the problem, as already observed during a national assessment of the National program 2011 [
42]. This intervention, coupled with the implementation of an effective regulatory monitoring and enforcement system, should allow sustainable prevention of any iodine deficiency disorder. The other child micronutrient deficiencies (zinc, vitamin A, and iron) could be prevented with the development of a social marketing strategy for micronutrient supplements or food supplements to improve the quality of complementary feeding. Cambodia could use the Scaling Up Nutrition (SUN) initiative, and especially the SUN business network, to ensure that commitment from the private sector to support the national initiative to iodize all salt used at the household level and during the production of processed foods, such as fish or soya sauces, is happening.
As highlighted in the recent global nutrition report [
5], scaling up nutrition-specific interventions to 90% coverage will generate a median benefit–cost ratio of 16:1 in countries like Cambodia. Therefore, investing 40 million USD (15% of the total economic burden of malnutrition in Cambodia) as described in the “Ministry of Health Conceptual budget for Cambodia’s fast track road map for improving nutrition” is recognized to be highly effective [
43].
Limitations to the conceptual model: Converting indicators of malnutrition to an economic activity and attaching a monetary value to that economic activity could be interpreted and analyzed in many different ways. First, monetizing the consequences of malnutrition is dependent on evolving evidence bases, complex methodologies and national health, demographic and economic statistics of uneven quality; Second, many factors beyond individual physical and intellectual potential determine earnings or work performance. Workplace incentives, available technology, and sense of opportunity all affect how increased human potential translates into actual improved productivity. In addition, productivity growth was not considered in the model, even if we can speculate that today’s children are likely to be much more productive in their working life than their parents are today; Finally, benefits of improved nutrition extend beyond the workplace to a range of “voluntary” activities, including parenting and household activities to educational improvement, entrepreneurial pursuits, and community participation. In a world where improvement in nutrition, health, and subsequent productivity will emerge mainly from individual choices and behaviors, the significance of these “voluntary” activities cannot be overstated. For all these reasons and more, the margin of error is large and the calculations should be considered as an order of magnitude. These are projections to focus and facilitate policy discussion and present a solid and conservative case for policy discussion. Therefore, data judgments or assumptions are consciously and consistently “biased” to minimize the impact of malnutrition. Consequently, conclusions drawn may be considered conservative low-end estimates.

 ,
, 


{kind=link}
{kind=link}