Dual-Wavelength Laser Speckle Contrast Imaging (dwLSCI) Improves Chronic Measurement of Superficial Blood Flow in Hands

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Methods and Experiments
2.1. Theory
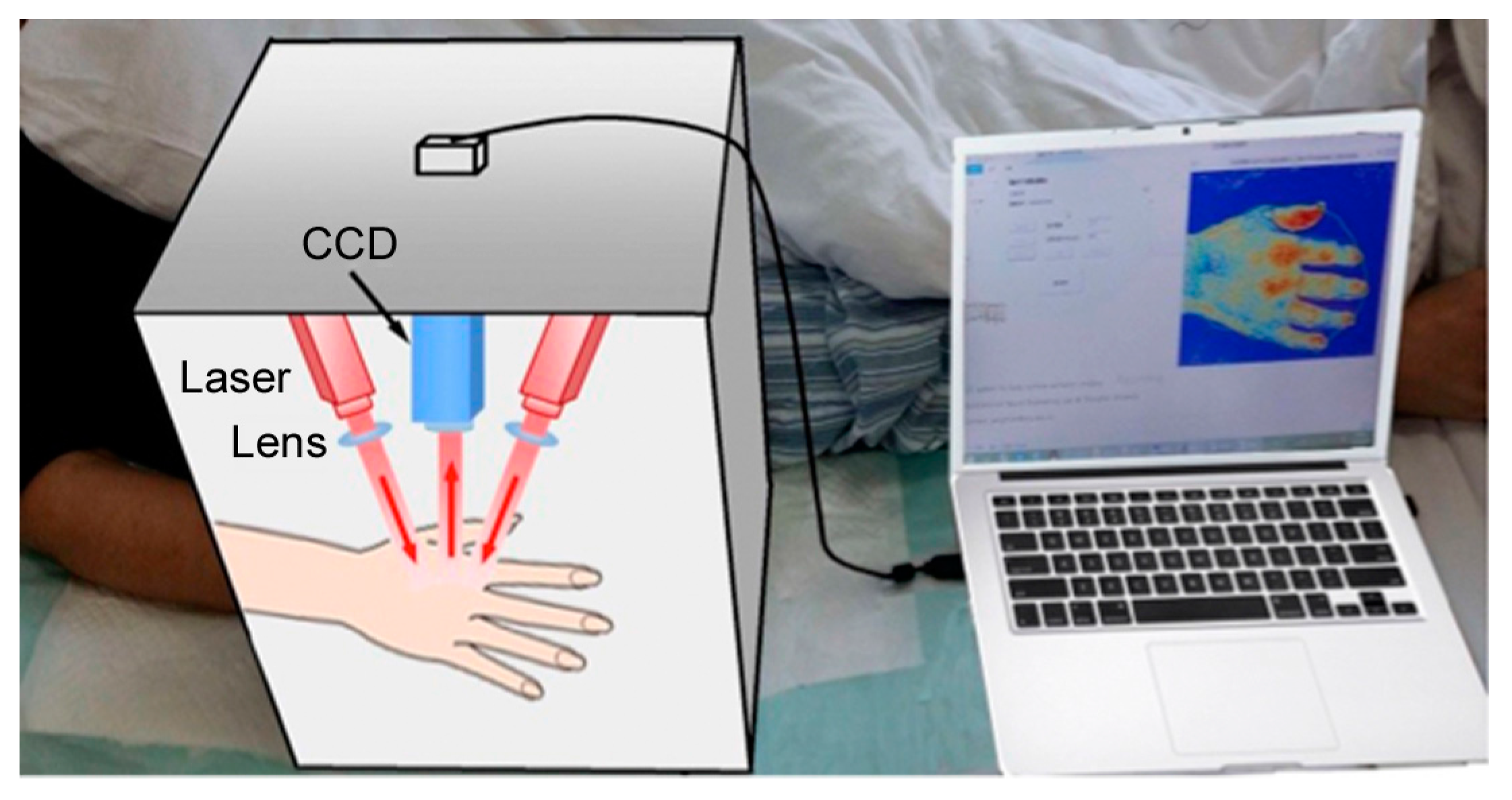
2.2. Equipment and Data Processing
2.3. Experiments
3. Results
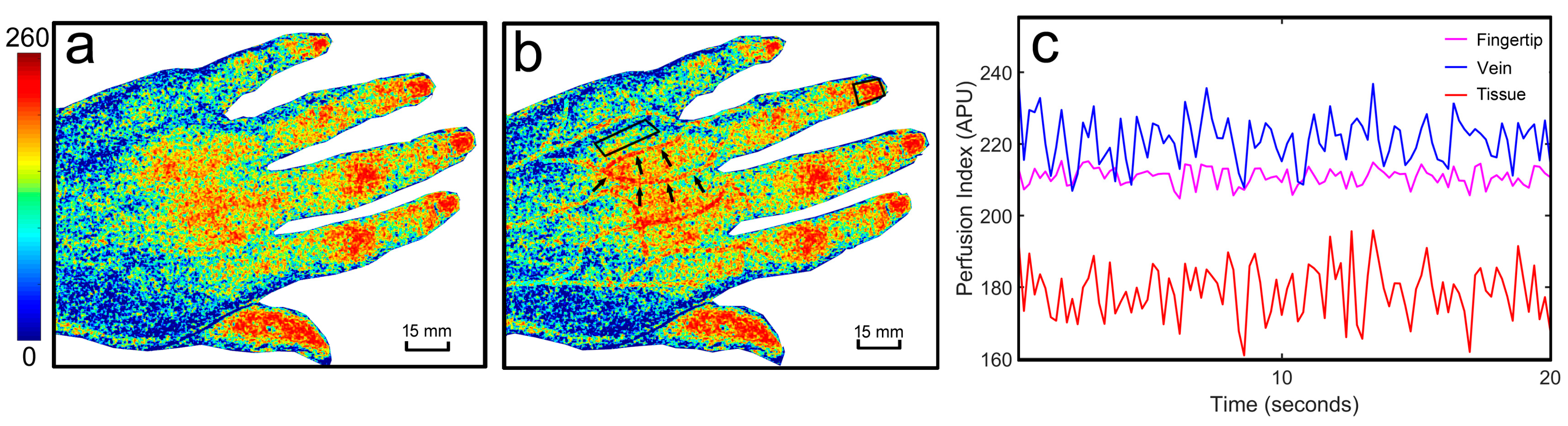
3.1. The dwLSCI Improvement of Superficial Blood Flow Imaging
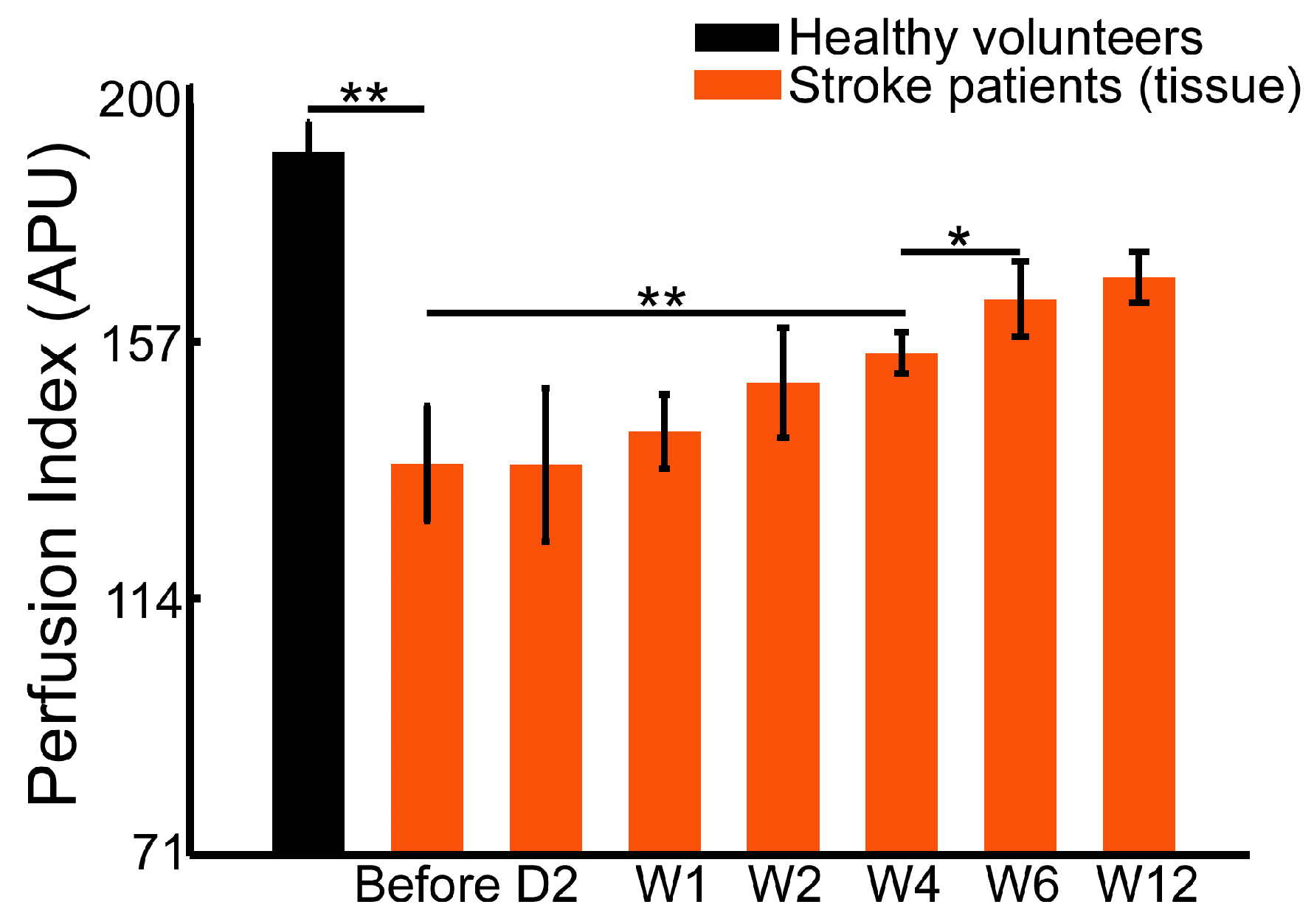
3.2. Healthy Volunteers Demonstrate Higher Superficial Perfusion of Hands than Stroke Patients
3.3. Early Stage Rehabilitation Therapy Improves Fingertip Perfusion
3.4. Blood Flow in the Superficial Veins and Surrounding Tissue Perfusion in Hands Demonstrates Different Recovering Patterns during Rehabilitation Therapy
4. Discussion
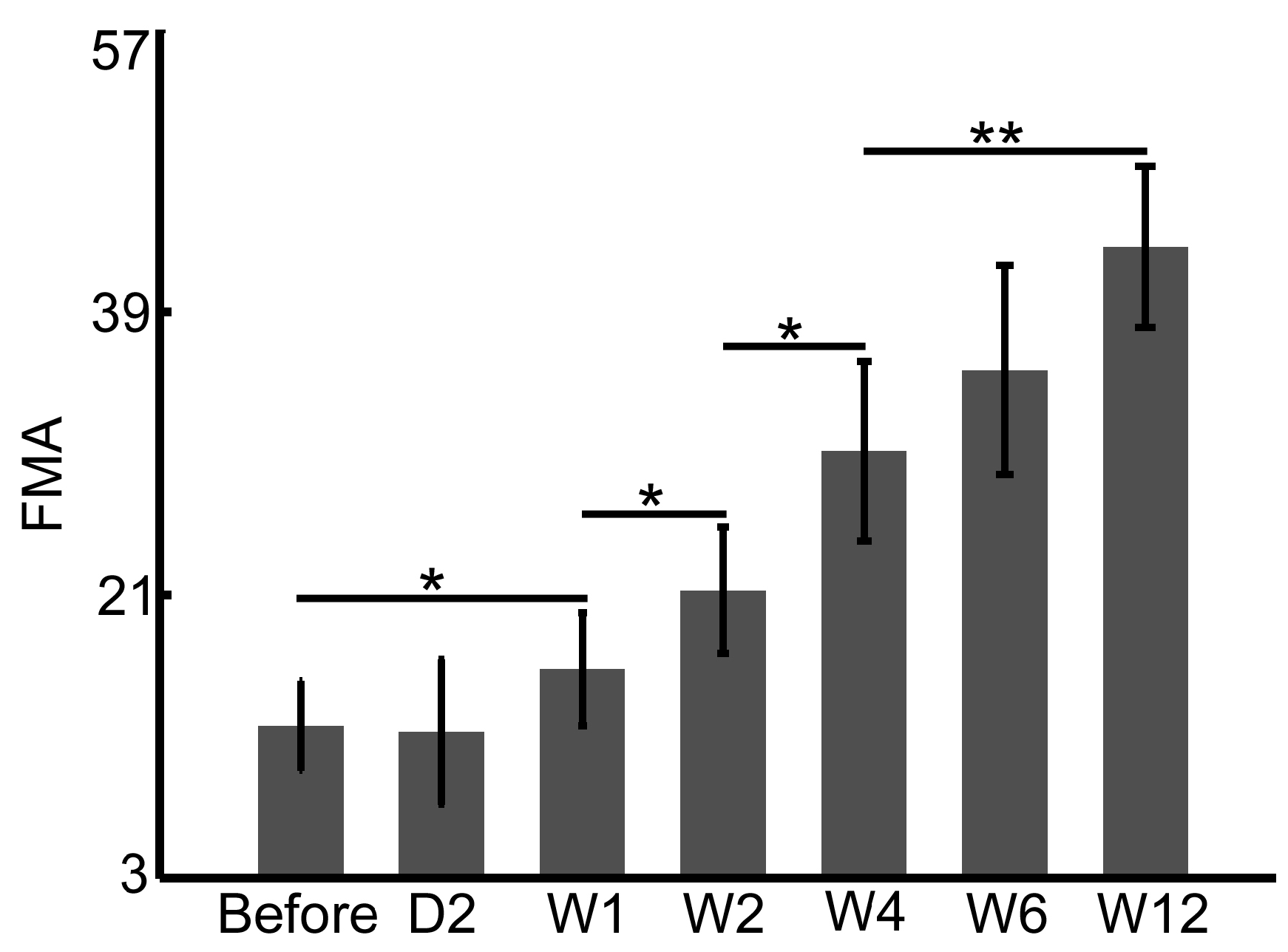
4.1. FMA and WMFT Demonstrate Limitations in the Early Assessment of Rehabilitation Therapy
4.2. Perfusion Signal in Fingertips Provides More Sensitive Monitoring of Early Rehabilitation
4.3. Perfusion and Flow Measurements Assist the Quantitative Assessment of Behavior Testing
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Huerta, T.E.; Norton, P.T.; Chhabra, B.; Drake, D.B.; Arnold, P.B.; Housseini, A.M.; Hagspiel, K.D. Comprehensive Magnetic resonance imaging of the hand and forearm vasculature at 3 Tesla using time-resolved angiography with stochastic trajectories (TWIST): Preliminary clinical results. Proc. Int. Soc. Magn. Reson. Med. 2009, 17, 3876. [Google Scholar]
- Sosa, J.M.; Nielsen, N.D.; Vignes, S.M.; Chen, T.G.; Shevkoplyas, S.S. The relationship between red blood cell deformability metrics and perfusion of an artificial microvascular network. Clin. Hemorheol. Microcirc. 2014, 57, 275–289. [Google Scholar] [PubMed]
- Budimkic, M.S.; Pekmezovic, T.; Beslac-Bumbasirevic, L.; Ercegovac, M.; Berisavac, I.; Stanarcevic, P.; Padjen, V.; Jovanovic, D.R. Long-term medication persistence in stroke patients treated with intravenous thrombolysis. Clin. Neurol. Neurosurg. 2015, 141, 19–22. [Google Scholar] [CrossRef] [PubMed]
- Saeki, S.; Chisaka, H.; Hachisuka, K. Life satisfaction and functional disabilities in long-term survivors after first stroke. J. UOEH 2005, 27, 171–177. [Google Scholar] [CrossRef] [PubMed]
- McKevitt, C.; Fudge, N.; Redfern, J.; Sheldenkar, A.; Crichton, S.; Rudd, A.R.; Forster, A.; Young, J.; Nazareth, I.; Silver, L.E.; et al. Self-reported long-term needs after stroke. Stroke 2011, 42, 1398–1403. [Google Scholar] [CrossRef] [PubMed]
- Nobutoki, T.; Ihara, T. Early disruption of neurovascular units and microcirculatory dysfunction in the spinal cord in spinal muscular atrophy type I. Med. Hypotheses 2015, 85, 842–845. [Google Scholar] [CrossRef] [PubMed]
- Van der Lee, J.H.; Beckerman, H.; Lankhorst, G.J.; Bouter, L.M. The responsiveness of the Action Research Arm test and the Fugl-Meyer Assessment scale in chronic stroke patients. J. Rehabil. Med. 2001, 33, 110–113. [Google Scholar] [PubMed]
- Padovani, C.; Pires, C.V.G.; Ferreira, F.P.C.; Borin, G.; Filippo, T.R.M.; Imamura, M.; Rosa, C.D.P.; Battistella, L.R. Application of the Fugl-Meyer Assessment (FMA) and the Wolf Motor Function Test (WMFT) in the recovery of upper limb function in patients after chronic stroke: A literature review. Acta Fisiatr. 2016, 20, 42–49. [Google Scholar] [CrossRef]
- Gutzeit, A.; Eckhardt, B.; Beranek, J.; Wentz, K.U.; Willemse, E.; Jenelten, R.; Binkert, C.A.; Froehlich, J.M. Clinical experience in timed arterial compression contrast-enhanced magnetic resonance angiography of the hand. Can. Assoc. Radiol. J. 2010, 61, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Fan, Z.; Hodnett, P.A.; Davarpanah, A.H.; Scanlon, T.G.; Sheehan, J.J.; Varga, J.; Carr, J.C.; Li, D. Noncontrast MR angiography of the hand: Improved arterial conspicuity by multi-directional flow-sensitive dephasing magnetization preparation in 3D Balanced SSFP Imaging. Investig. Radiol. 2011, 46, 515–523. [Google Scholar] [CrossRef] [PubMed]
- Connel, D.A.; Koulouris, G.; Thorn, D.A.; Potter, H.G. Contrast-enhanced MR angiography of the hand. RadioGraphics 2002, 22, 583–599. [Google Scholar] [CrossRef] [PubMed]
- Gardner-Medwin, J.M.; Taylor, J.Y.; Macdonald, I.A.; Powell, R.J. An investigation into variability in microvascular skin blood flow and the responses to transdermal delivery of acetylcholine at different sites in the forearm and hand. Br. J. Clin. Pharmacol. 1997, 43, 391–397. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Nguyen, H.C.; Hayes-Gill, B.R.; Zhu, Y.; Crowe, J.A.; Gill, C.; Clough, G.F.; Morgan, S.P. Laser Doppler blood flow imaging using a CMOS imaging sensor with on-chip signal processing. Sensors 2013, 13, 12632–12647. [Google Scholar] [CrossRef] [PubMed]
- Iwasaki, W.; Nogami, H.; Takeuchi, S.; Furue, M.; Higurashi, E.; Sawada, R. Detection of site-specific blood flow variation in humans during running by a wearable laser Doppler flowmeter. Sensors 2015, 15, 25507–25519. [Google Scholar] [CrossRef] [PubMed]
- Pauling, J.D.; Shipley, J.A.; Raper, S.; Watson, M.L.; Ward, S.G.; Harris, N.D.; McHugh, N.J. Comparison of infrared thermography and laser speckle contrast imaging for the dynamic assessment of digital microvascular function. Microvasc. Res. 2012, 83, 162–167. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Moon, S.; Lim, J.; Gwak, M.-J.; Kim, J.G.; Chung, E.; Lee, J.-H. Imaging of the finger vein and blood flow for anti-spoofing authentication using a laser and a MEMS scanner. Sensors 2017, 17, 925. [Google Scholar] [CrossRef] [PubMed]
- Zötterman, J.; Bergkvist, M.; Iredahl, F.; Tesselaar, E.; Farnebo, S. Monitoring of partial and full venous outflow obstruction in a porcine flap model using laser speckle contrast imaging. J. Plast. Reconstr. Aesthet. Surg. 2016, 69, 936–943. [Google Scholar] [CrossRef] [PubMed]
- Pauling, J.D.; Shipley, J.A.; Hart, D.J.; McGrogan, A.; McHugh, N.J. Use of laser speckle contrast imaging to assess digital microvascular function in primary Raynaud phenomenon and systemic sclerosis: A comparison using the Raynaud condition score diary. J. Rheumatol. 2015, 42, 1163–1168. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Iredahl, F.; Löfberg, A.; Sjöberg, F.; Farnebo, S.; Tesselaar, E. Non-invasive measurement of skin microvascular response during pharmacological and physiological provocations. PLoS ONE 2015, 10, e0133760. [Google Scholar] [CrossRef] [PubMed]
- Jeong, Y.; Li, G.; Lee, D.; Lee, B. Simplified multi-wavelength laser speckle contrast imaging system by using single holographic optical element. Imaging Appl. Opt. 2016. [Google Scholar] [CrossRef]
- Dunn, A.K.; Devor, A.; Bolay, H.; Andermann, M.L.; Moskowitz, M.A.; Dale, A.M.; Boas, D.A. Simultaneous imaging of total cerebral hemoglobin concentration oxygenation and blood flow during functional activation. Opt. Lett. 2003, 28, 28–30. [Google Scholar] [CrossRef] [PubMed]
- Dunn, A.K.; Devor, A.; Dale, A.M.; Boas, D.A. High resolution imaging of the hemodynamic and metabolic response to functional activation. In Proceedings of the Biomedical Topical Meeting, Miami Beach, FL, USA, 14–17 April 2004. [Google Scholar]
- Chen, W.; Park, K.; Pan, Y.; Du, C. Abnormal hemodynamic response to forepaw stimulation in rat brain after cocaine injection. In Optical Techniques in Neurosurgery, Neurophotonics, and Optogenetics II; International Society for Optics and Photonics (SPIE): Bellingham, WA, USA, 2015. [Google Scholar]
- Chen, W.; Park, K.; Volkow, N.; Pan, Y.; Du, C. Cocaine-induced abnormal cerebral hemodynamic responses to forepaw stimulation assessed by integrated multi-wavelength spectroimaging and laser speckle contrast imaging. IEEE J. Sel. Top. Quantum Electron. 2016, 22, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Khaksari, K.; Kirkpatrick, S.J. Laser speckle contrast imaging is sensitive to advective flux. J. Biomed. Opt. 2016, 21, 076001. [Google Scholar] [CrossRef] [PubMed]
- Miao, P.; Chao, Z.; Feng, S.; Yu, H.; Ji, Y.; Li, N.; Thakor, N.V. Local scattering property scales flow speed estimation in laser speckle contrast imaging. Laser Phys. Lett. 2015, 12, 075601. [Google Scholar] [CrossRef]
- Khaksari, K.; Kirkpatrick, S.J. Combined effects of scattering and absorption on laser speckle contrast imaging. J. Biomed. Opt. 2016, 21, 76002. [Google Scholar] [CrossRef] [PubMed]
- Luo, Z.; Yuan, Z.; Pan, Y.; Du, C. Simultaneous imaging of cortical hemodynamics and blood oxygenation change during cerebral ischemia using dual-wavelength laser speckle contrast imaging. Opt. Lett. 2009, 34, 1480–1482. [Google Scholar] [CrossRef] [PubMed]
- Qin, J.; Shi, L.; Dziennis, S.; Reif, R.; Wang, R.K. Fast synchronized dual-wavelength laser speckle imaging system for monitoring hemodynamic changes in a stroke mouse model. Opt. Lett. 2012, 37, 4005–4007. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Wang, Y.; Li, B.; Feng, D.; Lu, J.; Luo, Q.; Li, P. Dual-wavelength laser speckle imaging to simultaneously access blood flow, blood volume, and oxygenation using a color CCD camera. Opt. Lett. 2013, 38, 3690–3692. [Google Scholar] [CrossRef] [PubMed]
- Briers, J.D.; Webster, S. Laser speckle contrast analysis (LASCA): A nonscanning, full-field technique for monitoring capillary blood flow. J. Biomed. Opt. 1996, 1, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Li, P.; Ni, S.; Zhang, L.; Zeng, S.; Luo, Q. Imaging cerebral blood flow through the intact rat skull with temporal laser speckle imaging. Opt. Lett. 2006, 31, 1824–1826. [Google Scholar] [CrossRef] [PubMed]
- Miao, P.; Li, N.; Thakor, N.V.; Tong, S. Random process estimator for laser speckle imaging of cerebral blood flow. Opt. Express 2010, 18, 218–236. [Google Scholar] [CrossRef] [PubMed]
- Boas, D.A.; Dunn, A.K. Laser speckle contrast imaging in biomedical optics. J. Biomed. Opt. 2010, 15, 011109. [Google Scholar] [CrossRef] [PubMed]
- Avci, P.; Gupta, A.; Sadasivam, M.; Vecchio, D.; Pam, Z.; Pam, N.; Hamblin, M.R. Low-level laser (light) therapy (LLLT) in skin: Stimulating, healing, restoring. Semin. Cutan. Med. Surg. 2013, 32, 41–52. [Google Scholar] [PubMed]
- McLaren, C.E.; Brittenham, G.M.; Hasselblad, V. Statistical and graphical evaluation of erythrocyte volume distributions. Am. J. Physiol. 1987, 252, 857–866. [Google Scholar]
- Steinke, J.M.; Shepherd, A.P. Comparison of Mie theory and the light scattering of red blood cells. Appl. Opt. 1988, 27, 4027–4033. [Google Scholar] [CrossRef] [PubMed]







© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhang, L.; Ding, L.; Li, M.; Zhang, X.; Su, D.; Jia, J.; Miao, P. Dual-Wavelength Laser Speckle Contrast Imaging (dwLSCI) Improves Chronic Measurement of Superficial Blood Flow in Hands. Sensors 2017, 17, 2811. https://doi.org/10.3390/s17122811
Zhang L, Ding L, Li M, Zhang X, Su D, Jia J, Miao P. Dual-Wavelength Laser Speckle Contrast Imaging (dwLSCI) Improves Chronic Measurement of Superficial Blood Flow in Hands. Sensors. 2017; 17(12):2811. https://doi.org/10.3390/s17122811
Chicago/Turabian StyleZhang, Lingke, Li Ding, Miao Li, Xiaoli Zhang, Diansan Su, Jie Jia, and Peng Miao. 2017. "Dual-Wavelength Laser Speckle Contrast Imaging (dwLSCI) Improves Chronic Measurement of Superficial Blood Flow in Hands" Sensors 17, no. 12: 2811. https://doi.org/10.3390/s17122811