Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study †

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Food Record and Adequacy of Reported Intake
- 1
- The same dietician-nutritionist was responsible for checking the food records included by the participant during the three-day dietary food record study.
- 2
- The initial quality control was based on the photographs and descriptions sent by the participants, but also in the brief description that was asked before/after each meal and/or intake. Particular care was given to validate some variables such as ingredients, brands of the processed and ready-to-eat foods, portion size or culinary technique to obtain accurate information for further codification.
- 3
- The final approval of the received information was given by a dietician-nutritionist and supervisor.
2.3. Evaluation of Misreporting
2.4. Statistical Analysis
3. Results
3.1. Calcium, Phosphorus, Magnesium and Vitamin D Reported Intake and Distribution in the Whole Population
3.2. Calcium, Phosphorus, Magnesium and Vitamin D Reported Intake in Plausible Reporters
3.3. Disparity between Reported Intake and the Level Needed for Adequacy for Calcium, Magnesium and Vitamin D in the Whole Population
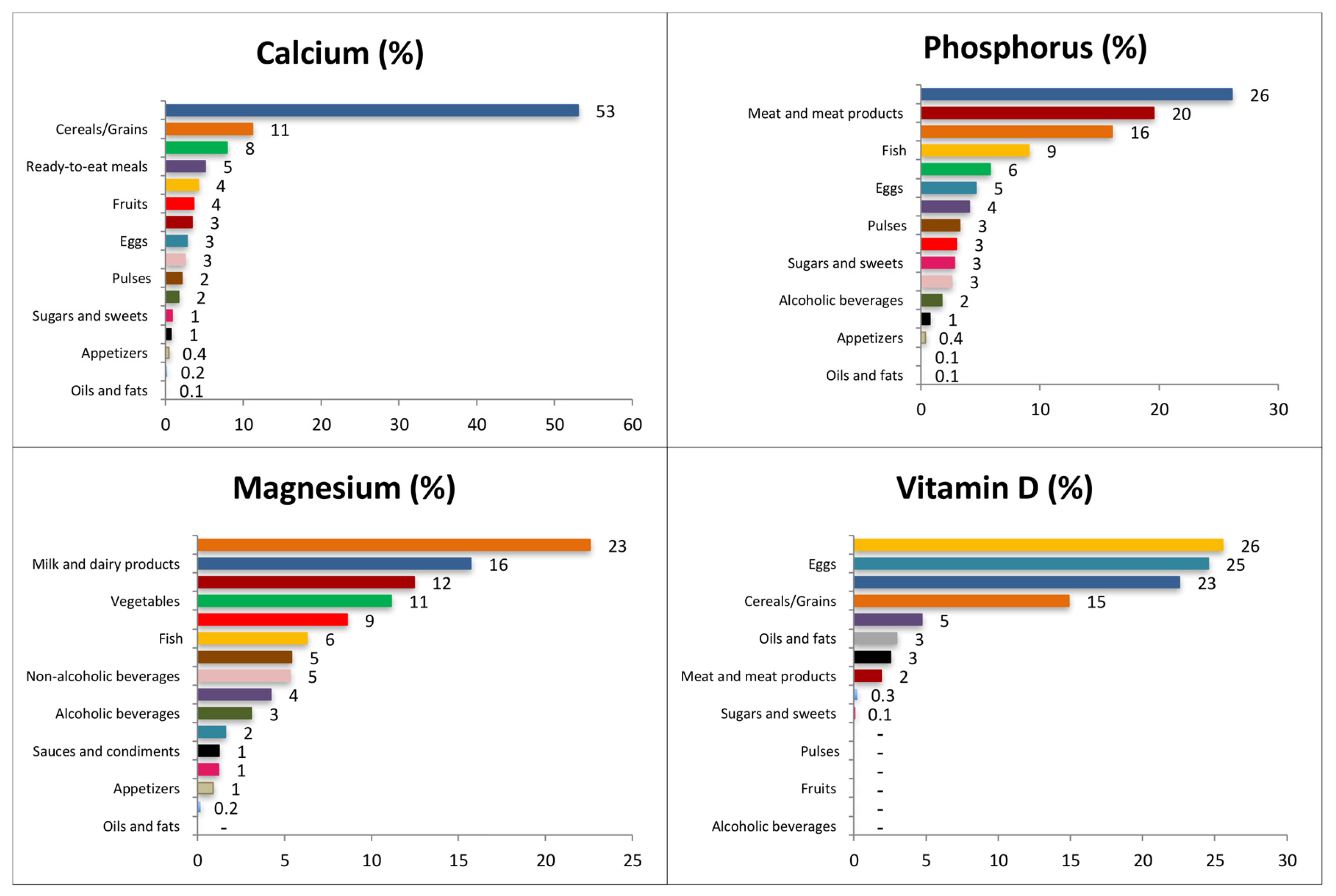
3.4. Contribution of Food Sources to Calcium, Phosphorus, Magnesium and Vitamin D Reported Intakes
3.4.1. Calcium
3.4.2. Phosphorus
3.4.3. Magnesium
3.4.4. Vitamin D
4. Discussion
5. Conclusions
Supplementary Materials
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Dietary Guidelines for Americans 2015–2020, Eight ed. Available online: http://health.gov/dietaryguidelines/2015/guidelines/message/ (accessed on 1 August 2016).
- World Health Organization (WHO). Global Status Report on Noncommunicables Diseases. 2014. Available online: http://apps.who.int/iris/bitstream/10665/148114/1/9789241564854_eng.pdf?ua=1 (accessed on 30 October 2016).
- Ezzati, M.; Riboli, E. Behavioral and Dietary Risk Factors for Noncommunicable Diseases. N. Engl. J. Med. 2013, 369, 954–964. [Google Scholar] [CrossRef] [PubMed]
- Institute of Medicine (IoM). Dietary Reference Intakes for Calcium, Phosphorus, Magnesium, Vitamin D, and Fluoride. Available online: https://www.nap.edu/catalog/5776/dietary-reference-intakes-for-calcium-phosphorus-magnesium-vitamin-d-and-fluoride (accessed on 10 October 2016).
- Rosanoff, A.; Dai, Q.; Shapses, S.A. Essential Nutrient Interactions: Does Low or Suboptimal Magnesium Status Interact with Vitamin D and/or Calcium Status? Adv. Nutr. 2016, 7, 25–43. [Google Scholar] [CrossRef] [PubMed]
- Muscogiuri, G.; Altieri, B.; Annweiler, C.; Balercia, G.; Pal, H.B.; Boucher, B.; Cannell, J.J.; Foresta, C.; Grübler, M.R.; Kotsa, K.; et al. Vitamin D and chronic diseases: The current state of the art. Arch. Toxicol. 2016. [Google Scholar] [CrossRef] [PubMed]
- Beto, J.A. The role of calcium in human aging. Clin. Nutr. Res. 2015, 4, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Soedamah-Muthu, S.S.; Verberne, L.D.; Ding, E.L.; Engberink, M.F.; Geleijnse, J.M. Dairy consumption and incidence of hypertension a dose-response meta-analysis of prospective cohort studies. Hypertension 2012, 60, 1131–1137. [Google Scholar] [CrossRef] [PubMed]
- Louie, J.C.; Flood, V.M.; Rangan, A.M.; Burlutsky, G.; Gill, T.P.; Gopinath, B.; Mitchell, P. Higher regular fat dairy consumption is associated with lower incidence of metabolic syndrome but not type 2 diabetes. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 816–821. [Google Scholar] [CrossRef] [PubMed]
- Malik, V.S.; Sun, Q.; van Dam, R.M.; Rimm, E.B.; Willett, W.C.; Rosner, B.; Hu, F.B. Adolescent dairy product consumption and risk of type 2 diabetes in middle-aged women. Am. J. Clin. Nutr. 2011, 94, 854–861. [Google Scholar] [CrossRef] [PubMed]
- Fumeron, F.; Lamri, A.; Abi Khalil, C.; Jaziri, R.; Porchay-Balderelli, I.; Lantieri, O.; Vol, S.; Balkau, B.; Marre, M. Dairy consumption and the incidence of hyperglycemia and the metabolic syndrome: Results from a French prospective study, data from the Epidemiological Study on the Insulin Resistance Syndrome (DESIR). Diabetes Care 2011, 34, 813–817. [Google Scholar] [CrossRef] [PubMed]
- Margolis, K.L.; Wei, F.; de Boer, I.H.; Howard, B.V.; Liu, S.; Manson, J.E.; Mossavar-Rahmani, Y.; Phillips, L.S.; Shikany, J.M.; Tinker, L.F. A diet high in low-fat dairy products lowers diabetes risk in postmenopausal women. J. Nutr. 2011, 141, 1969–1974. [Google Scholar] [CrossRef] [PubMed]
- Struijk, E.A.; Heraclides, A.; Witte, D.R.; Soedamah-Muthu, S.S.; Geleijnse, J.M.; Toft, U.; Lau, C.J. Dairy product intake in relation to glucose regulation indices and risk of type 2 diabetes. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 822–828. [Google Scholar] [CrossRef] [PubMed]
- Ortega, R.M.; Jiménez, A.I.; López-Sabater, A.M. El calcio y la salud. Nutr. Hosp. 2015, 31 (Suppl. 2), 10–17. (In Spanish) [Google Scholar]
- Gutierrez, O.M. The connection between dietary phosphorus, cardiovascular disease, and mortality: Where we stand and what we need to know. Adv. Nutr. 2013, 4, 723–729. [Google Scholar] [CrossRef] [PubMed]
- Ayuk, J.; Gittoes, N.J. Contemporary view of the clinical relevance of magnesium homeostasis. Ann. Clin. Biochem. 2014, 51, 179–188. [Google Scholar] [CrossRef] [PubMed]
- Gröber, U.; Schmidt, J.; Kisters, K. Magnesium in Prevention and Therapy. Nutrients 2015, 7, 8199–8226. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Dietary reference values for vitamin D, EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). EFSA J. 2016, 14, 4547. [Google Scholar]
- Fuleihan, G.-H.; Bouillon, R.; Clarke, B.; Chakhtoura, M.; Cooper, C.; McClung, M.; Singh, R.J. Serum 25-Hydroxyvitamin D Levels: Variability, Knowledge Gaps, and the Concept of a Desirable Range. J. Bone Miner. Res. 2015, 30, 1119–1133. [Google Scholar] [CrossRef] [PubMed]
- Glendenning, P.; Inderjeeth, C. Controversy and consensus regarding vitamin D: Recent methodological changes and the risks and benefits of vitamin D supplementation. Crit. Rev. Clin. Lab. Sci. 2016, 53, 13–28. [Google Scholar] [CrossRef] [PubMed]
- Archer, E.; Hand, G.A.; Blair, S.N. Validity of U.S. nutritional surveillance: National Health and Nutrition Examination Survey caloric energy intake data, 1971–2010. PLoS ONE 2013, 8, e76632. [Google Scholar] [CrossRef]
- European Food Safety Authority (EFSA). Example of a Protocol for Identification of Misreporting (Under- and Over-Reporting of Energy Intake) Based on the PILOT-PANEU Project. Available online: http://www.efsa.europa.eu/sites/default/files/efsa_rep/blobserver_assets/3944A-8–2-1.pdf (accessed on 10 February 2016).
- Archer, E.; Pavela, G.; Lavie, C.J. The Inadmissibility of What We Eat in America and NHANES Dietary Data in Nutrition and Obesity Research and the Scientific Formulation of National Dietary Guidelines. Mayo Clin. Proc. 2015, 90, 911–926. [Google Scholar] [CrossRef] [PubMed]
- Archer, E.; Pavela, G.; Lavie, C.J. A Discussion of the Refutation of Memory-Based Dietary Assessment Methods (M-BMs): The Rhetorical Defense of Pseudoscientific and Inadmissible Evidence. Mayo Clin. Proc. 2015, 90, 1736–1739. [Google Scholar] [CrossRef] [PubMed]
- Dhurandhar, N.V.; Schoeller, D.; Brown, A.W.; Heymsfield, S.B.; Thomas, D.; Sorensen, T.I.; Speakman, J.R.; Jeansonne, M.; Allison, D.B. Energy Balance Measurement Working Group. Energy balance measurement: When something is not better than nothing. Int. J. Obes. (Lond.) 2014, 39, 1109–1113. [Google Scholar] [CrossRef] [PubMed]
- Araujo, M.C.; Bezerra, I.N.; Barbosa Fdos, S.; Junger, W.L.; Yokoo, E.M.; Sichieri, R. Macro-nutrient consumption and inadequate micronutrient intake in adults. Rev. Saude Publica 2013, 47 (Suppl. 1), 177S–189S. [Google Scholar] [CrossRef] [PubMed]
- Tooze, J.A.; Midthune, D.; Dodd, K.W.; Freedman, L.S.; Krebs-Smith, S.M.; Subar, A.F.; Guenther, P.M.; Carroll, R.J.; Kipnis, V. A new statistical method for estimating the usual intake of episodically consumed foods with application to their distribution. J. Am. Diet. Assoc. 2006, 106, 1575–1587. [Google Scholar] [CrossRef] [PubMed]
- Barbosa Fdos, S.; Sichieri, R.; Junger, W.L. Assessing usual dietary intake in complex sample design surveys: The National Dietary Survey. Rev. Saude Publica 2013, 47 (Suppl. 1), 171S–176S. [Google Scholar] [CrossRef] [PubMed]
- European Food Safety Authority (EFSA). Guidance on the EU Menu methodology. EFSA J. 2014, 12, 3944. [Google Scholar]
- Ruiz, E.; Ávila, J.M.; Castillo, A.; Valero, T.; del Pozo, S.; Rodriguez, P.; Aranceta Bartrina, J.; Gil, A.; González-Gross, M.; Ortega, R.M.; et al. The ANIBES Study on Energy Balance in Spain: Design, Protocol and Methodology. Nutrients 2015, 7, 970–998. [Google Scholar] [CrossRef] [PubMed]
- Varela Moreiras, G.; Ávila, J.M.; Ruiz, E. Energy Balance, a new paradigm and methodological issues: The ANIBES study in Spain. Nutr. Hosp. 2015, 31, 101–112. [Google Scholar] [PubMed]
- Ruiz, E.; Ávila, J.M.; del Pozo, S.; Rodriguez, P.; Aranceta Bartrina, J.; Gil, A.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G. Macronutrient Distribution and Dietary Sources in the Spanish Population: Findings from the ANIBES Study. Nutrients 2016, 8, 177. [Google Scholar] [CrossRef] [PubMed]
- Nissensohn, M.; Sánchez-Villegas, A.; Ortega, R.M.; Aranceta-Bartrina, J.; Gil, Á.; González-Gross, M.; Varela-Moreiras, G.; Serra-Majem, L. Beverage Consumption Habits and Association with Total Water and Energy Intakes in the Spanish Population: Findings of the ANIBES Study. Nutrients 2016, 8, 232. [Google Scholar] [CrossRef] [PubMed]
- Moreiras, O.; Carbajal, A.; Cabrera, L.; Cuadrado, C. Tablas de Composición de Alimentos/Guía de Prácticas, 16th ed.; Ediciones Pirámide: Madrid, Spain, 2013. (In Spanish) [Google Scholar]
- Carbajal Azcona, Á. Ingestas recomendadas de energía y nutrientes. In Nutrición y Dietética; (revisited 2013); García-Arias, M.T., García-Fernández, M.C., Eds.; Secretariado de Publicaciones y Medios Audiovisuales, Universidad de León: León, Spain, 2003; pp. 1–26. Available online: https://www.ucm.es/data/cont/docs/458-2013-07-24-CARBAJAL-IR-2003-ISBN-84-9773-023–2-rev2013.pdf (accessed on 15 October 2016).
- EFSA. Dietary Reference Values and Dietary Guidelines. Available online: https://www.efsa.europa.eu/en/topics/topic/drv (accessed on 13 September 2016).
- Goldberg, G.R.; Black, A.E.; Jebb, S.A.; Cole, T.J.; Murgatroyd, P.R.; Coward, W.A.; Prentice, A.M. Critical evaluation of energy intake data using fundamental principles of energy physiology: 1. Derivation of cut-off limits to identify underrecording. Eur. J. Clin. Nut. 1991, 45, 569–581. [Google Scholar]
- Black, A.E. Critical evaluation of energy intake using the Goldberg cut-off for energy intake:basal metabolic rate. A practical guide to its calculation, use and limitations. Int. J. Obes. Relat. Metab. Disord. 2000, 24, 1119–1130. [Google Scholar] [CrossRef] [PubMed]
- Black, A.E. The sensitivity and specificity of the Goldberg cut-off for EI:BMR for identifying diet reports of poor validity. Eur. J. Clin. Nutr. 2000, 54, 395–404. [Google Scholar] [CrossRef] [PubMed]
- Schöfield, W.N. Predicting basal metabolic rate, new standards and review of previous work. Hum. Nutr. Clin. Nutr. 1985, 39 (Suppl. 1), 5–41. [Google Scholar] [PubMed]
- Mielgo-Ayuso, J.; Aparicio-Ugarriza, R.; Castillo, A.; Ruiz, E.; Ávila, J.M.; Aranceta Bartrina, J.; Gil, A.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; et al. Physical Activity Patterns of the Spanish Population Are Mostly Determined by Sex and Age: Findings in the ANIBES Study. PLoS ONE 2016, 11, e0149969. [Google Scholar] [CrossRef] [PubMed]
- Rayssiguier, Y.; Libako, P.; Nowacki, W.; Rock, E. Magnesium deficiency and metabolic syndrome: Stress and inflammation may reflect calcium activation. Magnes. Res. 2010, 23, 73–80. [Google Scholar] [PubMed]
- Archer, E.; Blair, S.N. Reply to LS Freedman et al. Adv. Nutr. 2015, 6, 489–490. [Google Scholar] [CrossRef] [PubMed]
- Agencia Española de Seguridad Alimentaria y Nutrición (AESAN). Evaluación Nutricional de la Dieta Española II. Micronutrientes. Sobre Datos de la Encuesta Nacional de Ingesta Dietética (ENIDE); Agencia Española de Seguridad Alimentaria y Nutrición (AESAN): Madrid, Spain, 2011. (In Spanish) [Google Scholar]
- Max Rubner-Institut. Nationale Verzehrsstudie II. Ergebnisbericht Teil 2. Die bundesweite Befragung zur Ernährung von Jugendlichen und Erwachsenen; Max Rubner-Institut: Karlsruhe, Germany, 2008. Chapter 5. (In German) [Google Scholar]
- Hulshof, K.F.A.M.; Ocke, M.C.; van Rossum, C.T.M.; Buurma-Rethans, E.J.M.; Brants, H.A.M.; Drijvers, J.J.M.M.; ter Doest, D. Resultaten van de Voedselconsumptiepeiling 2003. Results of the National Food Consumption Survey 2003; RIVM Report 350030002; RIVM: Bilthoven, The Netherlands, 2004; Available online: http://www.rivm.nl/bibliotheek/rapporten/350030002.html (accessed on 17 October 2016).
- Peltonen, M.; Harald, K.; Männistö, S.; Saarikoski, L.; Peltomäki, P.; Lund, L.; Sundvall, J.; Juolevi, A.; Laatikainen, T.; Aldén-Nieminen, H.; et al. The National FINRISK 2007 Study; B34/2008; National Public Health Institute: Helsinki, Finland, 2008.
- Elmadfa, I.; Meyer, A.; Nowak, V.; Hasenegger, V.; Putz, P.; Verstraeten, R.; Remaut-DeWinter, A.M.; Kolsteren, P.; Dostálová, J.; Dlouhý, P.; et al. European Nutrition and Health Report 2009. Ann. Nutr. Metab. 2009, 55, 1–40. [Google Scholar] [PubMed]
- Turrini, A.; Saba, A.; Perrone, D.; Cialfa, E.; D’Amicis, A. Food consumption patterns in Italy: The INNCA Study 1994–1996. Eur. J. Clin. Nutr. 2001, 55, 571–588. [Google Scholar] [CrossRef] [PubMed]
- Henderson, L.; Irving, K.; Gregory, J.; Bates, C.J.; Prentice, A.; Swan, G.; Farron, M. The National Diet and Nutrition Survey: Adults Aged 19 to 64 Year. Volume 3: Vitamin and Mineral Intake and Urinary Analyses; The Stationery Office: London, UK, 2003. [Google Scholar]
- Roman Viñas, B.; Ribas Barba, L.; Ngo, J.; Gurinovic, M.; Novakovic, R.; Cavelaars, A.; de Groot, L.C.; van’t Veer, P.; Matthys, C.; Serra Majem, L. Projected prevalence of inadequate nutrient intakes in Europe. Ann. Nutr. Metab. 2011, 59, 84–95. [Google Scholar] [CrossRef] [PubMed]
- Mensink, G.B.; Fletcher, R.; Gurinovic, M.; Huybrechts, I.; Lafay, L.; Serra-Majem, L.; Szponar, L.; Tetens, I.; Verkaik-Kloosterman, J.; Baka, A.; et al. Mapping low intake of micronutrients across Europe. Br. J. Nutr. 2013, 110, 755–773. [Google Scholar] [CrossRef] [PubMed]
- Welch, A.A.; Fransen, H.; Jenab, M.; Boutron-Ruault, M.C.; Tumino, R.; Agnoli, C.; Ericson, U.; Johansson, I.; Ferrari, P.; Engeset, D.; et al. Variation in intakes of calcium, phosphorus, magnesium, iron and potassium in 10 countries in the European Prospective Investigation into Cancer and Nutrition study. Eur. J. Clin. Nutr. 2009, 63 (Suppl. 4), S101–S121. [Google Scholar] [CrossRef] [PubMed]
- Calvo, M.S.; Tucker, K.L. Is phosphorus intake that exceeds dietary requirements a risk factor in bone health? Ann. N. Y. Acad. Sci. 2013, 1301, 29–35. [Google Scholar] [CrossRef] [PubMed]
- Helldán, A.; Raulio, S.; Kosola, M.; Tapanainen, H.; Ovaskainen, M.L.; Virtanen, S. Finravinto 2012—Tutkimus; The National FINDIET 2012 Survey; THL Raportti 16/2013; Juvenes Print: Tampere, Finland, 2013; p. 217. (In Finnish) [Google Scholar]
- Amcoff, E.; Edberg, A.; Enghardt Barbieri, H.; Lindroos, A.; Nälsén, C.; Pearson, M.; Warensjö Lemming, E. Riksmatenvuxna 2010–11. Livsmedelsoch Näringsintag Bland Vuxna i Sverige. Resultat från Matvaneundersökning Utförd 2010–11; Livsmedelsverket: Uppsala, Sweden, 2012; p. 180. (In Swedish) [Google Scholar]
- Van Rossum, C.T.M.; Fransen, H.P.; Verkaik-Kloosterman, J.; Buurma-Rethans, E.J.M.; Ocké, M.C. Dutch National Food Consumption Survey 2007–2010: Diet of Children and Adults Aged 7 to 69 Years; RIVM Report Number: 350050006/2011; National Institute for Public Health and the Environment: Amsterdam, The Netherlands, 2011; p. 143. [Google Scholar]
- Sette, S.; Le Donne, C.; Piccinelli, R.; Arcella, D.; Turrini, A.; Leclercq, C. The third Italian National Food Consumption Survey, INRAN-SCAI 2005-06—Part 1: Nutrient intakes in Italy. Nut. Metab. Cardiovasc. Dis. 2011, 21, 922–932. [Google Scholar] [CrossRef] [PubMed]
- Irish Universities Nutrition Alliance (IUNA). National Adult Nutrition Survey; IUNA: Dublin, Ireland, 2011; p. 40. [Google Scholar]
- Agence Française de Sécurité Sanitaire des Aliments (AFSSA). Étude Individuelle Nationale des Consommations Alimentaires 2 (INCA 2) (2006–2007); Rapport 228; AFSSA: Maisons-Alfort, France, 2009. (In French) [Google Scholar]
- Bates, B.; Lennox, A.; Prentice, A.; Bates, C.; Swan, G. National Diet and Nutrition Survey. Headline Results from Years 1, 2 and 3 (Combined) of the Rolling Programme (2008/2009–2010/11); Department of Health and the Food Standards Agency: London, UK, 2011; p. 79.
- Becker, W.; Pearson, M. Riksmaten 1997–98. Dietary Habits and Nutrient Intake in Sweden 1997–98 (In Swedish/English Summary); Livsmedelsverket: Uppsala, Sweden, 2002. [Google Scholar]
- Harrington, J.; Perry, I.; Lutomski, J.; Morgan, K.; McGee, H.; Shelley, E.; Watson, D.; Barry, M. SLÁN 2007: Survey of Lifestyle, Attitudes and Nutrition in Ireland; Dietary Habits of the Irish Population, Department of Health and Children, The Stationery Office: Dublin, Ireland, 2008.
- Prentice, A. Vitamin D deficiency: A global perspective. Nutr. Rev. 2008, 66 (Suppl. 2), S153–S164. [Google Scholar] [CrossRef] [PubMed]
- Holick, M.F.; Binkley, N.C.; Bischoff-Ferrari, H.A.; Gordon, C.M.; Hanley, D.A.; Heaney, R.P.; Murad, M.H.; Weaver, C.M.; Endocrine Society. Evaluation, treatment, and prevention of vitamin D deficiency: An Endocrine Society clinical practice guideline. J. Clin. Endocrinol. Metab. 2011, 96, 1911–1930. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Misreporting Cut-Off | ||||
|---|---|---|---|---|
| Group Level | Individual Level | |||
| PAL | Lower | Upper | Lower | Upper |
| Children and adoles cents | ||||
| 1.6 | 1.55 | 1.66 | 0.93 | 2.76 |
| 1.8 | 1.73 | 1.86 | 1.04 | 3.10 |
| 2.0 | 1.93 | 2.07 | 1.16 | 3.45 |
| Adults and elderly | ||||
| 1.4 | 1.38 | 1.42 | 0.77 | 2.53 |
| 1.6 | 1.58 | 1.62 | 0.88 | 2.89 |
| 1.8 | 1.77 | 2.83 | 1.00 | 3.25 |
| Total | Children 9–12 Years | Adolescents 13–17 Years | Adults 18–64 Years | Elderly 65–75 Years | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | |
| CALCIUM (mg/day) | |||||||||||||||
| Total | 2009 | 698 ± 7 | 664 (71–2551) | 213 | 826 ± 17 a | 822 (302–1520) | 211 | 817 ± 23 a | 774 (155–1960) | 1655 | 689 ± 7 b | 659 (71–2551) | 206 | 645 ± 19 b | 622 (157–2206) |
| Men | 1013 | 726 ± 10 * | 681 (71–2551) | 126 | 872 ± 22 * | 856 (302–1520) | 137 | 875 ± 31 * | 831 (174–1960) | 798 | 711 ± 11 * | 668 (71–2551) | 99 | 662 ± 31 | 642 (223–2206) |
| Women | 996 | 670 ± 8 | 650 (118–2399) | 87 | 759 ± 26 | 763 (305–1500) | 74 | 708 ± 29 | 667 (155–1276) | 857 | 668 ± 9 | 650 (118–2399) | 107 | 629 ± 21 | 613 (157–1344) |
| PHOSPHORUS (mg/day) | |||||||||||||||
| Total | 2009 | 1176 ± 8 | 1134 (331–4429) | 213 | 1285 ± 22 a | 1286 (433–2086) | 211 | 1261 ± 24 a | 1240 (414–2268) | 1655 | 1175 ± 9 b | 1128 (331–4429) | 206 | 1097 ± 23 c | 1058 (453–2921) |
| Men | 1013 | 1246 ± 12 * | 1200 (433–4429) | 126 | 1340 ± 27 * | 1362 (433–2086) | 137 | 1323 ± 31 * | 1310 (441–2268) | 798 | 1247 ± 14 * | 1197 (474–4429) | 99 | 1177 ± 38 * | 1117 (463–2921) |
| Women | 996 | 1104 ± 9 | 1080 (331–2396) | 87 | 1206 ± 35 | 1184 (646–1972) | 74 | 1145 ± 35 | 1140 (414–1953) | 857 | 1108 ± 10 | 1082 (331–2396) | 107 | 1023 ± 25 | 1014 (453–1919) |
| MAGNESIUM (mg/day) | |||||||||||||||
| Total | 2009 | 222 ± 2 | 213 (73–782) | 213 | 220 ± 4 | 221 (75–471) | 211 | 216 ± 4 | 214 (80–410) | 1655 | 223 ± 2 | 213 (73–782) | 206 | 226 ± 6 | 210 (103–736) |
| Men | 1013 | 233 ± 2 * | 224 (80–782) | 126 | 224 ± 5 | 222 (75–427) | 137 | 224 ± 5 * | 224 (80–410) | 798 | 236 ± 3 * | 225 (80–782) | 99 | 246 ± 11 * | 222 (110–736) |
| Women | 996 | 210 ± 2 | 204 (73–592) | 87 | 214 ± 7 | 213 (124–471) | 74 | 200 ± 7 | 195 (93–387) | 857 | 211 ± 2 | 204 (73–592) | 107 | 207 ± 6 | 201 (103–430) |
| VITAMIN D (µg/day) | |||||||||||||||
| Total | 2009 | 4.4 ± 0.1 | 2.6 (0.0–74.2) | 213 | 2.8 ± 0.2 a | 1.7 (0.1–13.5) | 211 | 3.7 ± 0.4 a,b | 1.8 (0.0–73.9) | 1655 | 4.5 ± 0.1 b | 2.9 (0.0–74.2) | 206 | 4.4 ± 0.4 b | 2.8 (0.0–34.2) |
| Men | 1013 | 4.4 ± 0.2 | 2.6 (0.0–74.2) | 126 | 2.6 ± 0.2 | 1.7 (0.1–12.2) | 137 | 4.0 ± 0.6 | 2.0 (0.0–73.9) | 798 | 4.7 ± 0.2 | 2.8 (0.0–74.2) | 99 | 4.5 ± 0.5 | 3.2 (0.0–30.7) |
| Women | 996 | 4.3 ± 0.2 | 2.7 (0.0–47.2) | 87 | 3.0 ± 0.3 | 1.8 (0.2–13.5) | 74 | 3.1 ± 0.5 | 1.2 (0.1–29.4) | 857 | 4.4 ± 0.2 | 2.9 (0.0–47.2) | 107 | 4.3 ± 0.5 | 2.6 (0.1–34.6) |
| Total | Children 9–12 Years | Adolescents 13–17 Years | Adults 18–64 Years | Elderly 65–75 Years | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | n | Mean ± SEM | Median (Range) | |
| CALCIUM (mg/day) | |||||||||||||||
| Total | 2009 | 698 ± 7 | 664 (71–2551) | 213 | 826 ± 17 | 822 (302–1520) | 211 | 817 ± 23 | 774 (155–1960) | 1655 | 689 ± 7 | 659 (71–2551) | 206 | 645 ± 19 | 622 (157–2206) |
| Plausible reporters | 543 | 862 ± 14 | 824 (265–2399) | 120 | 893 ± 22 | 876 (337–1520) | 76 | 978 ± 39 | 959 (324–1960) | 433 | 853 ± 16 | 790 (265–2399) | 45 | 807 ± 47 | 795 (300–1943) |
| Men | 232 | 934 ± 23 | 871 (300–2109) | 68 | 954 ± 29 | 940 (337–1520) | 48 | 1049 ± 55 | 991 (324–1960) | 158 | 938 ± 29 | 851 (71–2551) | 24 | 857 ± 71 | 821 (300–1943) |
| Women | 311 | 807 ± 16 | 778 (265–2399) | 52 | 812 ± 32 | 821 (354–1493) | 28 | 855 ± 43 | 834 (527–1276) | 275 | 804 ± 17 | 761 (265–2399) | 21 | 750 ± 59 | 705 (363–1344) |
| Non–Plausible reporters | 1466 | 637 ± 7 | 613 (71–2551) | 93 | 739 ± 25 | 770 (302–1500) | 135 | 726 ± 26 | 675 (155–1855) | 1222 | 631 ± 7 | 605 (71–2551) | 161 | 600 ± 18 | 572 (157–2206) |
| Men | 781 | 664 ± 10 | 631 (71–2551) | 58 | 775 ± 30 | 776 (302–1342) | 89 | 782 ± 35 | 725 (174–1855) | 640 | 655 ± 11 | 625 (71–2551) | 75 | 600 ± 31 | 553 (223–2206) |
| Women | 685 | 607 ± 9 | 585 (118–1684) | 35 | 681 ± 41 | 637 (305–1500) | 46 | 619 ± 32 | 627 (155–1088) | 582 | 604 ± 9 | 579 (118–1684) | 86 | 600 ± 21 | 590 (157–1052) |
| PHOSPHORUS (mg/day) | |||||||||||||||
| Total | 2009 | 1176 ± 8 | 1134 (331–4429) | 213 | 1285 ± 22 | 1286 (433–2086) | 211 | 1261 ± 24 | 1240 (414–2268) | 1655 | 1175 ± 9 | 1128 (331–4429) | 206 | 1097 ± 23 | 1058 (453–2921) |
| Plausible reporters | 543 | 1434 ± 14 | 1401 (708–3300) | 120 | 1408 ± 24 | 1395 (795–2086) | 76 | 1502 ± 33 | 1502 (883–2268) | 433 | 1433 ± 17 | 1396 (708–3300) | 45 | 1410 ± 51 | 1392 (885–2415) |
| Men | 232 | 1587 ± 23 | 1532 (901–3300) | 68 | 1456 ± 29 | 1447 (949–2086) | 48 | 1583 ± 41 | 1548 (984–2268) | 158 | 1638 ± 30 | 1600 (901–3300) | 24 | 1537 ± 72 | 1469 (928–2415) |
| Women | 311 | 1321 ± 16 | 1304 (708–2396) | 52 | 1344 ± 39 | 1317 (795–1972) | 28 | 1362 ± 48 | 1329 (883–1953) | 275 | 1315 ± 17 | 1288 (708–2396) | 21 | 1265 ± 57 | 1270 (885–1919) |
| Non–Plausible reporters | 1466 | 1080 ± 8 | 1048 (331–4429) | 93 | 1128 ± 32 | 1098 (433–1989) | 135 | 1125 ± 26 | 1111 (414–2083) | 1222 | 1084 ± 9 | 1047 (331–4429) | 161 | 1009 ± 21 | 993 (453–2921) |
| Men | 781 | 1145 ± 12 | 1114 (433–4429) | 58 | 1203 ± 40 | 1189 (433–1989) | 89 | 1183 ± 34 | 1162 (441–2083) | 640 | 1151 ± 13 | 1119 (474–4429) | 75 | 1061 ± 36 | 1034 (463–2921) |
| Women | 685 | 1006 ± 10 | 991 (331–1920) | 35 | 1002 ± 46 | 960 (646–1756) | 46 | 1012 ± 36 | 1021 (414–1558) | 582 | 1010 ± 11 | 987 (331–1929) | 86 | 963 ± 24 | 982 (453–1749) |
| MAGNESIUM (mg/day) | |||||||||||||||
| Total | 2009 | 222 ± 2 | 213 (73–782) | 213 | 220 ± 4 | 221 (75–471) | 211 | 216 ± 4 | 214 (80–410) | 1655 | 223 ± 2 | 213 (73–782) | 206 | 226 ± 6 | 210 (103–736) |
| Plausible reporters | 543 | 273 ± 3 | 261 (122–669) | 120 | 242 ± 5 | 241 (142–427) | 76 | 263 ± 6 | 255 (166–410) | 433 | 278 ± 4 | 266 (122–669) | 45 | 300 ± 16 | 26 (165–736) |
| Men | 232 | 301 ± 5 | 287 (154–669) | 68 | 248 ± 6 | 248 (146–427) | 48 | 274 ± 8 | 275 (178–410) | 158 | 319 ± 6 | 300 (188–669) | 24 | 327 ± 27 | 266 (184–736) |
| Women | 311 | 253 ± 4 | 244 (122–592) | 52 | 233 ± 7 | 237 (142–389) | 28 | 242 ± 9 | 235 (166–387) | 275 | 254 ± 4 | 246 (122–592) | 21 | 269 ± 15 | 253 (165–430) |
| Non–Plausible reporters | 1466 | 203 ± 2 | 197 (73–782) | 93 | 192 ± 6 | 182 (75–471) | 135 | 189 ± 4 | 188 (80–298) | 1222 | 204 ± 2 | 197 (73–782) | 161 | 205 ± 5 | 200 (101–641) |
| Men | 781 | 214 ± 2 | 207 (80–782) | 58 | 196 ± 7 | 189 (75–350) | 89 | 197 ± 5 | 192 (80–298) | 640 | 215 ± 3 | 207 (80–782) | 75 | 220 ± 9 | 210 (110–641) |
| Women | 685 | 191 ± 2 | 188 (73–591) | 35 | 185 ± 11 | 179 (124–471) | 46 | 175 ± 6 | 172 (93–253) | 582 | 191 ± 2 | 187 (73–591) | 86 | 192 ± 5 | 188 (103–327) |
| VITAMIN D (µg/day) | |||||||||||||||
| Total | 2009 | 4.4 ± 0.1 | 2.6 (0.0–74.2) | 213 | 2.8 ± 0.2 | 1.7 (0.1–13.5) | 211 | 3.7 ± 0.4 | 1.8 (0.0–73.7) | 1655 | 4.5 ± 0.1 | 2.9 (0.0–74.2) | 206 | 4.4 ± 0.4 | 2.8 (0.0–34.6) |
| Plausible reporters | 543 | 5.5 ± 0.3 | 3.6 (0.1–47.2) | 120 | 3.2 ± 0.3 | 2.0 (0.2–12.8) | 76 | 3.8 ± 0.5 | 2.0 (0.1–20.9) | 433 | 5.8 ± 0.3 | 4.1 (0.1–47.2) | 45 | 6.7 ± 0.9 | 5.2 (0.4–30–7) |
| Men | 232 | 5.5 ± 0.4 | 3.9 (0.1–38.3) | 68 | 3.0 ± 0.3 | 1.9 (0.2–12.2) | 48 | 4.0 ± 0.6 | 2.0 (0.1–20.9) | 158 | 5.9 ± 0.5 | 4.4 (0.1–38.3) | 24 | 8.0 ± 1.3 | 6.3 (1.0–30.7) |
| Women | 311 | 5.5 ± 0.4 | 3.5 (0.1–47.2) | 52 | 3.3 ± 0.4 | 2.5 (0.2–12.8) | 28 | 3.3 ± 0.8 | 1.5 (0.4–18.2) | 275 | 5.7 ± 0.4 | 3.9 (0.1–47.2) | 21 | 5.2 ± 1.2 | 3.3 (0.4–20.9) |
| Non–Plausible reporters | 1466 | 4.0 ± 0.1 | 2.3 (0.0–74.2) | 93 | 2.3 ± 0.2 | 1.3 (0.1–13.5) | 135 | 3.7 ± 0.6 | 1.8 (0.0–73.9) | 1222 | 4.1 ± 0.1 | 2.5 (0.0–74.2) | 161 | 3.8 ± 0.4 | 2.2 (0.0–34.6) |
| Men | 781 | 4.1 ± 0.2 | 2.3 (0.0–74.2) | 58 | 2.2 ± 0.3 | 1.3 (0.1–9.2) | 89 | 4.0 ± 0.9 | 1.9 (0.0–73.9) | 640 | 4.3 ± 0.2 | 2.5 (0.0–74.2) | 75 | 3.4 ± 0.4 | 2.2 (0.0–15.6) |
| Women | 685 | 3.8 ± 0.2 | 2.3 (0.0–37.2) | 35 | 2.5 ± 0.5 | 1.5 (0.2–13.5) | 46 | 2.9 ± 0.7 | 1.0 (0.0–29.4) | 582 | 3.7 ± 0.2 | 2.4 (0.0–37.2) | 86 | 4.1 ± 0.6 | 2.2 (0.1–34.6) |
| Total | Children 9–12 Years | Adolescents 13–17 Years | Adults 18–64 Years | Elderly 65–75 Years | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Spain | EFSA | Spain | EFSA | Spain | EFSA | Spain | EFSA | Spain | EFSA | |
| CALCIUM (%) | ||||||||||
| Whole population | 76 | 66 | 62 | 38 | 78 | 65 | 74 | 66 | 90 | 73 |
| Men | 72 | 63 | 57 | 29 | 71 | 58 | 70 | 64 | 88 | 71 |
| Women | 80 | 69 | 68 | 53 | 91 | 77 | 78 | 68 | 92 | 75 |
| Plausible reporters | 56 | 44 | 48 | 23 | 65 | 45 | 55 | 47 | 67 | 49 |
| Men | 49 | 37 | 44 | 12 | 54 | 35 | 45 | 40 | 63 | 46 |
| Women | 61 | 50 | 52 | 38 | 79 | 61 | 60 | 51 | 71 | 52 |
| MAGNESIUM (%) | ||||||||||
| Whole population | 79 | 72 | 65 | 48 | 90 | 57 | 78 | 73 | 79 | 79 |
| Men | 78 | 74 | 69 | 53 | 91 | 60 | 76 | 76 | 81 | 81 |
| Women | 80 | 70 | 59 | 40 | 89 | 51 | 80 | 71 | 77 | 77 |
| Plausible reporters | 53 | 40 | 49 | 29 | 72 | 26 | 51 | 41 | 44 | 44 |
| Men | 45 | 38 | 57 | 34 | 73 | 29 | 35 | 35 | 54 | 54 |
| Women | 58 | 42 | 38 | 23 | 71 | 21 | 60 | 45 | 33 | 33 |
| VITAMIN D (%) | ||||||||||
| Whole population | 94 | 93 | 99 | 99 | 95 | 95 | 93 | 93 | 97 | 94 |
| Men | 93 | 93 | 99 | 99 | 94 | 94 | 92 | 92 | 99 | 93 |
| Women | 94 | 94 | 98 | 98 | 97 | 97 | 94 | 94 | 95 | 94 |
| Plausible reporters | 90 | 89 | 98 | 98 | 93 | 93 | 89 | 88 | 94 | 84 |
| Men | 91 | 89 | 99 | 99 | 92 | 92 | 88 | 88 | 96 | 79 |
| Women | 89 | 89 | 98 | 98 | 96 | 96 | 89 | 89 | 90 | 90 |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Olza, J.; Aranceta-Bartrina, J.; González-Gross, M.; Ortega, R.M.; Serra-Majem, L.; Varela-Moreiras, G.; Gil, Á. Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study †. Nutrients 2017, 9, 168. https://doi.org/10.3390/nu9020168
Olza J, Aranceta-Bartrina J, González-Gross M, Ortega RM, Serra-Majem L, Varela-Moreiras G, Gil Á. Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study †. Nutrients. 2017; 9(2):168. https://doi.org/10.3390/nu9020168
Chicago/Turabian StyleOlza, Josune, Javier Aranceta-Bartrina, Marcela González-Gross, Rosa M. Ortega, Lluis Serra-Majem, Gregorio Varela-Moreiras, and Ángel Gil. 2017. "Reported Dietary Intake, Disparity between the Reported Consumption and the Level Needed for Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D in the Spanish Population: Findings from the ANIBES Study †" Nutrients 9, no. 2: 168. https://doi.org/10.3390/nu9020168