
Who Benefits from Public Healthcare Subsidies in Egypt?


1
Department of Economics, Philipps-Universität Marburg, Marburg 35037, Germany
2
Department of Economics, Faculty of Commerce, Damanhour University, Damanhour 22514, Egypt
3
Department of Economics, Faculty of Arts, University of Alberta, Edmonton, AB T6G 2H4, Canada
*
Author to whom correspondence should be addressed.
Soc. Sci. 2015, 4(4), 1162-1176; https://doi.org/10.3390/socsci4041162
Submission received: 20 August 2015
/
Revised: 10 November 2015
/
Accepted: 19 November 2015
/
Published: 25 November 2015
(This article belongs to the Special Issue Reinventing Healthy Communities: Implications for Individual and Societal Well-Being)
Abstract
:Direct subsidization of healthcare services has been widely used in many countries to improve health outcomes. It is commonly believed that the poor are the main beneficiaries from these subsidies. We test this hypothesis in Egypt by empirically analyzing the distribution of public healthcare subsidies using data from Egypt Demographic and Health Survey and Egypt National Health Accounts. To determine the distribution of public health care subsidies, we conducted a Benefit Incidence Analysis. As a robustness check, both concentration and Kakwani indices for outpatient, inpatient, and total healthcare were also calculated. Results show some degree of inequality in the benefits from public healthcare services, which varied by the type of healthcare provided. In particular, subsidies associated with University hospitals are pro-rich and have inequality increasing effect, while subsidies associated with outpatient and inpatient care provided by the Ministry of Health and Population have not been pro-poor but have inequality reducing effect (weakly progressive). Results were robust to the different analytical methods. While it is widely perceived that the poor benefit the most from health subsidies, the findings of this study refute this hypothesis in the case of Egypt. Poverty reduction measures and healthcare reforms in Egypt should not only focus on expanding the coverage of healthcare benefits, but also on improving the equity of its distribution.
1. Introduction
The World Health Organization (WHO) has been calling for a sustainable and equitable financing and delivery of healthcare services. This is to improve access to healthcare, offer greater financial protection to the poor and to combat poverty, hunger, and diseases, which are key ingredients of the United Nations Millennium Development Goals [1].
Adequate access to healthcare services is crucial for increasing productivity of the labor force, and hence economic growth. In the absence of universal health insurance coverage, subsidization of healthcare becomes essential to ensure that the poor can afford access to health services. Direct subsidization of healthcare services has been widely used as an effective policy instrument to improve health levels in many developing countries. Health subsidies could reduce income inequalities if the subsidy is benefiting the poor more than rich. Thus, the effect of the subsidies on income distribution depends on the distribution of the subsidization benefits across different economic classes.
Egypt has been adopting a subsidized healthcare system for several decades. It is commonly believed that the poor are the main beneficiaries from these subsidies. The objective of the current study is to test this hypothesis in Egypt by empirically analyzing the distribution of public healthcare subsidies using nationally representative data from Egypt Demographic and Health Survey.
Following the establishment of the Republic of Egypt in 1952, the new socialist regime has relied on a redistribution system that promoted a minimum standard of living by providing universal subsidies of basic consumption goods [2]. Egypt has one of the biggest subsidy programs that cover food and energy on a massive scale. In the health sector, the government of Egypt has pledged to provide free healthcare to all citizens. Right of access to healthcare is a constitutional right in Egypt, and the government uses general tax revenue to provide subsidized healthcare services.
Over the period 2000 to 2009, public health spending in Egypt accounted for 6% of the total public spending. This is far behind the Abuja target of allocating 15% of total government spending to health. The subsidized health system is under continuous population pressure resulting from the significant increase in life expectancy and the high fertility rates. Consequently, this has led to increasing use of private health facilities, which require fees [3,4]. To obtain adequate healthcare, many households in Egypt rely on out-of-pocket financing which increases the risk of becoming impoverished if the out-of-pocket payments were substantial and for prolonged periods. Excessive reliance on out-of-pocket payments may increase inequalities in access to healthcare and could also increase intergenerational inequality if the households’ ability to invest in their children’s health and education is reduced [5,6]. Statistics show that out-of-pocket payments are the principle mean of financing healthcare in Egypt. According to the National Health Accounts, in 2008, out-of-pocket payments accounted for 60% of health spending. The seventh round of the Egyptian Family Observatory Survey revealed that 80% of households have at least one member covered by public health insurance. However, the survey pointed out that only 25% of the insured households are benefiting from it due to low quality services and excessive red tape. This suggests that health shocks may push non-poor into poverty and exacerbate the poverty of the poor [7].
To the best of our knowledge, this study is among the first to assess the distribution of government health sector subsidies across economic classes in Egypt. To evaluate whether public health spending is pro-poor or pro-rich, the study uses Benefit Incidence Analysis (BIA) [8,9,10]. BIA is a commonly used accounting procedure that helps determine who gets how much of the amount the government spends providing healthcare to the population.
The paper is organized as follows: Section 2 presents a brief review of the related literature. Section 3 provides an overview on the structure of the healthcare system in Egypt. The data is described in Section 4, and the empirical methodology is presented in Section 5. Empirical results are discussed in Section 6. Section 7 summarizes the findings of the paper and discusses some policy recommendations. Section 8 concludes the paper.
2. Literature Review
Health shocks could increase households’ vulnerability and disrupt their livelihood. To make healthcare services affordable, many countries adopt a subsidized universal healthcare system with the pre-assumption that the poor are the ones who benefit the most. The importance of an equitable distribution of the benefits from public healthcare subsidies stems from the fact that with no adequate access of healthcare services, vulnerable households may resort to out-of-pocket payments which increases the risk of becoming impoverished if the payments were substantial and for prolonged periods1. In a cross country study of 11 Asian countries, Van Doorslaer et al. [11] examined whether out-of-pocket healthcare payments exacerbate poverty. They found that poverty estimates after accounting for the out-of-pocket healthcare payments were much higher than the conventional estimates, ranging from an additional 1.2% of the population in Vietnam to 3.8% in Bangladesh. In a recent study, Rashad and Sharaf [12] found empirical evidence that out-of-pocket health expenditures pushed 6% of the Egyptian households to encounter financial catastrophe, and 7.4% of the households fell below the poverty line after controlling for healthcare expenditures. They also found that rural households are more likely to incur catastrophic health expenditure when compared to urban households.
Several studies have examined the distribution of benefits from public healthcare subsidies in a wide range of countries with mixed findings2. For example, in a cross-country study, O’Donnell et al. [8] reported substantial variation, across 11 Asian countries, in the incidence of public healthcare subsidies. The study revealed that public health subsidy is strongly pro-poor in Hong Kong, moderately pro-poor in Malaysia and Thailand, evenly distributed in Sri Lanka, while it is mildly pro-rich in Vietnam. In the remainder of the low-income countries and provinces examined, the better-off receive substantially more of the subsidy than do the poor. In another cross-country study of 69 countries, Wagstaff et al. [14] estimated the pro-poorness of government health expenditure at different income levels. They found that on average, government health expenditures are pro-rich. At the country level, in the majority of countries, government health expenditure is neither pro-rich nor pro-poor, while in a small minority it is pro-rich, and in an even smaller minority it is pro-poor. In addition, government health spending on contracted private facilities are pro-rich for all types of care, and in almost all Asian countries government health spending overall is significantly pro-rich. Moreover, they found that at the country level, the pro-poorness of government health spending is positively correlated with per-capita GDP, per-capita government health spending, and with six measures of the quality of a country’s governance, while negatively correlated with the share of government facility revenues coming from user fees.
In addition to cross country studies, a growing number of country-specific studies have examined the distribution and equity aspects of public healthcare subsidies in a wide range of countries, during different periods, and using different estimation techniques with similarly mixed findings (e.g., [6,15,16,17,18]). For instance, Akazili et al. [15] conducted an assessment of the financing and benefit incidence of health services in Ghana and found that the healthcare financing system is progressive, while the distribution of total benefits from both public and private health services is pro-rich. However, public sector district-level hospital inpatient care is pro-poor and benefits of primary-level healthcare services are relatively evenly distributed. The study also reported a number of access constraints which contribute to inequities in the distribution of health service benefits in Ghana.
In another study, Limwattananon et al. [17] found that public subsidies to healthcare, both outpatient (OP) and inpatient (IP) services to public hospitals and health facilities, in Thailand was pro-poor between 2003 and 2009, which preferentially benefited the poorer quintiles. Burger et al. [16] investigated whether public health spending and access to healthcare services in South Africa have become more or less pro-poor over time. They found that public health spending became more pro-poor between 1993 and 2008, with an increase in the share of public clinic and hospital spending going to the poor. In addition, there were improvements in both financial and physical access to public health services which significantly helped poor households who are more frequent users of public hospitals and clinics than those who are more affluent. Onwujekwe et al. [9] found evidence that although coverage of priority public health services were well below target levels in Nigeria, the poorer quintiles and rural residents that are in greater need received more net benefits from provision of these health services.
Using BIA, Anselmi et al. [19] assessed horizontal and vertical equity in the geographic allocation of recurrent expenditure for outpatient healthcare across districts in Mozambique between 2008 and 2011. They found a pro-rich distribution of government spending, driven by pro-rich service utilization. Though an improvement towards horizontal and vertical equity, in both government and donor expenditure, took place between 2008 and 2011, inequities in the distribution of expenditure across beneficiaries persisted and were driven by inequities in service use.
In a recent study, Chen et al. [18] examined how the benefits from government healthcare subsidies in China are distributed. Using a BIA, they found an inequitable distribution of government healthcare subsidies during the period 2002 to 2007, where high-income individuals generally reap larger benefits from the subsidized healthcare system. Although greater healthcare subsidies were concentrated among the rich and did not demonstrate inequality-reducing effects in different regions over the studied years, some policy reforms along with the decrease in out-of pocket-payments and the rising allocation of government healthcare resources to healthcare facilities widened access and improved the opportunity to receive healthcare benefits all of which reduced inequity.
This paper contributes to the extant literature by providing empirical evidence on the distribution of public healthcare subsidies by focusing on the specific case of Egypt on which limited research has been conducted. To our knowledge, only one related study has investigated the distributional aspect of public health care expenditure in Egypt. In an earlier study, Rannan-Eliya et al. [20], combined data from the national health accounts, and micro data from the National Household Health Utilization and Expenditure Survey conducted in 1994, to examine the degree of inequality in the distribution of health expenditures in Egypt. The incidence of overall health expenditures in Egypt was found to be progressive. They concluded that the social insurance programs in Egypt, and the use of cost recovery in some public sector institutions contributed to greater inequality in the access to health care resources, both when evaluated by the level of income, and gender. The 1994–1995 expansion of social health insurance coverage to children has not improved the distribution of health care spending in favor of lower income households. The current study extends the earlier study of Rannan-Eliya et al. [20] by using an up to data from the Egyptian Demographic and Health Survey (EDHS), and using a BIA.
In the next section, we will shed the light on the structure of the healthcare system in Egypt.
3. Structure of the Healthcare System in Egypt
Egypt has a highly pluralistic healthcare system, with several different public and private providers and financing agents [3]. Public health providers include the Ministry of Health and Population (MOHP) and other organizations that receive budgetary support from the government general revenues. The MOHP operates a large network of health facilities that offer comprehensive healthcare to all Egyptians at highly subsidized rates. It owns more than 441 hospitals and 4839 primary healthcare centers. Eighty percent of MOHP’s services are free and the rest requires some user fees. In addition to out of pocket payments and donations, the vast majority of MOHP funding comes from the Ministry of Finance. University hospitals are important health providers that provide primary, secondary, and tertiary treatment. They are autonomous facilities affiliated to individual universities and fall under the responsibility of the Ministry of Higher Education. The number of University Hospitals is 76 hospitals in 2008. Funding to University hospitals comes mainly from the Ministry of Finance through the Ministry of Higher Education and 30% comes from user fees. They are highly concentrated in Cairo and urban areas.
In addition to MOHP and University hospitals, Teaching Hospitals and Institutes Organization (THIO), Curative Care Organization (CCO) and the Health Insurance Organization are additional key healthcare providers. They are quasi-governmental organizations. Teaching Hospitals and Institutes Organization runs 11 general teaching hospitals and 20 research institutes which provides primary, secondary, and tertiary services. Half of the THIO’s services are free of charge, and it serves a small proportion of the population due to its small size. It receives funding from the Ministry of Finance, MOHP and private firms through contracts, international donors through grants, the Health Insurance Organization through contracts and direct user fees. CCO is a non-profit organization under the authority of MOHP. It operates 11 urban hospitals that provide a comprehensive range of curative care services mainly to urban residents. It does not receive any subsidy from the Government, and hence it relies on 100% cost recovery. The Health Insurance Organization is an independent public organization under the authority of the MOHP. It provides compulsory insurance to formal sector workers, widows and pensioners, school children and newborns. It is funded mainly from insurance premiums and co-payments, and it covers 55% of the population. However, less than half of the insured are really benefiting from the insurance scheme [21].
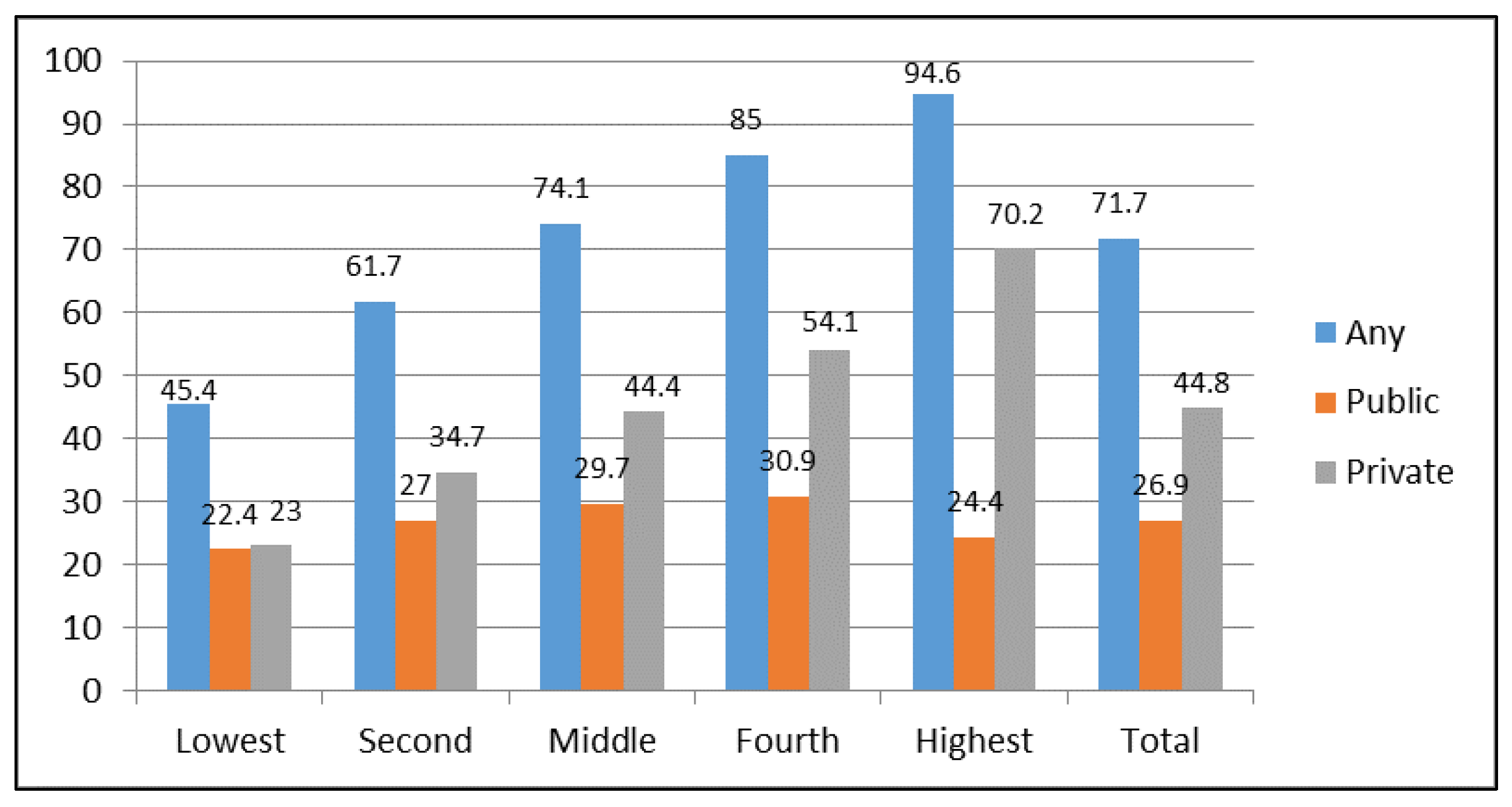
Figure 1 depicts the percentage of delivery in a Health Facility by wealth quintiles in 2008. As evident from the figure, there are large disparities in healthcare utilization across wealth quintiles. For example, women in the richest quintile are more than twice as likely as women in the poorest quintile to deliver in a health facility. Based on a survey, 70 percent of poor households mentioned financial cost as a significant impediment to healthcare [2].
Figure 1.
Delivery in a health facility by wealth quintiles in 2008. Source: Egypt Demographic and Health Survey [22].
Figure 1.
Delivery in a health facility by wealth quintiles in 2008. Source: Egypt Demographic and Health Survey [22].

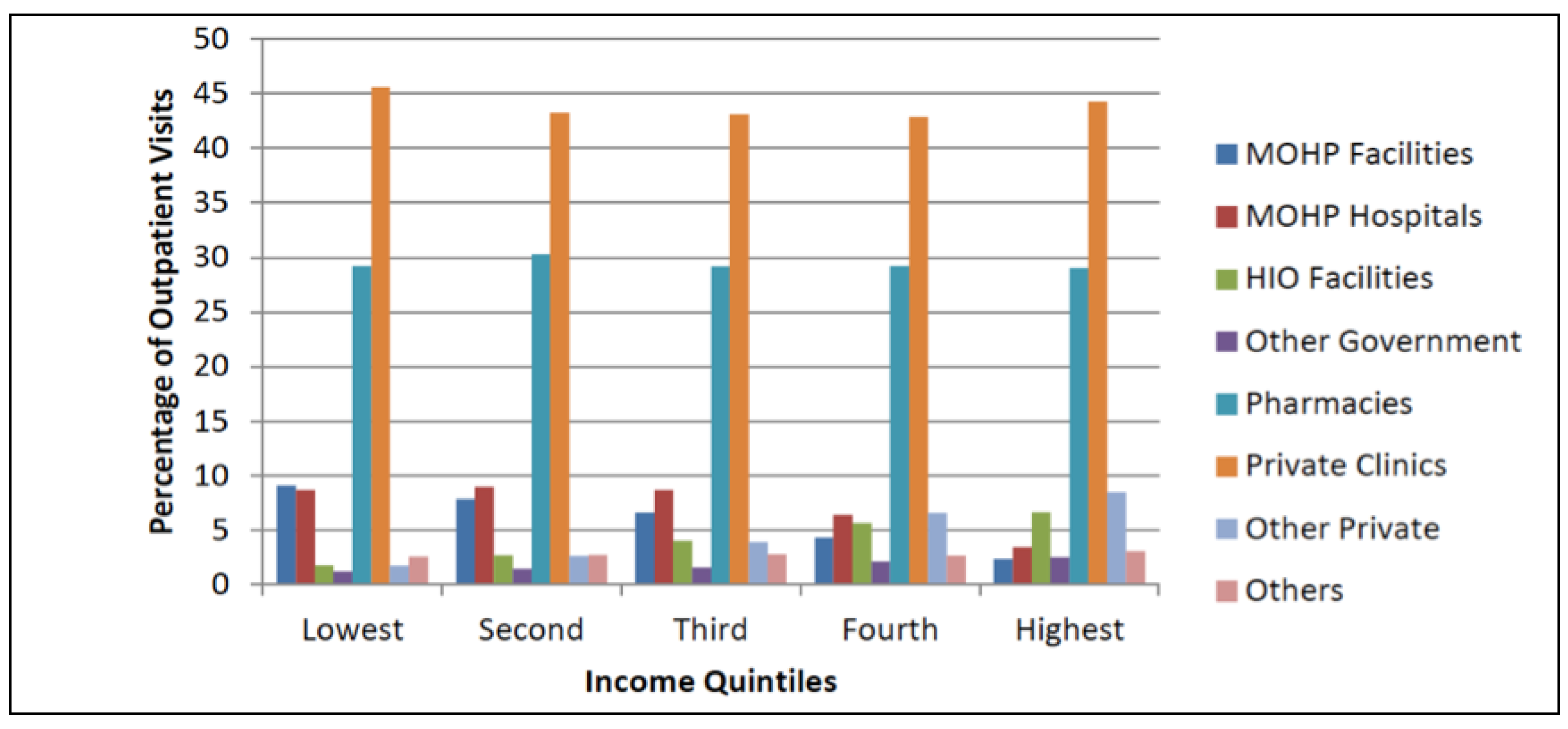
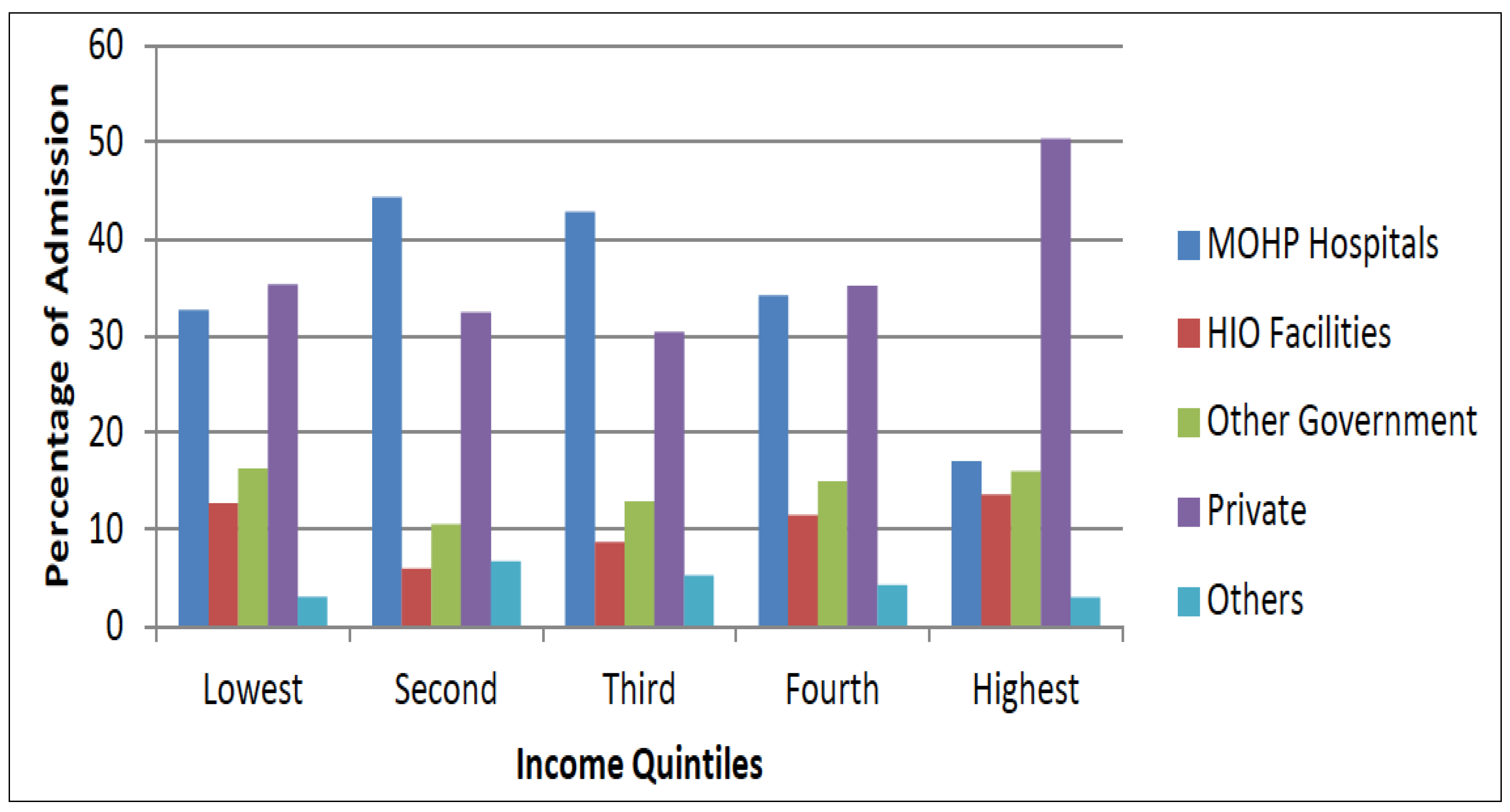
Despite subsidization, statistics show that the utilization of MOHP outpatient facilities is very low. The most striking fact about the choice of a healthcare provider is the high use of private healthcare among the poor. Figure 2 displays the choice of a provider for outpatient care by income quintiles. The private sector dominates the provision of outpatient care even among the poor. For households in the poorest quintile, 15% of all outpatient visits occurred in MOHP outpatient facilities, while 70% occurred in the private sector. The utilization of MOHP outpatient facilities steadily decreases with income. A similar pattern is observed for inpatient care (Figure 3). The utilization of MOHP inpatient facilities is more frequent than MOHP outpatient facilities, which is likely due to the high fees associated with inpatient care at private facilities. Private sector is the preferred provider for inpatient care for the wealthiest quintile and even for the insured patients if they can afford it.
Figure 2.
Choice of outpatient care provider by income quintile. Source: Egypt National Health Accounts [23].
Figure 2.
Choice of outpatient care provider by income quintile. Source: Egypt National Health Accounts [23].

Figure 3.
Inpatient care provider by income quintile. Source: Egypt National Health Accounts [23].
Figure 3.
Inpatient care provider by income quintile. Source: Egypt National Health Accounts [23].

It is difficult to run a BIA using data on quasi-governmental organizations, as they raise funds from several sources, and it is not possible to identify the subsidized patients from the non-subsidized ones. Consequently, in this study, BIA is limited to public health providers, both MOHP and University hospital, as both mainly get funding from the general tax revenue, and both constitute the biggest public health providers in Egypt in terms of coverage.
Private for-profit-health providers and other non-profit organizations that are not subsidized from the government revenue are not taken into account. Three categories of healthcare services are explored in the BIA: ambulatory visits to MOHP, hospital stays in MOHP, and hospital stays in University Hospitals.
4. Data
The main data set of this paper is the Egyptian Demographic and Health Survey (EDHS). The EDHS is a micro data survey implemented in 2008 and covers a nationally representative sample of 12,008 individuals. The survey collects a wide range of vital information on health related behavior, as well as corresponding economic and socio-demographic variables. Of particular importance, the EDHS includes information on outpatient visits to healthcare providers, hospital stays, and health expense incurred [22]. The survey distinguishes between public and private care and collects information on the level of household ownership, which is used to construct a measure of living standard based on the principal component analysis.
To conduct a BIA, we need the amount of public spending on each type of healthcare service for which utilization data are available on the survey. Data on public spending on healthcare are computed from the Egyptian National Health Accounts [23] (Table 1)3.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Health Provider | Public Expenditure | Out of Pocket Payments | Unit Cost |
|---|---|---|---|
| MOHP Hospitals | 3,819,458,728,00 | 288,049,928,00 | 281 |
| University Hospitals | 2,638,095,984,00 | 294,610,573,00 | 536 |
| Outpatient care | 2,180,591,664,00 | 527,439,388,00 | 60 |
Source: Egyptian National Health Accounts [23].
Conducting the BIA requires a health survey that has information on the utilization of the entire population of all types of healthcare, and all types of health facilities. In general, the standard Demographic and Health Survey (DHS) questionnaire cannot be used in conducting a BIA, as it does not gather enough information on health care utilization, or on the expenses incurred as it is too partial [24]. However, EDHS for the year 2008, has a special feature that makes it unique. It collects information on different types of health care utilization prior to the interview and on expenses households may have incurred for health services [22]. Consequently, the paper has greatly benefited from this exceptional round, and performed the BIA for Egypt using this special round. Given what has been stated, it would be obvious now why the current study has used the EDHS round for the year 2008, instead of using the most recent round of 2014.
5. Methodology: Benefit Incidence Analysis
To determine whether public healthcare spending in Egypt is pro-poor or pro-rich, we use the BIA4. The BIA is a commonly used accounting procedure, which helps determine the share of the different recipients in the healthcare expenditure provided by the government.
The first step of the BIA is estimation of the service-specific subsidy received by a patient which is calculated as in Equation (1).
where is the quantity of health service utilized by patient is the fee paid for service by patient . is the cost per unit of health service at region . Unit cost is calculated by dividing total spending on service by the weighted quantity of utilization provided in the survey as in Equation (2).
where and are the sum of government subsidies and out of pocket payments on service respectively divided by the aggregate utilization .
The total amount of the subsidy received by patient is calculated as in Equation (3).
standardizes the recall period across different types of healthcare services. It is an equal one if the recall period is one year and equals 13 for a four-week recall period.
After estimating the total amount of the subsidy received by each individual in the sample, the next step is to examine the distribution of the subsidy across the different income quintiles. A concentration index is used to determine whether the subsidization of healthcare is pro-poor or pro-rich. The concentration index (CI) is a quantification of the degree of economic related inequality in the variable of interest. A positive CI indicates pro-rich distribution of subsidies, and a negative CI reflects pro-poor distribution. The higher the absolute value of the CI, the greater is the degree of concentration of subsidies among the economic group. CI of subsidies could get more pro-poor either due to low utilization of public health facilities by the rich or higher concentration of user fees among the rich. The CI is calculated as in Equation (4):
In Equation (4), is the amount of the subsidy received by individual and is its mean, while is a measure of living standard. The concentration index depends on the covariance between the amount of the subsidy received and its association with the measure of living standard. In addition to the CI, the concentration curve is used to illustrate the share of subsidies received by cumulative proportions of individuals in the population across the income distribution.
The CI and the concentration curve are powerful tools for assessing the distribution of health sector subsidies. However, visual inspection of concentration curve is not sufficient to conclude whether the subsidies are pro-poor or pro-rich. A formal test of statistical dominance is necessary to definitively conclude whether health sector subsidies benefit the poor more or not. According to the concentration curve dominance test, the concentration curve for outpatient care is statistically pro-poor if at least one quintile point at which the concentration curve for outpatient care lies significantly above the 45 degree line, and there is no quintile point at which the 45 degree line lies above the concentration curve [8].
In addition to the concentration curve dominance test, Kakwani’s progressivity index is also used as a robustness check. This index evaluates whether the health sector subsidies reduce inequality (weak progressivity) by comparing income distribution to subsidies’ distribution. It is equal to the difference between the subsidies concentration index and the Gini index, and it ranges between −2 and 1. Data for the Gini coefficient and income shares are obtained from the World Development Indicators issued by the World Bank. All analyses and estimations are population weighted using the sampling weights provided in the survey.
6. Results
Table 2 reports the average subsidy received by each wealth quintile for inpatient admission at University hospitals, outpatient visit to MOHP, and hospital stays at MOHP, respectively. The table also displays the share of each wealth quintile in the public subsidies in relative terms, as well as results of the different tests of dominance.
Results show that subsidies for University hospitals increase with wealth level. The fourth wealth quintile is benefiting six times higher than the poorest wealth quintile. On the contrary, public subsidies for ambulatory care in MOHP and inpatient care in MOHP hospitals are inversely related to wealth level.
Households at the poorest wealth quintile receive 40% of the public subsidies associated with ambulatory care, while households at the richest quintile receive 16% of these subsidies. A similar pattern is observed for inpatient care at MOHP hospitals. For University hospitals, the poorest quintile receives only 11% of the public subsidies, while the fourth quintile alone receives 67% of the subsidies.
| Income | University Hospitals | MOHP Outpatient | MOHP Inpatient | Total Subsidies | |
|---|---|---|---|---|---|
| Mean subsidy | |||||
| Lowest quintile | 5153 | 20.05 | 35.94 | 103.81 | 159.60 |
| (20.05) | (5.58) | (38.82) | (43.97) | ||
| Poorest 40% | 7216 | 5.95 | 34.22 | 52.32 | 92.33 |
| (5.95) | (4.42) | (23.99) | (25.51) | ||
| Poorest 60% | 9086 | 12.28 | 32.06 | 44.64 | 88.91 |
| (7.60) | (4.23) | (20.41) | (22.55) | ||
| Poorest 80% | 11,687 | 121.09 | 22.14 | 16.61 | 159.75 |
| (69.35) | (3.57) | (12.38) | (70.50) | ||
| Highest quintile | 22,341 | 19.77 | 24.23 | 42.09 | 86.01 |
| (19.77) | (4.81) | (20.54) | (28.98) | ||
| Total | 11,192 | 35.82 | 29.72 | 51.87 | 117.30 |
| (15.10) | (2.04) | (11.09) | (18.87) | ||
| Shares (%) | |||||
| Lowest quintile | 9.3 | 11.2 | 24.1 | 40 | 27.2 |
| (10.92) | (3.19) | (10.86) | (6.70) | ||
| Poorest 40% | 13 | 3.3 | 23.0 | 20.2 | 15.8 |
| (3.50) | (2.73) | (8.36) | (4.41) | ||
| Poorest 60% | 16.4 | 6.9 | 21.6 | 17.2 | 15.2 |
| (4.89) | (2.64) | (7.36) | (4.04) | ||
| Poorest 80% | 21 | 67.6 | 14.9 | 6.4 | 27.2 |
| (16.84) | (2.28) | (4.66) | (9.23) | ||
| Highest quintile | 40.3 | 11.0 | 16.3 | 16.2 | 14.7 |
| (10.81) | (2.90) | (7.39) | (4.79) | ||
| Total | 100 | 100 | 100 | 100 | 100 |
| Test of Dominance | |||||
| Against 45 degree line | None | None | None | None | |
| Against Income distribution | None | D − | D + | D+ | |
| Concentration Index | 0.3182 | −0.1051 | −0.2168 | −0.0252 | |
| (0.15) | (0.04) | (0.12) | (0.09) | ||
| Kakwani Index | 0.1 | −0.309 | −0.51 | −0.31 |
Note: Total refers to overall subsidies, standard errors are in parenthesis. None indicates that the concentration curve is indistinguishable from the 45 degree line or Lorenz curve. D− and D+ indicate that the concentration curve is significantly distinguishable from the compared distribution.
Table 2 shows a positive CI for University hospitals, which suggests that subsidies associated with University hospitals are strongly concentrated among the rich. This result was further confirmed by the positive sign of the Kakwani index for inpatient admission at University hospitals. This indicates that subsidies associated with hospital care at University hospitals increased the income gap between the rich and the poor.
On the other hand, the concentration indices for outpatient visits and inpatient care at MOHP are both negative, indicating that the public subsidies for these healthcare services are pro-poor. Overall, health sector subsidies seem slightly pro-poor, as the CI of total subsidies is almost equal to zero. Results of the Kakwani indices for outpatient visits and inpatient care at MOHP are both negative, which are in line with the results of the CI. This indicates that subsidies associated with the MOHP, for outpatient and inpatient visits, reduce the income gap between the poor and the rich.
Results of the dominance tests, conducted to investigate whether health sector subsidies are significantly pro-poor at the 5% significance level, fail to reject the null hypothesis that the concentration curves are indistinguishable from the line of equality. This indicates that public healthcare subsidies are not pro-poor. However, testing the concentration curves against the income distribution shows that the concentration curves for outpatient and inpatient care at the MOHP dominate the income distribution curve. This suggests that subsidies associated with the MOHP are inequality-reducing (weakly progressive).
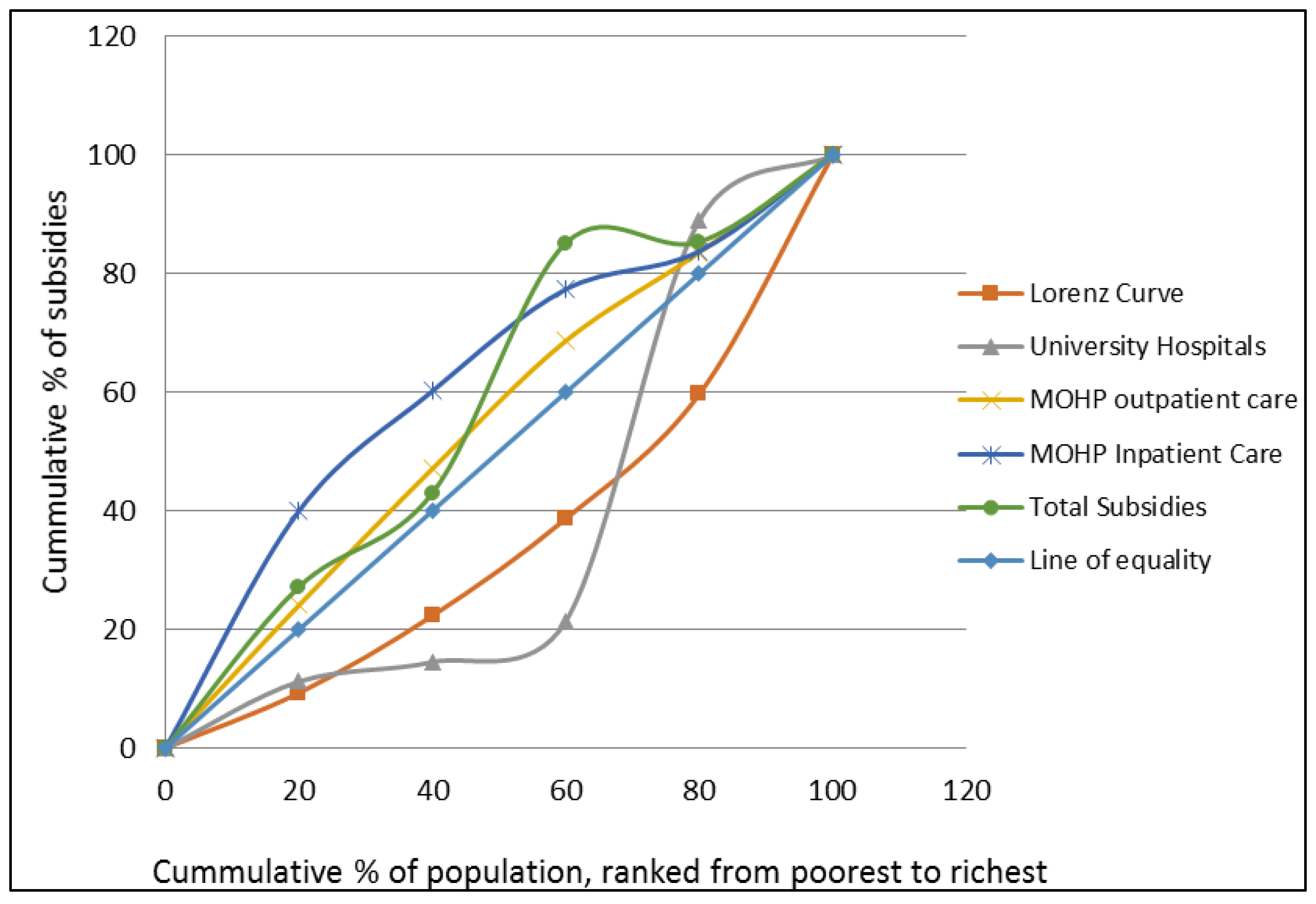
Figure 4 depicts the concentration curves for health sector subsidies and shows that the concentration curves for outpatient and inpatient care at MOHP are lying above the line of equality, which means that the poor benefits more from public subsidies than the rich. In contrast, the concentration curve for university hospitals lies below the line of equality, which indicates that the rich households benefit more from the public subsidies for university hospitals. The concentration curve for total public healthcare subsidies is slightly above the 45 degree line for the first two quintiles and, as we move farther, it is almost on the top of the 45 degree line.
Figure 4.
Concentration curves for health sector subsidies.

7. Discussion and Policy Implications
Egypt has been adopting a subsidized healthcare system for decades. This paper examined whether public healthcare subsidies in Egypt are pro-poor or pro-rich. Results show that public subsidies to healthcare services in Egypt are not pro-poor, meaning that subsidies tend to benefit wealthier groups more than the poorer groups. Under less restrictive assumption, in which the distribution of subsidies is compared to income distribution, the BIA showed that subsidies associated with the MOHP have inequality-reducing effect (weakly progressive). University hospitals’ subsidies are mainly benefiting the rich and did not contribute to closing the income gap.
Previous studies have documented a number of access constraints which contribute to inequities in the distribution of health service benefits. These include long queues, long waiting hours, and inadequate staff and equipment in healthcare facilities especially in rural areas [15,25,26].
Geographical access is a major challenge, particularly for rural populations. This could explain why subsidies associated with University hospitals in Egypt are pro-rich. The poor are more likely to live in rural communities, while University hospitals are in urban areas. In addition, University hospitals require some sort of user fees and the poor are most affected by high user fees. This implies that user fees would reduce access to health-care more for the poor than for the better off. Therefore, the burden of user fees and transportation costs could be among the primary reasons for the inequitable distribution of the University hospitals’ subsidies in Egypt. Red tape and long waiting lists for many healthcare services especially surgeries, medical exams and hospitalization have also been reported as major access barriers by the poor. The seventh round of the Egyptian Family Observatory Survey revealed that only 25% of households who are covered by public health insurance are benefiting from it due to low quality services and excessive red tape. Statistics from Egypt National Health Accounts show that in 2008, only 8.1% and 21% of the insured individuals use Health Insurance Organization (HIO) facilities for outpatient and inpatient healthcare. Insured individuals reported several reasons for not using HIO facilities: distance was cited by 18% of the individuals, 35 percent cited the long waiting time, and 44 percent cited lower-quality services [23].
To ensure an equitable distribution of health service benefits, poverty reduction policies should tackle the access constraints that affect the distribution of benefits. One policy measure for improving the distribution of subsidies is targeting health subsidies more toward illness associated with poverty. For instances, poor housing, poor nutrition, and lack of sanitation are associated with certain types of diseases. The government could link subsidies to these types of diseases. We recommend re-engineering the allocation of health sector subsidies toward healthcare services and facilities that are mostly used by the poor households. Another policy option is reducing the user fees associated with University hospitals, especially for the poor, and redirecting subsidies from University hospitals to MOHP facilities, which are the main source of healthcare services for the poor and rural residents.
Addressing the problems associated with the HIO facilities, and improving the quality of the provided services could also be an essential step to achieve an equitable distribution of public healthcare subsidies and increase the usage of HIO facilities. This has to be supplemented with improved focus on primary care and immunization, especially in rural and remote communities, in which the Non-Governmental Organizations (NGOs) and the private sector could play a vital role. In a review of the contracting experiences in 10 low-income countries, Loevinsohn and Harding [27] found that contracting with NGOs and the private sector to deliver healthcare or nutrition services was in general effective. Contractors, both NGOs and private healthcare providers, are more efficient than government agencies in terms of quality and coverage of the provided healthcare services and were more cost-effective. There is substantial empirical evidence that contracting increases accessibility, utilization level and coverage of healthcare services [28]. Levin and Kaddar [29] conducted a literature review on the role of the private sector in the provision of immunization services in low-and middle-income countries. They found that in low-income countries, the private for-profit sector is contributing to immunization service delivery and helping to extend access to traditional vaccines. In middle-income countries, the private for-profit sector facilitates early adopted new vaccines and technologies before introduction and generalization by the public sector. They also found that the not-for-profit sector plays an important role in extending access to traditional Expanded Program on Immunization (EPI) vaccines in low-income countries especially in rural and remote areas.
The current study has some limitations that warrant acknowledgment. First, the cross sectional nature of the used survey limits the ability to infer causality and to examine how the equity aspects of public subsidies evolve over time. The availability of longitudinal data in the future would stimulate further research to study the dynamics of the problem under investigation which will help design more effective policies to tackle it. Second, there could be other confounding factors that affect the benefit incidence of public health subsidies which we did not control for such as differences in geographical access to healthcare facilities, variations in the quality of healthcare services across communities, and patient satisfaction.
Poverty reduction measures and healthcare reforms in Egypt should not only focus on expanding the coverage but also on improving the equity of distribution of healthcare benefits.
8. Conclusions
We found robust evidence that in Egypt, public healthcare subsidies associated with University hospitals are pro-rich and have inequality increasing effect, while subsidies associated with outpatient and inpatient care provided by the MOHP have not been pro-poor but have inequality reducing effect (weakly progressive). While it is widely perceived that the poor benefit the most from the health subsidies, the findings of this study refute this hypothesis in the case of Egypt. Poverty reduction measures and healthcare reforms in Egypt should not only focus on expanding the coverage of healthcare benefits but also on improving the equity of its distribution. Addressing the problems associated with HIO facilities, improving the quality of the provided services, and contracting with NGOs and the private sector to deliver healthcare or nutrition services, especially in rural and remote areas, could also be a promising policy option.
Acknowledgments
The authors would like to thank the two anonymous referees and the academic editor of this journal for the invaluable comments and suggestions which have substantially improved the manuscript.
Author Contributions
Both Authors contributed equally to the conceptualization, design and composition of the paper. Both authors read and approved the final manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. “Sustainable Health Financing, Universal Coverage and Social Health Insurance—Resolution WHA583. 33.” 2005. Available online: http://www.who.int/health_financing/documents/cov-wharesolution5833/en/ (accessed on 10 October 2014).
- Matteo Morgandi, Joana Silva, and Victoria Levin. Inclusion and Resilience: The Way Forward for Social Safety Nets in the Middle East and North Africa, Overview. Washington: World Bank, 2012. [Google Scholar]
- Fatma El-Zanaty, and Ann Way. “Egypt: DHS, 2005—Final Report.” February 2006. Available online: http://dhsprogram.com/publications/publication-fr176-dhs-final-reports.cfm (accessed on 20 November 2014).
- Lenka Benova, Oona M. R. Campbell, and George B. Ploubidis. “Socio-economic gradients in maternal and child health-seeking behaviours in Egypt: Systematic literature review and evidence synthesis.” PLoS ONE 9 (2014): e93032. [Google Scholar] [CrossRef] [PubMed]
- Ke Xu, David B. Evans, Guido Carrin, Ana Mylena Aguilar-Rivera, Philip Musgrove, and Timothy Evans. “Protecting households from catastrophic health spending.” Health Affairs 26 (2007): 972–83. [Google Scholar] [CrossRef] [PubMed]
- Khurshid Alam, and Ajay Mahal. “Economic impacts of health shocks on households in low and middle income countries: A review of the literature.” Global Health 10 (2014): 21. [Google Scholar] [CrossRef] [PubMed]
- Information and Decision Support Center. “Bank of Surveys: Eighth Round of the Egyptian Family Observatory Survey.” 2010. Available online: http://surveysbank.org.eg/Cod_Surveys/SurveyDetails_dtl.aspx?Survey_id=350 URL (accessed on 12 November 2012).
- Owen O’Donnell, Eddy van Doorslaer, Ravi P. Rannan-Eliya, Aparnaa Somanathan, Shiva Raj Adhikari, Deni Harbianto, Charu C. Garg, Piya Hanvoravongchai, Mohammed N. Huq, Anup Karan, and et al. “The incidence of public spending on healthcare: Comparative evidence from Asia.” The World Bank Economic Review 21 (2007): 93–123. [Google Scholar] [CrossRef]
- Obinna Onwujekwe, Kara Hanson, and Benjamin Uzochukwu. “Are the poor differentially benefiting from provision of priority public health services? A benefit incidence analysis in Nigeria.” International Journal for Equity in Health 11 (2012): 1–12. [Google Scholar] [CrossRef] [PubMed]
- Adam Wagstaff. “Benefit-incidence analysis: Are government health expenditures more pro-rich than we think? ” Health Economics 21 (2012): 351–66. [Google Scholar] [CrossRef] [PubMed]
- Eddy Van Doorslaer, Owen O’Donnell, Ravi P. Rannan-Eliya, Aparnaa Somanathan, Shiva Raj Adhikari, Charu C. Garg, Deni Harbianto, Alejandro N. Herrin, Mohammed Nazmul Huq, Shamsia Ibragimova, and et al. “Effect of payments for health care on poverty estimates in 11 countries in Asia: An analysis of household survey data.” The Lancet 368 (2006): 1357–64. [Google Scholar] [CrossRef]
- Ahmed Shoukry Rashad, and Mesbah Fathy Sharaf. “Catastrophic and Impoverishing Effects of Out-of-Pocket Health Expenditure: New Evidence from Egypt.” American Journal of Economics 5 (2015): 526–33. [Google Scholar]
- Laura Anselmi, Mylene Lagarde, and Kara Hanson. “Equity in the allocation of public sector financial resources in low-and middle-income countries: A systematic literature review.” Health Policy and Planning 30 (2014): czu034. [Google Scholar] [CrossRef] [PubMed]
- Adam Wagstaff, Marcel Bilger, Leander R. Buisman, and Caryn Bredenkamp. “Who benefits from government health spending and why? A global assessment.” 2014. Available online: http://papers.ssrn.com/sol3/Papers.cfm?abstract_id=2500586 (accessed on 10 February 2015).
- James Akazili, Bertha Garshong, Moses Aikins, John Gyapong, and Di McIntyre. “Progressivity of health care financing and incidence of service benefits in Ghana.” Health Policy and Planning 27 (2012): i13–22. [Google Scholar] [CrossRef] [PubMed]
- Ronelle Burger, Caryn Bredenkamp, Christelle Grobler, and Servaas van der Berg. “Have public health spending and access in South Africa become more equitable since the end of apartheid? ” Development Southern Africa 29 (2012): 681–703. [Google Scholar] [CrossRef]
- Supon Limwattananon, Viroj Tangcharoensathien, Kanjana Tisayaticom, Tawekiat Boonyapaisarncharoen, and Phusit Prakongsai. “Why has the Universal Coverage Scheme in Thailand achieved a pro-poor public subsidy for health care? ” BMC Public Health 12 (2012): S6. [Google Scholar] [CrossRef] [PubMed]
- Mingsheng Chen, Guixia Fang, Lidan Wang, Zhonghua Wang, Yuxin Zhao, and Lei Si. “Who Benefits from Government Healthcare Subsidies? An Assessment of the Equity of Healthcare Benefits Distribution in China.” PLoS ONE 10 (2015): e0119840. [Google Scholar] [CrossRef] [PubMed]
- Laura Anselmi, Mylène Lagarde, and Kara Hanson. “Going beyond horizontal equity: An analysis of health expenditure allocation across geographic areas in Mozambique.” Social Science & Medicine 130 (2015): 216–24. [Google Scholar] [CrossRef] [PubMed]
- Ravi P. Rannan-Eliya, Claudia Blanco-Vidal, and A. K. Nandakumar. The Distribution of Health Care Resources in Egypt: Implications for Equity. Boston: Harvard School of Public Health, 2000. [Google Scholar]
- Sherine Shawky. “Could the employment-based targeting approach serve Egypt in moving towards a social health insurance model? ” Eastern Mediterranean Health Journal 16 (2010): 663. [Google Scholar] [PubMed]
- Fatma El Zanaty, and Ann Way. “Egypt Demographic and Health Survey 2008.” 2009. Available online: http://dhsprogram.com/pubs/pdf/fr220/fr220.pdf (accessed on 5 December 2014).
- Sharon Nakhimovsky, Douglas Glandon, Nadwa Rafeh, and Nagwan Hassan. “Egypt National Health Accounts: 2008/09.” 2011. Available online: http://pdf.usaid.gov/pdf_docs/pnadz604.pdf (accessed on 10 September 2014).
- Di McIntyre, and John E. Ataguba. “How to do (or not to do)…a benefit incidence analysis.” Health Policy and Planning 26 (2011): 174–82. [Google Scholar] [CrossRef] [PubMed]
- Owen O’Donnell. “Access to health care in developing countries: Breaking down demand side barriers.” Cadernos de Saúde Pública 23 (2007): 2820–34. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. The World Health Report 2008: Primary Health Care Now More Than Ever. Geneva: World Health Organization, 2008. [Google Scholar]
- Benjamin Loevinsohn, and April Harding. “Buying results? Contracting for health service delivery in developing countries.” The Lancet 366 (2005): 676–81. [Google Scholar] [CrossRef]
- A. Venkat Raman, and James Warner Björkman. Public-Private Partnerships in Health Care in India: Lessons for Developing Countries. London: Routledge, 2008. [Google Scholar]
- Ann Levin, and Miloud Kaddar. “Role of the private sector in the provision of immunization services in low-and middle-income countries.” Health Policy and Planning 26 (2011): i4–12. [Google Scholar] [CrossRef] [PubMed]
- 1For a recent review of literature on the economic impacts of health shocks on households in low and middle income countries see Alam and Mahal [6].
- 2For a recent systematic review of the literature on the equity aspects in the distribution of public health sector expenditure in low- and middle-income countries see Anselmi et al. [13].
- 3Unit cost is assumed to be the same for a given type of service. Additionally, due to data limitations, variations in the quality of health care services across regions are not captured in the analysis.
- 4For a more technical discussion of the BIA and its associated assumptions see Wagstaff [10].
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Rashad, A.S.; Sharaf, M.F. Who Benefits from Public Healthcare Subsidies in Egypt? Soc. Sci. 2015, 4, 1162-1176. https://doi.org/10.3390/socsci4041162
AMA Style
Rashad AS, Sharaf MF. Who Benefits from Public Healthcare Subsidies in Egypt? Social Sciences. 2015; 4(4):1162-1176. https://doi.org/10.3390/socsci4041162
Chicago/Turabian StyleRashad, Ahmed Shoukry, and Mesbah Fathy Sharaf. 2015. "Who Benefits from Public Healthcare Subsidies in Egypt?" Social Sciences 4, no. 4: 1162-1176. https://doi.org/10.3390/socsci4041162