
Treatment of Chronic Migraine with Focus on Botulinum Neurotoxins

Abstract
:1. Introduction
2. Pathophysiology
3. Treatment
4. Botulinum Toxins (BoNTs): Animal Data
4.1. Peripheral Effects
4.2. Central Effects
5. Botulinum Toxin Treatment of Chronic Migraine
6. Comparator Studies of BoNTs vs. Oral Agents in Chronic Migraine
6.1. Botulinum Toxin vs. Divalproex Sodium
6.2. Botulinum Toxin vs. Topiramate
7. The Issue of Medication Overuse in Chronic Migraine
8. Long-Term Efficacy, Safety, and Effects on Quality of Life
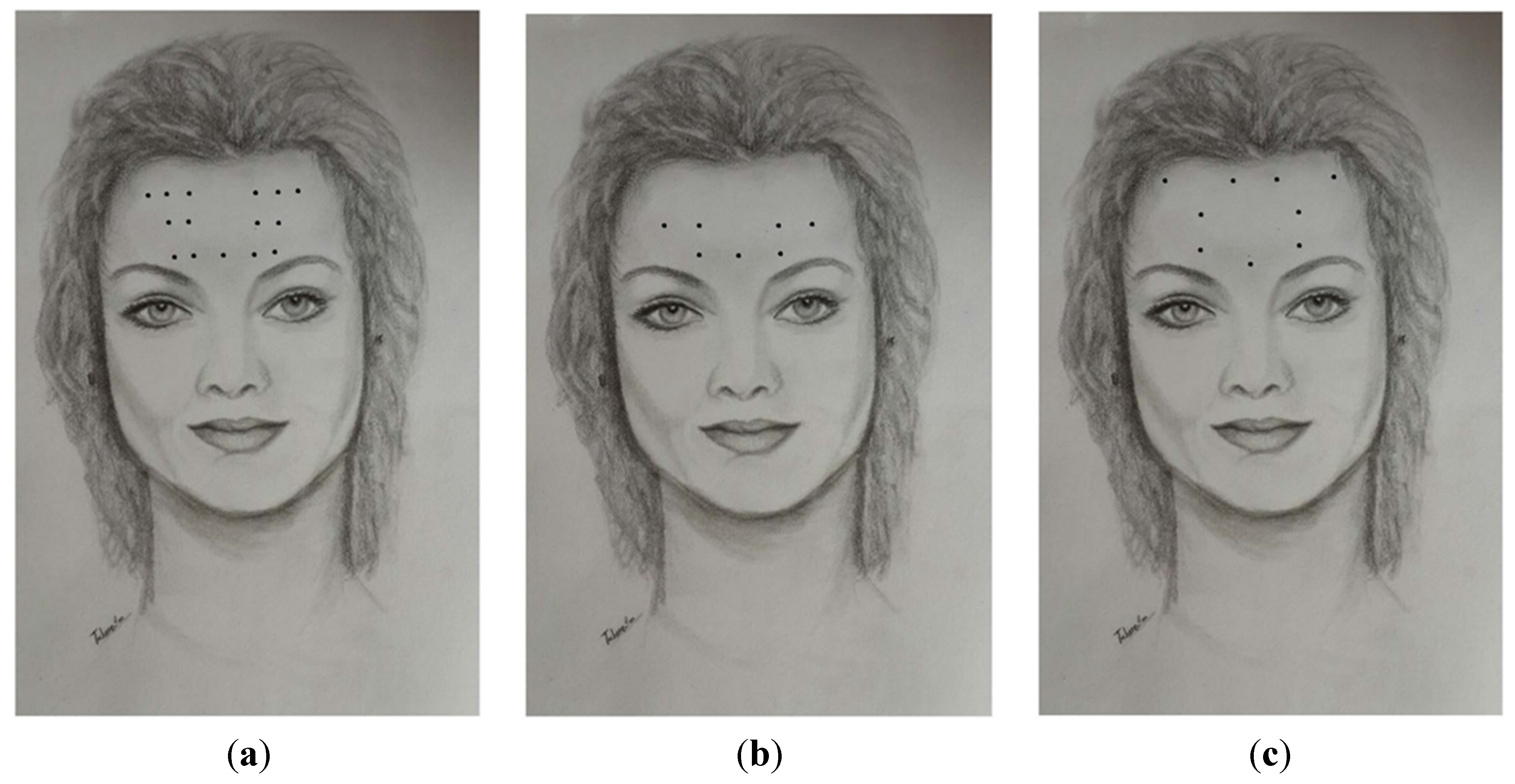
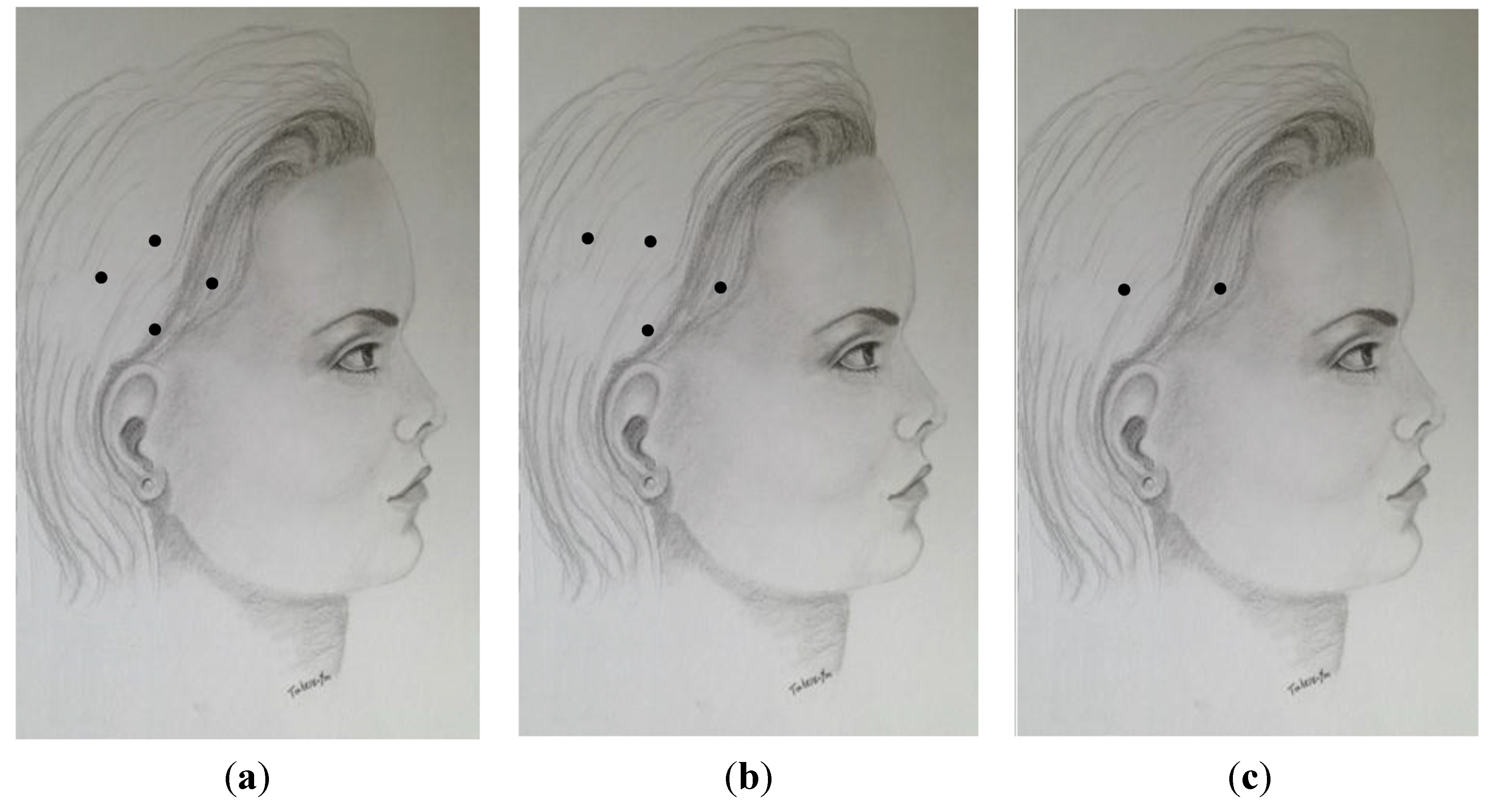
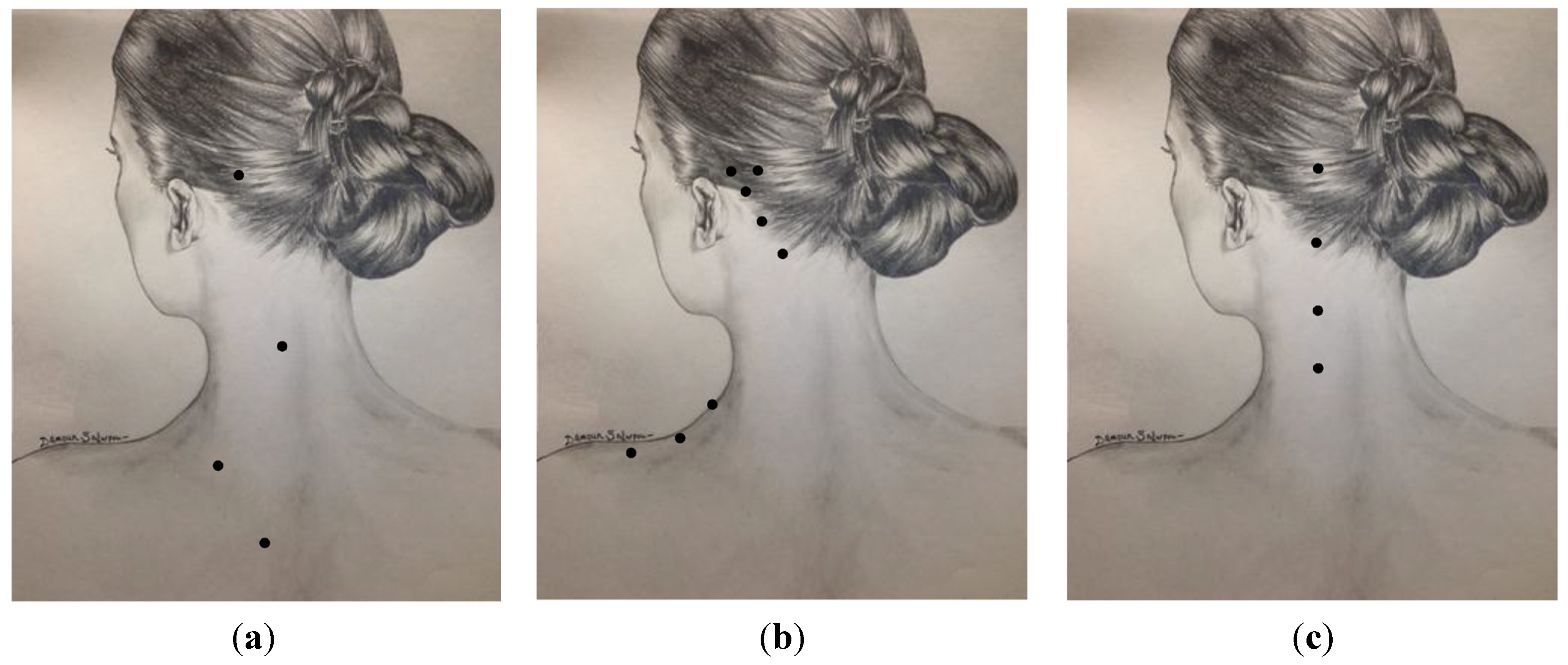
9. Techniques of Injection

{kind=link}
{kind=link}
{kind=link}
| Method | Procerus (Midline) | Corrugator | Frontalis | Temporalis | Occipitalis | Splenius/Paraspinalis | Trapezius | Masseter |
|---|---|---|---|---|---|---|---|---|
| Blumenfeld et al. 2003 [53]; Silberstein 2009 [54] (Figure 1a, Figure 2a and Figure 3a) | 2.5–5 u | 2.5 u × 2 | 2.5 u × 5 | 2.5–5 u × 4 | 2.5–5 u × 1 | 2.5–5 u × 1 | 2.5 u × 2 | 2.5–5 u × 1 |
| PREEMPT Blumenfeld 2010 [55] (Figure 1b, Figure 2b and Figure 3b) | 5 u | 5 u × 1 | 5 u × 2 | 5 u × 4 | 5 u × 3 | 5 u × 2 | 5 u × 3 | - |
| Jabbari (Yale) 2015 [56], (Figure 1c, Figure 2c and Figure 3c) * | 5 u | 5 u × 1 | 5 u × 3 | 15 u × 2 | 10 u × 1 | 10 u × 3 | - | - |



10. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- World Health Organization. The Global Burden of Disease: 2004 Update; WHO Press: Geneva, Switzerland, 2008; p. 31. [Google Scholar]
- Headache Classification Subcommittee of the International Headache Society. The international classification of headache disorders: 2nd ed. Cephalalgia 2004, 24 (Suppl. 1), 9–160. [Google Scholar]
- Lipton, R.B.; Bigal, M.E.; Diamond, M.; Freitag, F.; Reed, M.L.; Stewart, W.F.; AMPP Advisory Group. Migraine prevalence, disease burden, and the need for preventive therapy. Neurology 2007, 68, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Goldberg, L.D. The cost of migraine and its treatment. Am. J. Manag. Care 2005, 11, S62–S67. [Google Scholar] [PubMed]
- Ruggeri, M. The cost effectiveness of Botox in Italian patients with chronic migraine. Neurol. Sci. 2014, 35 (Suppl. 1), 45–47. [Google Scholar] [CrossRef] [PubMed]
- Cao, Y.; Welch, K.M.; Aurora, S.; Vikingstad, E.M. Functional mri-bold of visually triggered headache in patients with migraine. Arch. Neurol. 1999, 56, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Waeber, C.; Moskowitz, M.A. Therapeutic implications of central and peripheral neurologic mechanisms in migraine. Neurology 2003, 61, S9–S20. [Google Scholar] [CrossRef] [PubMed]
- Noseda, R.; Burstein, R. Migraine pathophysiology: Anatomy of the trigeminovascular pathway and associated neurological symptoms, csd, sensitization and modulation of pain. Pain 2013, 154 (Suppl. 1), S44–S53. [Google Scholar] [CrossRef] [PubMed]
- Benemei, S.; De Cesaris, F.; Fusi, C.; Rossi, E.; Lupi, C.; Geppetti, P. TRPA1 and other TRP channels in migraine. J. Headache Pain 2013, 14, 71. [Google Scholar] [CrossRef] [PubMed]
- Del Fiacco, M.; Quartu, M.; Boi, M.; Serra, M.P.; Melis, T.; Boccaletti, R.; Shevel, E.; Cianchetti, C. Trpv1, CGRP and SP in scalp arteries of patients suffering from chronic migraine. J. Neurol. Neurosurg. Psychiatry 2015, 86, 393–397. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Collins, B.; Jakubowski, M. Defeating migraine pain with triptans: A race against the development of cutaneous allodynia. Annals Neurol. 2004, 55, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Olesen, J.; Friberg, L.; Olsen, T.S.; Iversen, H.K.; Lassen, N.A.; Andersen, A.R.; Karle, A. Timing and topography of cerebral blood flow, aura, and headache during migraine attacks. Annals Neurol. 1990, 28, 791–798. [Google Scholar] [CrossRef] [PubMed]
- Ahn, A.H. On the temporal relationship between throbbing migraine pain and arterial pulse. Headache 2010, 50, 1507–1510. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D.; Dodick, D.W. Migraine genetics: Part ii. Headache 2013, 53, 1218–1229. [Google Scholar] [CrossRef] [PubMed]
- Cernuda-Morollon, E.; Larrosa, D.; Ramon, C.; Vega, J.; Martinez-Camblor, P.; Pascual, J. Interictal increase of cgrp levels in peripheral blood as a biomarker for chronic migraine. Neurology 2013, 81, 1191–1196. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D. Treatment recommendations for migraine. Nat. Clin. Pract. Neurol. 2008, 4, 482–489. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.C.; Holle, D.; Dodick, D. Treatment of chronic migraine. Curr. Pain Headache Rep. 2011, 15, 64–69. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, J.; Goadsby, P.J. Emerging targets in migraine. CNS Drugs 2014, 28, 11–17. [Google Scholar] [CrossRef] [PubMed]
- Gelfand, A.A.; Goadsby, P.J. A neurologist’s guide to acute migraine therapy in the emergency room. Neurohospitalist 2012, 2, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Ozkurt, B.; Cinar, O.; Cevik, E.; Acar, A.Y.; Arslan, D.; Eyi, E.Y.; Jay, L.; Yamanel, L.; Madsen, T. Efficacy of high-flow oxygen therapy in all types of headache: A prospective, randomized, placebo-controlled trial. Am. J. Emerg. Med. 2012, 30, 1760–1764. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D. Preventive treatment of migraine: An overview. Cephalalgia 1997, 17, 67–72. [Google Scholar] [CrossRef] [PubMed]
- Goadsby, P.J. Therapeutic prospects for migraine: Can paradise be regained? Annals Neurol. 2013, 74, 423–434. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Zhang, X.; Levy, D.; Aoki, K.R.; Brin, M.F. Selective inhibition of meningeal nociceptors by botulinum neurotoxin type a: Therapeutic implications for migraine and other pains. Cephalalgia 2014, 34, 853–869. [Google Scholar] [CrossRef] [PubMed]
- Meng, J.; Wang, J.; Lawrence, G.; Dolly, J.O. Synaptobrevin i mediates exocytosis of cgrp from sensory neurons and inhibition by botulinum toxins reflects their anti-nociceptive potential. J. Cell Sci. 2007, 120, 2864–2874. [Google Scholar] [CrossRef] [PubMed]
- Lucioni, A.; Bales, G.T.; Lotan, T.L.; McGehee, D.S.; Cook, S.P.; Rapp, D.E. Botulinum toxin type a inhibits sensory neuropeptide release in rat bladder models of acute injury and chronic inflammation. BJU Int. 2008, 101, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.R. Evidence for antinociceptive activity of botulinum toxin type a in pain management. Headache 2003, 43 (Suppl. 1), S9–S15. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Shibata, M.; Toriumi, H.; Iwashita, T.; Funakubo, M.; Sato, H.; Kuroi, T.; Ebine, T.; Koizumi, K.; Suzuki, N. Reduction of trpv1 expression in the trigeminal system by botulinum neurotoxin type-a. Neurobiol. Dis. 2012, 48, 367–378. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, G.W.; Aoki, K.R.; Dolly, J.O. Excitatory cholinergic and purinergic signaling in bladder are equally susceptible to botulinum neurotoxin a consistent with co-release of transmitters from efferent fibers. J. Pharmacol. Exp. Ther. 2010, 334, 1080–1086. [Google Scholar] [CrossRef] [PubMed]
- Cui, M.; Khanijou, S.; Rubino, J.; Aoki, K.R. Subcutaneous administration of botulinum toxin a reduces formalin-induced pain. Pain 2004, 107, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Namazi, H. Intravesical botulinum toxin a injections plus hydrodistension can reduce nerve growth factor production and control bladder pain in interstitial cystitis: A molecular mechanism. Urology 2008, 72, 463–464. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.C.; Yoshimura, N.; Huang, C.C.; Wu, M.; Chiang, P.H.; Chancellor, M.B. Intraprostatic botulinum toxin a injection inhibits cyclooxygenase-2 expression and suppresses prostatic pain on capsaicin induced prostatitis model in rat. J. Urol. 2008, 180, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Luvisetto, S.; Vacca, V.; Cianchetti, C. Analgesic effects of botulinum neurotoxin type a in a model of allyl isothiocyanate- and capsaicin-induced pain in mice. Toxicon 2015, 94, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.C.; Wakita, M.; Xie, D.J.; Yamaga, T.; Iwata, S.; Torii, Y.; Harakawa, T.; Ginnaga, A.; Kozaki, S.; Akaike, N. Inhibition of membrane na+ channels by a type botulinum toxin at femtomolar concentrations in central and peripheral neurons. J. Pharmacol. Sci. 2012, 118, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Rand, M.J.; Whaler, B.C. Impairment of sympathetic transmission by botulinum toxin. Nature 1965, 206, 588–591. [Google Scholar] [CrossRef] [PubMed]
- Filippi, G.M.; Errico, P.; Santarelli, R.; Bagolini, B.; Manni, E. Botulinum a toxin effects on rat jaw muscle spindles. Acta Otolaryngol. 1993, 113, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Bach-Rojecky, L.; Salkovic-Petrisic, M.; Lackovic, Z. Botulinum toxin type a reduces pain supersensitivity in experimental diabetic neuropathy: Bilateral effect after unilateral injection. Eur. J. Pharmacol. 2010, 633, 10–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matak, I.; Bach-Rojecky, L.; Filipovic, B.; Lackovic, Z. Behavioral and immunohistochemical evidence for central antinociceptive activity of botulinum toxin A. Neuroscience 2011, 186, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matak, I.; Riederer, P.; Lackovic, Z. Botulinum toxin’s axonal transport from periphery to the spinal cord. Neurochem. Int. 2012, 61, 236–239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinelli, S.; Vacca, V.; Ricordy, R.; Uggenti, C.; Tata, A.M.; Luvisetto, S.; Pavone, F. The analgesic effect on neuropathic pain of retrogradely transported botulinum neurotoxin a involves schwann cells and astrocytes. PLoS ONE 2012, 7, e47977. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.; Mathew, N.; Saper, J.; Jenkins, S. Botulinum toxin type a as a migraine preventive treatment. For the botox migraine clinical research group. Headache 2000, 40, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Naumann, M.; So, Y.; Argoff, C.E.; Childers, M.K.; Dykstra, D.D.; Gronseth, G.S.; Jabbari, B.; Kaufmann, H.C.; Schurch, B.; Silberstein, S.D.; et al. Assessment: Botulinum neurotoxin in the treatment of autonomic disorders and pain (an evidence-based review): Report of the therapeutics and technology assessment subcommittee of the american academy of neurology. Neurology 2008, 70, 1707–1714. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.; Mauskop, A.; Elkind, A.H.; DeGryse, R.; Brin, M.F.; Silberstein, S.; BOTOX CDH Study Group. Botulinum toxin type a for the prophylaxis of chronic daily headache: A subgroup analysis of patients not receiving other prophylactic medications: A randomized double-blind, placebo-controlled study. Headache 2005, 45, 315–324. [Google Scholar] [CrossRef] [PubMed]
- Freitag, F.G.; Diamond, S.; Diamond, M.; Urban, G. Botulinum toxin type a in the treatment of chronic migraine without medication overuse. Headache 2008, 48, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Aurora, S.K.; Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F.; PREEMPT 1 Chronic Migraine Study Group. Onabotulinumtoxina for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the preempt 1 trial. Cephalalgia 2010, 30, 793–803. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.C.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; DeGryse, R.E.; Lipton, R.B.; Silberstein, S.D.; Brin, M.F.; PREEMPT 1 Chronic Migraine Study Group. Onabotulinumtoxina for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the preempt 2 trial. Cephalalgia 2010, 30, 804–814. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.W.; Turkel, C.C.; DeGryse, R.E.; Aurora, S.K.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F.; PREEMPT 1 Chronic Migraine Study Group. Onabotulinumtoxina for treatment of chronic migraine: Pooled results from the double-blind, randomized, placebo-controlled phases of the preempt clinical program. Headache 2010, 50, 921–936. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D. Trpv1, cgrp and sp in scalp arteries of patients suffering from chronic migraine. Some like it hot! Chronic migraine increases trpv1 receptors in the scalp. J. Neurol. Neurosurg. Psychiatry 2015, 86, 361. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, A.M.; Schim, J.D.; Chippendale, T.J. Botulinum toxin type a and divalproex sodium for prophylactic treatment of episodic or chronic migraine. Headache 2008, 48, 210–220. [Google Scholar] [CrossRef] [PubMed]
- Mathew, N.T.; Jaffri, S.F. A double-blind comparison of onabotulinumtoxina (botox) and topiramate (topamax) for the prophylactic treatment of chronic migraine: A pilot study. Headache 2009, 49, 1466–1478. [Google Scholar] [CrossRef] [PubMed]
- Cady, R.K.; Schreiber, C.P.; Porter, J.A.; Blumenfeld, A.M.; Farmer, K.U. A multi-center double-blind pilot comparison of onabotulinumtoxina and topiramate for the prophylactic treatment of chronic migraine. Headache 2011, 51, 21–32. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D.; Blumenfeld, A.M.; Cady, R.K.; Turner, I.M.; Lipton, R.B.; Diener, H.C.; Aurora, S.K.; Sirimanne, M.; DeGryse, R.E.; Turkel, C.C.; et al. Onabotulinumtoxina for treatment of chronic migraine: Preempt 24-week pooled subgroup analysis of patients who had acute headache medication overuse at baseline. J. Neurol. Sci. 2013, 331, 48–56. [Google Scholar] [CrossRef] [PubMed]
- Aurora, S.K.; Dodick, D.W.; Diener, H.C.; DeGryse, R.E.; Turkel, C.C.; Lipton, R.B.; Silberstein, S.D. Onabotulinumtoxina for chronic migraine: Efficacy, safety, and tolerability in patients who received all five treatment cycles in the preempt clinical program. Acta Neurol. Scand. 2014, 129, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, A.M.; Binder, W.; Silberstein, S.D.; Blitzer, A. Procedures for administering botulinum toxin type a for migraine and tension-type headache. Headache 2003, 43, 884–891. [Google Scholar] [CrossRef] [PubMed]
- Silberstein, S.D. Botulinum toxin in headache management. In Botulinum Toxin: Therapeutic Clinical Practice and Science, 1st ed.; Saunders, Elsevier: Philadelphia, PA, USA, 2009; p. 218. [Google Scholar]
- Blumenfeld, A.; Silberstein, S.; Dodick, D.; Aurora, S.; Turkel, C.C.; Binder, W.J. Method of injection of onabotulinumtoxina for chronic migraine: A safe, well-tolerated, and effective treatment paradigm on the preempt clinical program. Headache 2010, 50, 1406–1418. [Google Scholar] [CrossRef] [PubMed]
- Jabbari, B. Migraine and other primary headaches. In Botulinum Toxin Treatment of Pain Disorders; Springer-Verlag: New York, NY, USA, 2015; pp. 49–67. [Google Scholar]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Schaefer, S.M.; Gottschalk, C.H.; Jabbari, B. Treatment of Chronic Migraine with Focus on Botulinum Neurotoxins. Toxins 2015, 7, 2615-2628. https://doi.org/10.3390/toxins7072615
Schaefer SM, Gottschalk CH, Jabbari B. Treatment of Chronic Migraine with Focus on Botulinum Neurotoxins. Toxins. 2015; 7(7):2615-2628. https://doi.org/10.3390/toxins7072615
Chicago/Turabian StyleSchaefer, Sara M., Christopher H. Gottschalk, and Bahman Jabbari. 2015. "Treatment of Chronic Migraine with Focus on Botulinum Neurotoxins" Toxins 7, no. 7: 2615-2628. https://doi.org/10.3390/toxins7072615