Beverage Intake Assessment Questionnaire: Relative Validity and Repeatability in a Spanish Population with Metabolic Syndrome from the PREDIMED-PLUS Study

 , , , , and
, , , , and 
Abstract
:
1. Introduction
2. Material and Methods
2.1. Subjects and Design
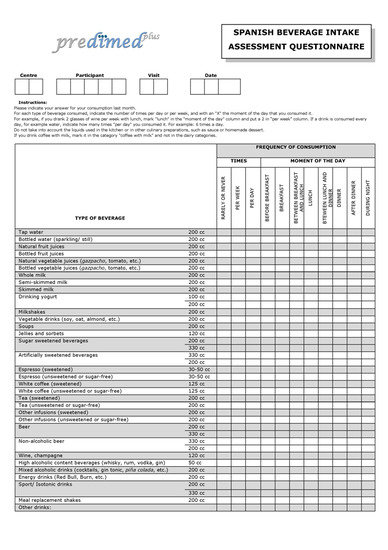
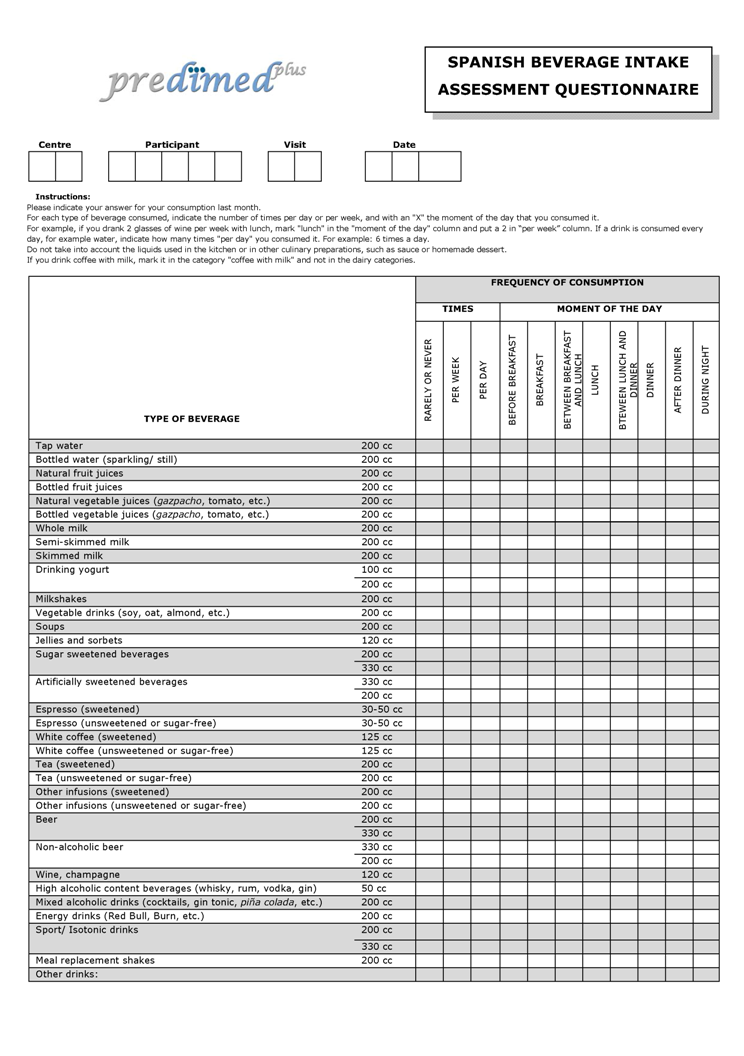
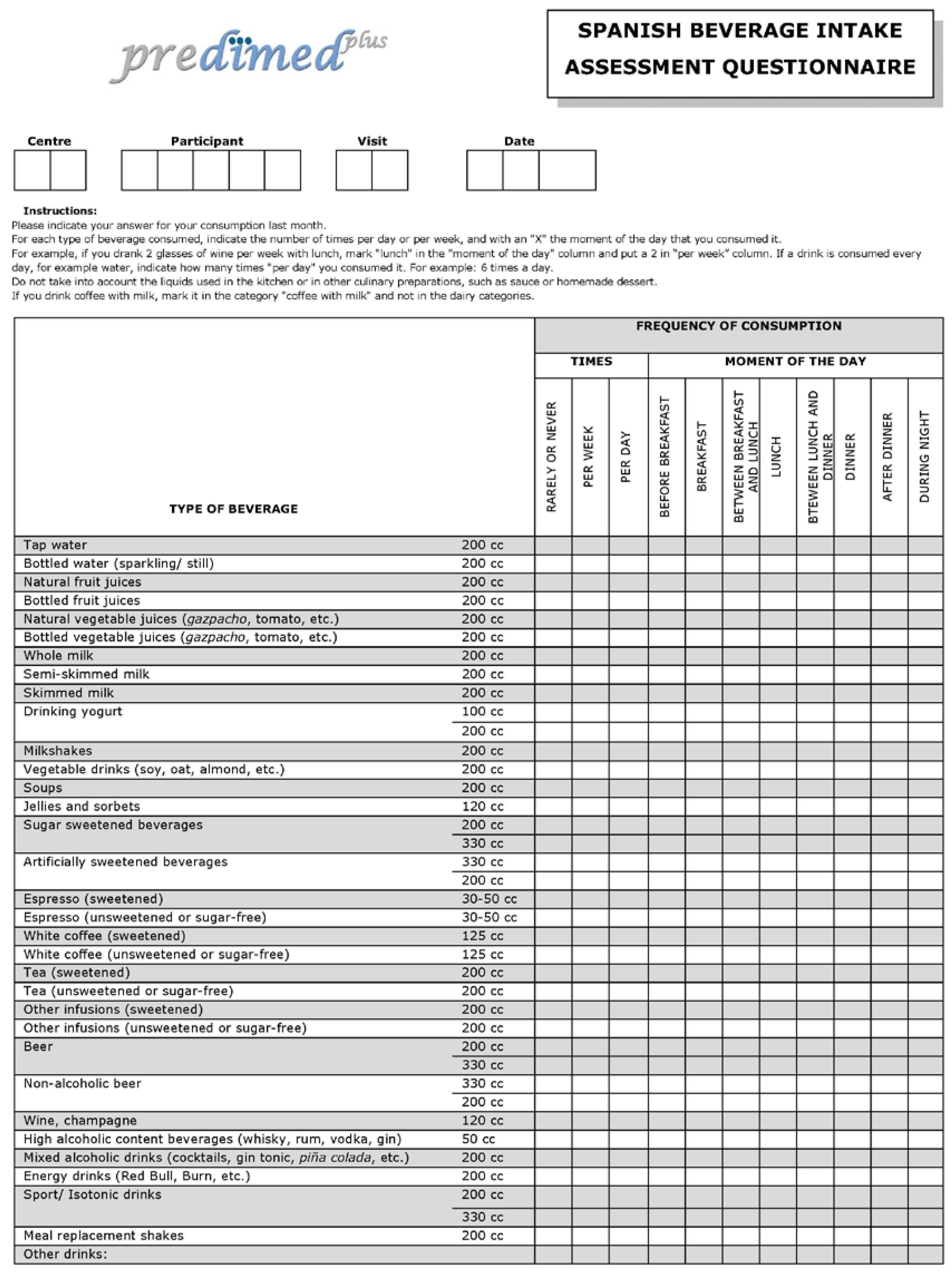
2.2. Assessment of Fluid Intake
2.3. Urine Collection
2.4. Assessment of Other Covariates
2.5. Statistical Analysis
3. Results
3.1. Relative Validity of the Questionnaire
3.2. Repeatability of the Questionnaire
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
Abbreviations
References
- Johnson, E.C.; Muñoz, C.X.; Le Bellego, L.; Klein, A.; Casa, D.J.; Maresh, C.M.; Armstrong, L.E. Markers of the hydration process during fluid volume modification in women with habitual high or low daily fluid intakes. Eur. J. Appl. Physiol. 2015, 115, 1067–1074. [Google Scholar] [CrossRef] [PubMed]
- Lafontan, M. H4H—Hydration for health. Obes. Facts 2014, 7 (Suppl. S2), 1–5. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Popkin, B.M.; Bray, G.A.; Despres, J.-P.; Willett, W.C.; Hu, F.B. Sugar-Sweetened Beverages and Risk of Metabolic Syndrome and Type 2 Diabetes: A meta-analysis. Diabetes Care 2010, 33, 2477–2483. [Google Scholar] [CrossRef] [PubMed]
- Cohen, L.; Curhan, G.; Forman, J. Association of sweetened beverage intake with incident hypertension. J. Gen. Intern. Med. 2012, 27, 1127–1134. [Google Scholar] [CrossRef] [PubMed]
- Sonestedt, E. Artificial and sugar-sweetened beverages are associated with increased incidence of hypertension. Evid.-Based Med. 2013, 18, e38. [Google Scholar] [CrossRef] [PubMed]
- Sayon-Orea, C.; Martinez-Gonzalez, M.A.; Gea, A.; Alonso, A.; Pimenta, A.M.; Bes-Rastrollo, M. Baseline consumption and changes in sugar-sweetened beverage consumption and the incidence of hypertension: The SUN project. Clin. Nutr. 2014, 34, 1133–1140. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Hu, F.B. Fructose and Cardiometabolic Health: What the Evidence from Sugar-Sweetened Beverages Tells Us. J. Am. Coll. Cardiol. 2015, 66, 1615–1624. [Google Scholar] [CrossRef] [PubMed]
- Sauvant, M.P.; Pepin, D. Drinking water and cardiovascular disease. Food Chem. Toxicol. 2002, 40, 1311–1325. [Google Scholar] [CrossRef]
- Khosravi-Boroujeni, H.; Sarrafzadegan, N.; Mohammadifard, N.; Alikhasi, H.; Sajjadi, F.; Asgari, S.; Esmaillzadeh, A. Consumption of sugar-sweetened beverages in relation to the metabolic syndrome among Iranian adults. Obes. Facts 2012, 5, 527–537. [Google Scholar] [CrossRef] [PubMed]
- Odegaard, A.O.; Koh, W.-P.; Yuan, J.-M.; Pereira, M.A. Beverage habits and mortality in Chinese adults. J. Nutr. 2015, 145, 595–604. [Google Scholar] [CrossRef] [PubMed]
- Rippe, J.M. The Metabolic and Endocrine Response and Health Implications of Consuming Sugar-Sweetened Beverages: Findings from Recent Randomized Controlled Trials. Adv. Nutr. 2013, 4, 677–686. [Google Scholar] [CrossRef] [PubMed]
- Armstrong, L.E. Challenges of linking chronic dehydration and fluid consumption to health outcomes. Nutr. Rev. 2012, 70 (Suppl. S2), S121–S127. [Google Scholar] [CrossRef] [PubMed]
- Popkin, B.B.M.; D’Anci, K.K.E.; Rosenberg, I.I.H. Water, hydration, and health. Nutr. Rev. 2010, 68, 439–458. [Google Scholar] [CrossRef] [PubMed]
- Manz, F.; Johner, S.A.; Wentz, A.; Boeing, H.; Remer, T. Water balance throughout the adult life span in a German population. Br. J. Nutr. 2012, 107, 1673–1681. [Google Scholar] [CrossRef] [PubMed]
- Riebl, S.K.; MacDougal, C.; Hill, C.; Estabrooks, P.A.; Dunsmore, J.C.; Savla, J.; Frisard, M.I.; Dietrich, A.M.; Davy, B.M. Beverage Choices of Adolescents and Their Parents Using the Theory of Planned Behavior: A Mixed Methods Analysis. J. Acad. Nutr. Diet. 2016, 116, 226–239. [Google Scholar] [CrossRef] [PubMed]
- Serra-Majem, L.; Santana-Armas, J.F.; Ribas, L.; Salmona, E.; Ramon, J.M.; Colom, J.; Salleras, L. A comparison of five questionnaires to assess alcohol consumption in a Mediterranean population. Public Health Nutr. 2002, 5, 589–594. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, V.E.; Savla, J.; Comber, D.L.; Flack, K.D.; Estabrooks, P.A.; Nsiah-Kumi, P.A.; Ortmeier, S.; Davy, B.M. Development of a brief questionnaire to assess habitual beverage intake (BEVQ-15): Sugar-Sweetened beverages and total beverage energy intake. J. Acad. Nutr. Diet. 2012, 112, 840–849. [Google Scholar] [CrossRef] [PubMed]
- Le Bellego, L.; Jean, C.; Jiménez, L.; Magnani, C.; Tang, W.; Boutrolle, I. Understanding Fluid Consumption Patterns to Improve Healthy Hydration. Nutr. Today 2010, 45, S22–S26. [Google Scholar] [CrossRef]
- Popkin, B.B.M.; Armstrong, L.L.E.; Bray, G.M.; Caballero, B.; Frei, B.; Willett, W.C. A new proposed guidance system for beverage consumption in the United States. Am. J. Clin. Nutr. 2006, 83, 529–542. [Google Scholar] [PubMed]
- Han, E.; Powell, L.M. Consumption patterns of sugar-sweetened beverages in the United States. J. Acad. Nutr. Diet. 2013, 113, 43–53. [Google Scholar] [CrossRef] [PubMed]
- Hedrick, V.E.; Comber, D.L.; Estabrooks, P.A.; Savla, J.; Davy, B.M. The beverage intake questionnaire: Determining initial validity and reliability. J. Am. Diet. Assoc. 2010, 110, 1227–1232. [Google Scholar] [CrossRef] [PubMed]
- PREDIMED-PLUS. Available online: http://predimedplus.com/ (accessed on 8 June 2016).
- Alberti, K.G.M.M.; Eckel, R.H.; Grundy, S.M.; Zimmet, P.Z.; Cleeman, J.I.; Donato, K.A.; Fruchart, J.-C.; James, W.P.T.; Loria, C.M.; Smith, S.C. Harmonizing the metabolic syndrome: a joint interim statement of the International Diabetes Federation Task Force on Epidemiology and Prevention; National Heart, Lung, and Blood Institute; American Heart Association; World Heart Federation; International Atherosclerosis Society; and International Association for the Study of Obesity. Circulation 2009, 120, 1640–1645. [Google Scholar] [PubMed]
- United States Department of Agriculture USD. A Online Database. Available online: https://ndb.nal.usda.gov/ (accessed on 8 June 2016).
- Manz, F.; Wentz, A.; Sichert-Hellert, W. The most essential nutrient: defining the adequate intake of water. J. Pediatr. 2002, 141, 587–592. [Google Scholar] [CrossRef] [PubMed]
- Elosua, R.; Marrugat, J.; Molina, L.; Pons, S.; Pujol, E. Validation of the Minnesota Leisure Time Physical Activity Questionnaire in Spanish men. The MARATHOM Investigators. Am. J. Epidemiol. 1994, 139, 1197–1209. [Google Scholar] [PubMed]
- Fernández-Ballart, J.D.; Piñol, J.L.; Zazpe, I.; Corella, D.; Carrasco, P.; Toledo, E.; Perez-Bauer, M.; Martínez-González, M.A.; Salas-Salvadó, J.; Martín-Moreno, J.M. Relative validity of a semi-quantitative food-frequency questionnaire in an elderly Mediterranean population of Spain. Br. J. Nutr. 2010, 103, 1808–1816. [Google Scholar] [CrossRef] [PubMed]
- Mataix, V. Tabla de Composición de Alimentos [Food Composition Table], 4th ed.; Universidad de Granada: Granada, Spain, 2003. (In Spanish) [Google Scholar]
- Moreiras, O.; Cabrera, L. Tabla de Composición de Alimentos [Food Composition Table]; Ediciones Pirámide: Madrid, Spain, 2005. [Google Scholar]
- Schröder, H.; Fitó, M.; Estruch, R.; Martínez-González, M.A.; Corella, D.; Salas-Salvadó, J.; Lamuela-Raventós, R.; Ros, E.; Salaverría, I.; Fiol, M.; et al. A short screener is valid for assessing Mediterranean diet adherence among older Spanish men and women. J. Nutr. 2011, 141, 1140–1145. [Google Scholar] [CrossRef] [PubMed]
- Neuhouser, M.L.; Lilley, S.; Lund, A.; Johnson, D.B. Development and validation of a beverage and snack questionnaire for use in evaluation of school nutrition policies. J. Am. Diet. Assoc. 2009, 109, 1587–1592. [Google Scholar] [CrossRef] [PubMed]
- Malisova, O.; Bountziouka, V.; Panagiotakos, D.B.; Zampelas, A.; Kapsokefalou, M. The water balance questionnaire: Design, reliability and validity of a questionnaire to evaluate water balance in the general population. Int. J. Food Sci. Nutr. 2012, 63, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Nissensohn, M.; Ruano, C.; Serra-Majem, L. Validation of beverage intake methods vs. hydration biomarker; a short review. Nutr. Hosp. 2013, 28, 1815–1819. [Google Scholar] [PubMed]
- Armstrong, L.E. Assessing hydration status: the elusive gold standard. J. Am. Coll. Nutr. 2007, 26, 575S–584S. [Google Scholar] [CrossRef] [PubMed]
- Shirreffs, S.M. Markers of hydration status. Eur. J. Clin. Nutr. 2003, 57 (Suppl. S2), S6–S9. [Google Scholar] [CrossRef] [PubMed]
- Tsubono, Y.; Nishino, Y.; Fukao, A.; Hisamichi, S.; Tsugane, S. Temporal change in the reproducibility of a self-administered food frequency questionnaire. Am. J. Epidemiol. 1995, 142, 1231–1235. [Google Scholar] [PubMed]
- Cade, J.; Thompson, R.; Burley, V.; Warm, D. Development, validation and utilisation of food-frequency questionnaires—A review. Public Health Nutr. 2002, 5, 567–587. [Google Scholar] [CrossRef] [PubMed]
- Willett, W.; Lenart, E. Nutritional Epidemiology, 2nd ed.; Oxford University Press: New York, NY, USA, 1998. [Google Scholar]
- Ferreira-pêgo, C.; Babio, N.; Fenández-alvira, J.M.; Iglesia, I.; Moreno, L.A. Fluid intake from beverages in Spanish adults: Cross-Sectional study. Nutr. Hosp. 2014, 29, 1171–1178. [Google Scholar] [PubMed]
- Saetun, P.; Semangoen, T.; Thongboonkerd, V. Characterizations of urinary sediments precipitated after freezing and their effects on urinary protein and chemical analyses. Am. J. Physiol. Ren. Physiol. 2009, 296, F1346–F1354. [Google Scholar] [CrossRef] [PubMed]
- Cheuvront, S.N.; Ely, B.R.; Kenefick, R.W.; Sawka, M.N. Biological variation and diagnostic accuracy of dehydration assessment markers. Am. J. Clin. Nutr. 2010, 92, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Sparks, S.A.; Close, G.L. Validity of a portable urine refractometer: The effects of sample freezing. J. Sports Sci. 2013, 31, 745–749. [Google Scholar] [CrossRef] [PubMed]
- Remer, T.; Montenegro-Bethancourt, G.; Shi, L. Long-Term urine biobanking: Storage stability of clinical chemical parameters under moderate freezing conditions without use of preservatives. Clin. Biochem. 2014, 47, 307–311. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Variables | All Population (n = 160) | Men (n = 68) | Women (n = 92) | p-Value a |
|---|---|---|---|---|
| Age, years | 65.3 (4.9) | 64.5 (5.9) | 65.9 (3.9) | 0.097 |
| Height, m | 1.62 (0.09) | 1.69 (0.06) | 1.56 (0.06) | <0.001 |
| Weight, kg | 86.7 (14.3) | 94.3 (12.5) | 81.9 (12.9) | <0.001 |
| BMI, kg/m2 | 33.0 (4.3) | 32.9 (3.6) | 33.1 (4.7) | 0.328 |
| Leisure-time physical activity, METs/week | 3123 (2804) | 4006 (2945) | 2471 (2518) | <0.001 |
| Mediterranean diet score, (0–17 points) | 9.2 (2.5) | 8.5 (2.6) | 9.8 (2.3) | <0.005 |
| Total energy intake, kcal/day | 2229 (551) | 2330 (606) | 2155 (497) | <0.005 |
| Total protein intake, g/day | 134 (357) | 189 (545) | 93 (22) | 0.276 |
| Urine volume, mL/day | 1722 (651) | 1762 (698) | 1693 (616) | 0.506 |
| Urine osmolality, mOsm/kg | 551 (211) | 631 (204) | 492 (196) | <0.001 |
| Urine albumin, mg/dL | 13.8 (31.8) | 20.0 (39.5) | 9.0 (23.4) | 0.047 |
| Urine creatinine, μmol/dL | 7718 (3760) | 9440 (4204) | 6431 (2783) | <0.001 |
| Urine albumin to creatinine ratio, mg/g | 17.1 (43.4) | 22.2 (53.2) | 13.2 (33.9) | 0.228 |
| Use of medications, % (n) | ||||
| Aspirin | 24.4 (39) | 26.5 (18) | 22.8 (21) | 0.596 |
| Pain relief | 33.7 (54) | 17.6 (12) | 45.6 (42) | <0.005 |
| Tranquilizers | 27.5 (44) | 17.6 (12) | 34.8 (32) | 0.016 |
| Vitamin/minerals | 6.9 (11) | 2.9 (2) | 9.8 (9) | 0.091 |
| Heart problems | 4.4 (7) | 5.9 (4) | 3.3 (3) | 0.423 |
| Antihypertensive agents | 79.4 (127) | 82.3 (56) | 77.2 (71) | 0.423 |
| Statins | 56.9 (91) | 50.0 (34) | 62.0 (57) | 0.131 |
| Insulin | 6.2 (10) | 5.9 (4) | 6.5 (6) | 0.869 |
| Oral anti-diabetic drugs | 30.0 (48) | 30.9 (21) | 29.3 (27) | 0.834 |
| Others | 68.1 (109) | 63.2 (43) | 71.7 (66) | 0.254 |
| Term | Parameter Estimate | Standardized β * | Standard Error | p-Value | R2 |
|---|---|---|---|---|---|
| Intercept | 2278 | ||||
| Osmolality | −0.65 | −0.26 | 0.18 | 0.0005 | 0.20 |
| Age | −25.13 | −0.23 | 7.94 | 0.0019 | |
| BMI | 23.86 | 0.15 | 11.38 | 0.0376 | |
| Total energy | 0.27 | 0.25 | 0.08 | 0.0007 | |
| Intercept | 2455 | ||||
| Urine volume | 0.22 | 0.27 | 0.06 | 0.0003 | 0.20 |
| Age | −26.03 | −0.24 | 7.93 | 0.0013 | |
| Total energy | 0.24 | 0.23 | 0.07 | 0.0019 |
| Beverage Category | Baseline (mL/day) (n = 67) | Baseline vs. 6 Months | Baseline vs. 1 Year | |||||
|---|---|---|---|---|---|---|---|---|
| Mean (SD) | Mean (SD) | |||||||
| 6 Months (mL/day) (n = 45) | Differences from Baseline | p-Value a | 1 Year (mL/day) (n = 34) | Differences from Baseline | p-Value a | p-Value b | ||
| Tap water | 289 (571) | 449 (657) | 62 (413) | 0.32 | 360 (577) | −23 (502) | 0.79 | 0.389 |
| Bottled water | 755 (539) | 773 (714) | 80 (505) | 0.29 | 813 (612) | 125 (577) | 0.22 | 0.905 |
| Natural fruit juices | 39 (69) | 27 (54) | 1 (79) | 0.92 | 28 (61) | 16 (75) | 0.21 | 0.537 |
| Bottled fruit juices | 26 (93) | 22 (52) | 7 (46) | 0.33 | 19 (44) | 7 (29) | 0.16 | 0.880 |
| Natural vegetable juices | 6 (28) | 16 (36) | 9 (29) | 0.05 | 1 (9) | −1 (16) | 0.79 | 0.073 |
| Bottled vegetable juices | 14 (69) | 4 (14) | −5 (32) | 0.25 | 4 (18) | −7 (41) | 0.35 | 0.451 |
| Whole milk | 24 (92) | 3 (17) | −16 (89) | 0.22 | 25 (74) | 4 (125) | 0.86 | 0.284 |
| Semi-skimmed milk | 43 (81) | 67 (126) | 8 (125) | 0.67 | 63 (123) | 9 (131) | 0.69 | 0.467 |
| Skimmed milk | 95 (146) | 59 (107) | −19 (145) | 0.38 | 54 (102) | −36 (151) | 0.17 | 0.192 |
| Drinking yogurt (100 cc) | 13 (32) | 10 (32) | −6 (32) | 0.23 | 8 (23) | −6 (25) | 0.18 | 0.765 |
| Drinking yogurt (200 cc) | 6 (31) | 13 (46) | 5 (61) | 0.58 | 10 (42) | 4 (54) | 0.56 | 0.562 |
| Milkshakes | 0 (2) | 0 (0) | 0 (3) | 0.32 | 2 (10) | 1 (11) | 0.53 | 0.289 |
| Vegetable drinks | 21 (80) | 9 (39) | 5 (49) | 0.47 | 38 (128) | 33 (133) | 0.16 | 0.330 |
| Soups | 36 (30) | 34 (35) | 0 (45) | 0.93 | 50 (56) | 17 (52) | 0.07 | 0.144 |
| Jellies and sorbets | 2 (11) | 1 (5) | −1 (9) | 0.61 | 1 (4) | −1 (7) | 0.64 | 0.594 |
| SSBs (200 cc) | 11 (34) | 11 (38) | 3 (31) | 0.53 | 7 (32) | −3 (18) | 0.32 | 0.862 |
| SSBs (330 cc) | 8 (39) | 18 (90) | 6 (92) | 0.68 | 10 (51) | 5 (54) | 0.59 | 0.707 |
| ASBs (200 cc) | 7 (48) | 21 (118) | 11 (134) | 0.57 | 39 (158) | 37 (157) | 0.18 | 0.363 |
| ASBs (330 cc) | 42 (164) | 8 (32) | −54 (200) | 0.08 | 18 (45) | −61 (215) | 0.11 | 0.292 |
| Espresso sweetened | 16 (31) | 9 (20) | −4 (31) | 0.33 | 9 (18) | −4 (20) | 0.25 | 0.287 |
| Espresso unsweetened | 24 (35) | 36 (38) | 7 (36) | 0.22 | 31 (37) | 2 (23) | 0.62 | 0.223 |
| White coffee sweetened | 23 (63) | 5 (25) | −3 (40) | 0.66 | 4 (21) | −2 (36) | 0.69 | 0.063 |
| White coffee unsweetened | 9 (31) | 3 (18) | −5 (35) | 0.32 | 7 (28) | 3 (36) | 0.57 | 0.492 |
| Tea sweetened | 7 (29) | 2 (13) | −7 (26) | 0.09 | 14 (48) | 2 (65) | 0.82 | 0.246 |
| Tea unsweetened | 25 (87) | 34 (105) | 17 (79) | 0.15 | 19 (51) | −2 (54) | 0.82 | 0.718 |
| Other infusions sweetened | 27 (96) | 13 (66) | 12 (67) | 0.23 | 17 (55) | 15 (56) | 0.13 | 0.646 |
| Other infusions unsweetened | 34 (91) | 51 (107) | 14 (90) | 0.30 | 54 (139) | 12 (106) | 0.51 | 0.613 |
| Beer (200 cc) | 18 (67) | 10 (32) | −12 (68) | 0.24 | 1 (4) | −18 (71) | 0.13 | 0.266 |
| Beer (330 cc) | 32 (91) | 47 (119) | 2 (131) | 0.92 | 26 (66) | 6 (69) | 0.63 | 0.580 |
| Non-alcoholic beer (200 cc) | 5 (25) | 11 (39) | −8 (45) | 0.21 | 5 (24) | −4 (20) | 0.28 | 0.581 |
| Non-alcoholic beer (330 cc) | 13 (54) | 3 (14) | 4 (22) | 0.25 | 2 (15) | −11 (58) | 0.25 | 0.283 |
| Wine | 35 (63) | 41 (68) | −7 (60) | 0.46 | 60 (85) | 9 (55) | 0.35 | 0.257 |
| High alcoholic content beverages | 1 (3) | 1 (4) | 0 (3) | 0.66 | 1 (2) | 0 (3) | 0.26 | 0.988 |
| Mixed alcoholic beverages | 1 (6) | 0 (3) | 0 (0) | - | 0 (0) | 0 (3) | 0.32 | 0.388 |
| Energy drinks | 0 (0) | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | - | - |
| Sports drinks (200 cc) | 0 (3) | 0 (0) | 0 (4) | 0.32 | 0 (0) | 0 (0) | - | 0.558 |
| Sports drinks (330 cc) | 0 (0) | 2 (13) | 2 (13) | 0.32 | 0 (0) | 0 (0) | - | 0.328 |
| Meal replacement shakes | 0 (0) | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | - | - |
| Other drinks | 0 (0) | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | - | - |
| Total water intake | 1711 (64) | 1816 (498) | 106 (475) | 0.14 | 1804 (435) | 128 (559) | 0.19 | 0.477 |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC-BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ferreira-Pêgo, C.; Nissensohn, M.; Kavouras, S.A.; Babio, N.; Serra-Majem, L.; Martín Águila, A.; Mauromoustakos, A.; Álvarez Pérez, J.; Salas-Salvadó, J. Beverage Intake Assessment Questionnaire: Relative Validity and Repeatability in a Spanish Population with Metabolic Syndrome from the PREDIMED-PLUS Study. Nutrients 2016, 8, 475. https://doi.org/10.3390/nu8080475
Ferreira-Pêgo C, Nissensohn M, Kavouras SA, Babio N, Serra-Majem L, Martín Águila A, Mauromoustakos A, Álvarez Pérez J, Salas-Salvadó J. Beverage Intake Assessment Questionnaire: Relative Validity and Repeatability in a Spanish Population with Metabolic Syndrome from the PREDIMED-PLUS Study. Nutrients. 2016; 8(8):475. https://doi.org/10.3390/nu8080475
Chicago/Turabian StyleFerreira-Pêgo, Cíntia, Mariela Nissensohn, Stavros A. Kavouras, Nancy Babio, Lluís Serra-Majem, Adys Martín Águila, Andy Mauromoustakos, Jacqueline Álvarez Pérez, and Jordi Salas-Salvadó. 2016. "Beverage Intake Assessment Questionnaire: Relative Validity and Repeatability in a Spanish Population with Metabolic Syndrome from the PREDIMED-PLUS Study" Nutrients 8, no. 8: 475. https://doi.org/10.3390/nu8080475