
Botulinum Toxin for Neuropathic Pain: A Review of the Literature

1
Department of Rehabilitation Medicine, Seoul St. Mary’s Hospital, College of Medicine, the Catholic University of Korea, 222 Banpo-daero, Seocho-gu, Seoul 06591, Korea
2
Department of Rehabilitation Medicine, St. Paul’s Hospital, College of Medicine, the Catholic University of Korea, Wangsan-ro 180, Dongdaemoon-Gu, Seoul 02559, Korea
*
Author to whom correspondence should be addressed.
Toxins 2015, 7(8), 3127-3154; https://doi.org/10.3390/toxins7083127
Submission received: 27 June 2015
/
Revised: 29 July 2015
/
Accepted: 7 August 2015
/
Published: 14 August 2015
(This article belongs to the Collection Botulinum Toxins on Human Pain)
Abstract
:Botulinum neurotoxin (BoNT), derived from Clostridium botulinum, has been used therapeutically for focal dystonia, spasticity, and chronic migraine. Its spectrum as a potential treatment for neuropathic pain has grown. Recent opinions on the mechanism behind the antinociceptive effects of BoNT suggest that it inhibits the release of peripheral neurotransmitters and inflammatory mediators from sensory nerves. There is some evidence showing the axonal transport of BoNT, but it remains controversial. The aim of this review is to summarize the experimental and clinical evidence of the antinociceptive effects, mechanisms, and therapeutic applications of BoNT for neuropathic pain conditions, including postherpetic neuralgia, complex regional pain syndrome, and trigeminal neuralgia. The PubMed and OvidSP databases were searched from 1966 to May 2015. We assessed levels of evidence according to the American Academy of Neurology guidelines. Recent studies have suggested that BoNT injection is an effective treatment for postherpetic neuralgia and is likely efficient for trigeminal neuralgia and post-traumatic neuralgia. BoNT could also be effective as a treatment for diabetic neuropathy. It has not been proven to be an effective treatment for occipital neuralgia or complex regional pain syndrome.
1. Introduction
Botulinum neurotoxin (BoNT), derived from Clostridium botulinum, has been used worldwide for not only cosmetic therapeutic purposes but also for the treatment of neurologic disorders, such as dystonia or spasticity [1,2]. It has been approved by the Food and Drug Administration (FDA) as a treatment for strabismus, blepharospasm, hemifacial spasm, focal dystonia, and upper limb spasticity in the United States [3].
BoNT has seven antigenically different serotypes (A–G) [4], and its main mechanism is the inhibition of acetylcholine (Ach) neurotransmitter release at presynaptic nerve terminals, which results in a reduction of muscle fiber activity [2,4,5]. BoNT inhibits the exocytosis of Ach from cholinergic nerve endings by endocytosing into the presynaptic membranes of neuromuscular junctions and cleaving proteins that are essential for Ach exocytosis [6]. These proteins are required for the docking of Ach-containing vesicles to presynaptic membranes. Without this docking, Ach cannot be released into the synaptic cleft, and the innervated structure can become paralyzed.
Each serotype of BoNT acts as a protease that specifically targets soluble N-ethylmaleimide-sensitive factor attachment protein receptor (SNARE) proteins by attaching a light chain, which is an active part of the toxin [7]. With the plasma membrane, the SNARE proteins form a core that is required to mediate the fusion of synaptic vesicles (SVs). The SNARE proteins include synaptosomal-associated protein of 25 kDa (SNAP-25), target membrane proteins, syntaxin, and the vesicle-associated membrane protein (VAMP)/synaptobrevin. BoNT/A—the most well-known toxin—and BoNT/E cleave SNAP-25 at two different sites. BoNT/B, /D, /F, and /G cleave VAMP/synaptobrevin at different sites, whereas BoNT/C cleaves both syntaxin and SNAP-25 [4,7].
Aside from blocking the release of Ach, it has been suggested that BoNT, particularly BoNT/A, may inhibit the release of local nociceptive neuropeptides, such as substance P, calcitonin gene-related peptide (CGRP), and glutamate, as well as the expression of the transient receptor potential vanilloid 1 (TRPV1) [8,9,10,11]. Through this process, BoNT/A may inhibit neurogenic inflammation and peripheral sensitization. In discovering the different mechanisms of the different BoNTs, in vivo data have been generated that suggest that BoNT can serve as a potential treatment for pain. In addition, the FDA approved Botox® for the treatment of chronic migraines in 2010 after investigating its efficacy in reducing the frequency and intensity of chronic migraines [12,13]. BoNT/A is the only approved prophylactic drug, with a peripheral application [14]. In addition to the impairment of SNARE-mediated synaptic vesicle fusion to nerve terminals, this study demonstrated that BoNT/A selectively inhibits C- but not Aδ-menigeal nociceptors. BoNT inhibited mechanical transduction in suture branches of meningeal nociceptors during extracranial application. Burstein et al. [14] suggest that during the prophylactic application of BoNT/A for migraines, it prevents high-threshold mechanosensitive ion channels from fusing into the nerve terminal membrane and lowers the neuronal surface expression of these channels.
The spectrum of the usage of BoNT/A for the treatment of pain is increasing, and the possibility that BoNT/A can be used as a treatment for a wider variety of pain disorders is currently being explored. However, the entire process by which BoNT/A exerts pain relief is not yet clear.
Neuropathic pain is a type of pain that is “caused by a lesion or disease of the somatosensory system” [15], and recent studies have suggested that BoNT/A is effective for the treatment of different clinical conditions that present with neuropathic pain, such as postherpetic neuralgia, diabetic neuropathy, post-traumatic neuralgia, complex regional pain syndrome, trigeminal neuralgia, and occipital neuralgia [12,16,17,18].
The aim of this review is to investigate the mechanisms behind the antinociceptive actions of BoNT/A, its axonal transport, and its anti-inflammatory properties and to provide a compilation of data that report on the therapeutic use of BoNT injections for neuropathic pain conditions by assigning levels of evidence according to the American Academy of Neurology guidelines. A literature search was conducted using the PubMed and OvidSP databases (1966–May 2015) with the following cross-searching terms: “Botulinum toxins, type A”, “botulinum toxin”, “botulinum neurotoxin”, “neuralgia”, “neuropathy”, “pain”, “chronic pain”, and “neuropathic pain”. The results included randomized controlled trials, observational studies, and case reports. Additional references were found by reviewing individual references from the articles, which were searched using PubMed.
2. Mechanisms of the Antinociceptive Effects of Botulinum Toxin
There have been several preclinical studies showing that BoNT/A inhibits the release of neurotransmitters that regulate pain and inflammation [11,19]. A rat formalin-induced inflammatory pain model was used in an early in vivo preclinical study that showed the antinociceptive effects of BoNT/A [11]. A subcutaneous BoNT/A injection reduced inflammatory hyperalgesia and edema. An intrathecal injection of BoNT/A showed similar analgesic effects in animal models of formalin-induced pain [19].
Welch et al. observed that BoNT inhibits the release of substance P from cultured embryonic rat dorsal root ganglia neurons [20]. In this study, dorsal root ganglia neurons showed different sensitivities for each serotype of BoNT; they were the most sensitive to BoNT/A, suggesting differences in receptor affinity between the various BoNT serotypes. The effects of BoNT/A cleavage of SNAP 25 appeared after two hours, whereas substance P secretion was inhibited after four hours. This effect of BoNT/A lasted for up to 15 days. In rat trigeminal ganglia cells, BoNT/A directly diminished the amount of calcitonin gene-related peptide (CGRP), an inflammatory neuropeptide [21]. Incubating the cell cultures with BoNT/A was more effective in suppressing stimulated CGRP secretion than incubating them with a control. Substance P and CGRP are neurotransmitters produced by dorsal root ganglia neurons, mainly C fibers, a primary nociceptive afferent. This suggests that BoNT/A inhibits the release of these neurotransmitters from primary sensory neurons [8]. These neurotransmitters can act on blood vessels and induce vasodilatation. This can cause flares of weals to appear on the skin around lesions. By inhibiting the release of these neurotransmitters, BoNT/A can decrease tenderness and pain in areas where sensitized nociceptors are pathologically altered. Ultimately, substance P and CGRP contribute to peripheral sensitization during inflammation and indirectly reduce central sensitization [6,8,22].
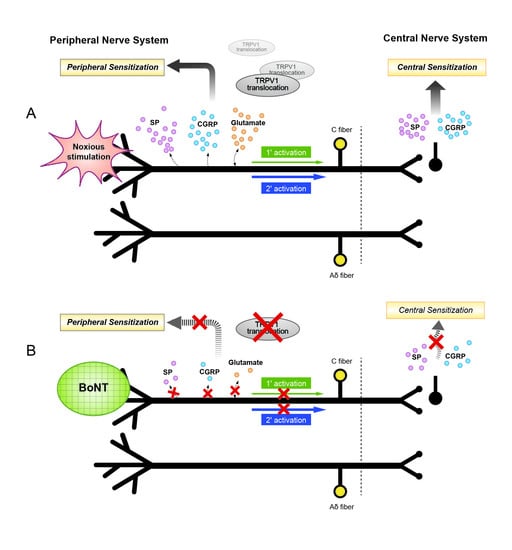
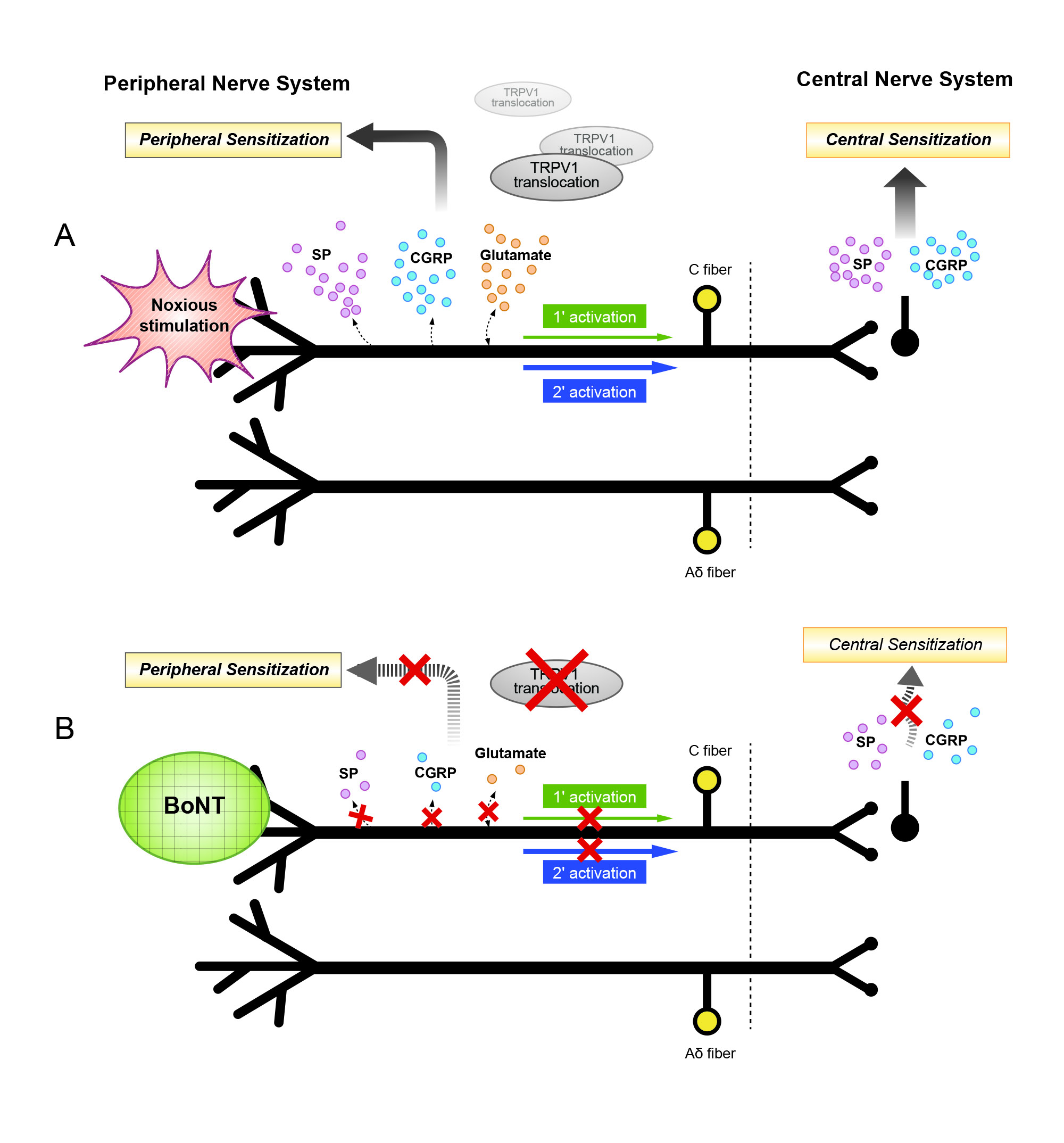
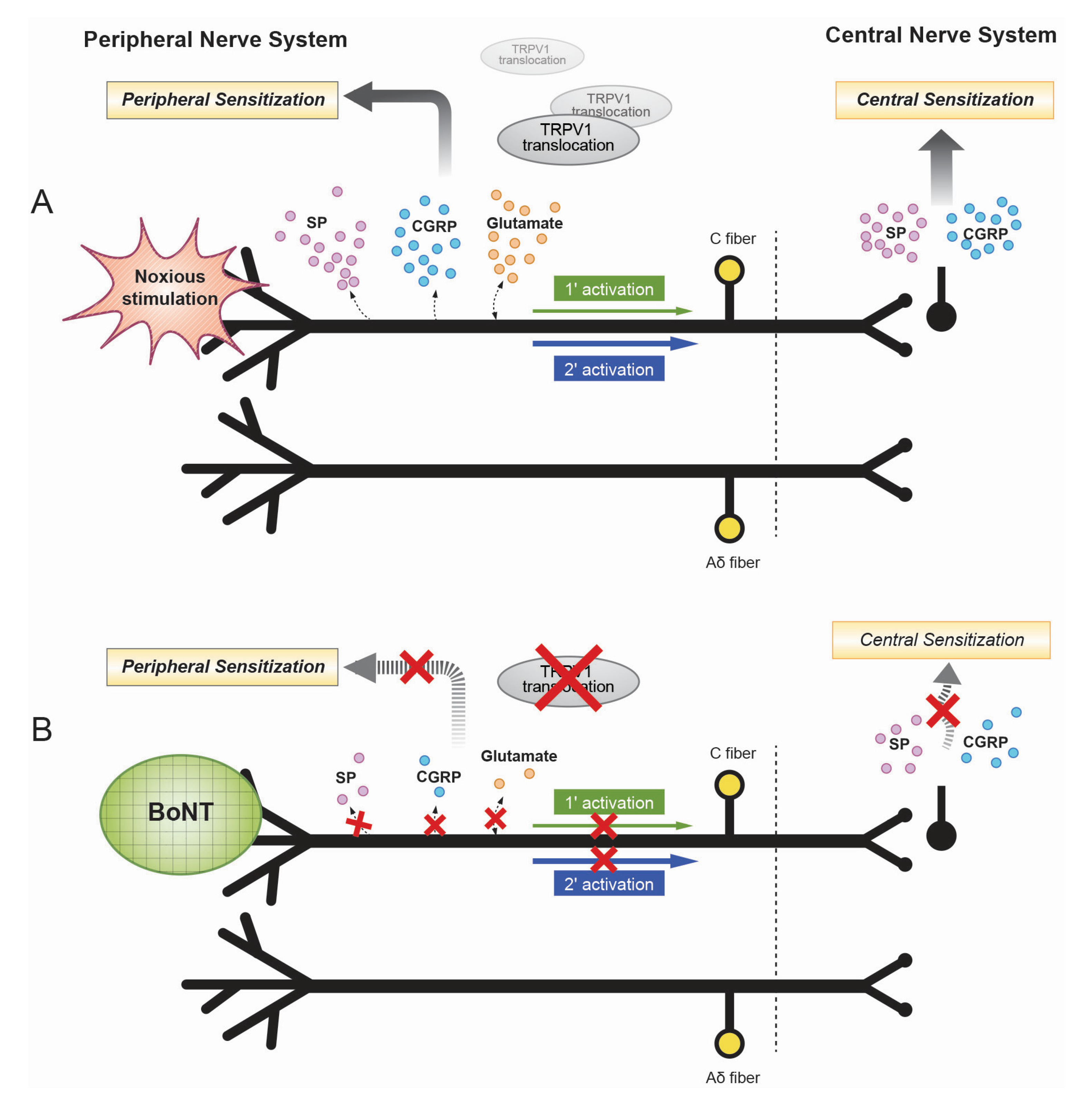
In addition, BoNT can decrease the delivery of the transient receptor potential vanilloid 1 (TRPV1) to neuron cell membranes [23]. TRPV1 is an ionotropic receptor that intensifies the excitability of nociceptors, responding to noxious stimuli, such as heat and proalgesic substances. BoNT/A can inhibit the SNARE-mediated translocation of TRPV1 to the plasma membrane [24]. TRPV1 has an important role during the processing of peripheral thermal and inflammatory pain. Proalgesic agents can up-regulate TRPV1 expression and channel activity [23]. BoNT/A is also effective in inhibiting the release of excitatory neurotransmitters, such as glutamate. In a study that utilized a guinea pig formalin-induced pain model [25,26], glutamate concentrations decreased after an injection of BoNT compared with an injection of saline. Glutamate secretion was also inhibited in a synaptosome preparation from the cerebral cortex of a guinea pig (Figure 1).
Figure 1.
(A) Illustrated mechanism of peripheral and central nerve system sensitization. Noxious stimulation may lead to peripheral sensitization through release of neuropeptides and inflammatory mediators. The peripheral sensitization may result in sensitization of the central nerve system. SP indicates substance P; CGRP, calcitonin gene-related peptide; TRPV1, transient receptor potential vanilloid 1. (B) The antinociceptive mechanism of botulinum neurotoxin (BoNT) in the treatment of neuropathic pain including decrease in peripheral SP, CGRP, glutamate, TRPV1 receptor translocation, leading to direct block of peripheral sensitization. As substance P and CGRP secretion are blocked within central nerve system, central sensitization is also indirectly reduced.
Figure 1.
(A) Illustrated mechanism of peripheral and central nerve system sensitization. Noxious stimulation may lead to peripheral sensitization through release of neuropeptides and inflammatory mediators. The peripheral sensitization may result in sensitization of the central nerve system. SP indicates substance P; CGRP, calcitonin gene-related peptide; TRPV1, transient receptor potential vanilloid 1. (B) The antinociceptive mechanism of botulinum neurotoxin (BoNT) in the treatment of neuropathic pain including decrease in peripheral SP, CGRP, glutamate, TRPV1 receptor translocation, leading to direct block of peripheral sensitization. As substance P and CGRP secretion are blocked within central nerve system, central sensitization is also indirectly reduced.

Paterson et al. found that BoNT/A selectively increased the threshold of mechanical pain without changing the thermal detection or pain threshold [27]. The effect of BoNT/A on mechanotransfution was evaluated at the cellular level. Cultured mouse dorsal root ganglion neurons were exposed to BoNT/A. BoNT treatment showed no change in rapidly and intermediately adapting, mechanically activated inward currents, while there was a significant decrease in the proportion of cells expressing a slowly adapting, mechanically gated current with local pressure to the cell soma. There was no effect of BoNT/A on the activation threshold of mechanically gated currents with a slight decrease in the peak current intensity. It has been believed that the slowly adapting, mechanically gated current in dorsal root ganglion neurons has been linked to noxious mechanosensation; conotoxin noxious mechanosensation blocker-1 selectively inhibits slowly adapting, mechanically activated currents. This action increases mechanical pain threshold without changing light touch or heat sensitivity [28]. The responsible channels for this current are not known yet. More possible explanation can be effects of BoNT/A on the trafficking of mechanosensitive channels. BoNT would block vesicular traffic and suppress protein kinase C activation. Mechanically gated currents could be upregulated by inflammatory mediators in sensory neuron cultures [27,29].
BoNT/A has been used as a treatment for pain associated with neuromuscular hyperactivity disorders, such as spasmodic torticollis and cervical dystonia, for decades [3,30]. It was initially believed that BoNT/A reduced pain by inducing muscular relaxation through inhibiting the release of acetylcholine [6]; this might indirectly reduce the painful ischemia that can be caused by a hyper-contracted muscle. However, there have been a few cases in which pain relief was observed even in patients who did not show any improvements in hyperactive muscle contraction [31]. Additionally, clinicians have reported cases of pain relief occurring before muscle relaxation [32]. It was also discovered that pain relief existed even after the effects of muscle relaxation disappeared, measured by reduced bite force in patients treated for temporomandibular disorders [33]. In a study by Relja and Klepac [34], pain relief was observed one week after BoNT/A injection in patients with spasmodic torticollis, whereas paralytic effects started two weeks after the injection. Lower doses (50 units) of BoNT/A were necessary to induce analgesic effects, whereas 100 to 150 units were needed to create a paralytic effect [34]. This implies that the mechanism behind the antinociceptive effects of BoNT/A is more complex than muscle relaxation and that these effects on pain can be explained.
There are efforts to find additional explanations for BoNT as a treatment. Xiao et al. were interested in the potential interaction between BoNT/A and transmembrane channels/receptors, which are closely linked to pain [35]. They performed a study to determine the effects of BoNT/A on neuropathic pain and the expression of purinergic P2X3 receptor in the dorsal root ganglion of rats with neuropathic pain caused by L5 ventral root transaction. Either saline or BoNT/A was injected to plantar surfaces. Before and after the operation, behavioral tests were done. After 3, 7, 14 and 21 days, immunoreactivity was used to detect the expression of P2X3 receptors in the dorsal root ganglion. Nerve transaction induced bilateral mechanical allodynia and over-expression of P2X3 receptors in the dorsal root ganglion of the rats. Subcutaneous intraplantar injection of BoNT/A reduced the neuropathic behavior and the over-expressed P2X3 receptors of nociceptive neurons. This study shows over-expressed P2X3 receptors in this ventral root transaction model and reveals a novel mechanism of BoNT, acting on nociceptive neurons.
For phantom limb pain and phantom sensation, in cases where the nerves are transected, the pain is characterized by the cortical perception of an amputated body part [36]. There are suggested pathophysiologies, including ectopic activities at the neuroma, which are formed at the transected nerve ending in the residual limb. Early studies of rat transected sciatic nerves showed that the site of neuroma is complicated and dynamic. Images of neuromas show multiple sprouts growing out from each cut axon and can travel in many directions, including back along the axon. The neuroma can increase sympathetic tone through central plasticity and sensitization. There are usually immediate changes of chemical transport including the dorsal root ganglion and from peripheral to central nervous system. The central pathways involve hyperexcitability in the spinal cord, and this can cause somatosensory cortical reorganization.
To increase the potential of BoNT for therapeutic usage, developing a recombination of BoNT can be promising. Before discussing the recombination, the structure of BoNT/A complex should be discussed first. As mentioned, there are the seven distinct serotypes (A–G) which selectively block different proteins of the SNARE. While toxin types C and D are causes of illness in animals, the toxin types A, B, E, F are well-known causes of human botulism [4,37]. The serotypes cleave proteins, required for the synaptic vesicles to fuse to the presynaptic membrane and block the exocytosis of neurotransmitters. The BoNT consist of a light chain which is linked to a heavy chain through a disulphide bridge [38,39,40]. The heavy chain has a carboxy terminal membrane acceptor-binding domain, and BoNT/A can bind to overactive nerve endings with high affinity through the C-terminal half of the heavy chain. The heavy chain also has a translocation domain at the N-terminal which can mediate the toxin binding to nerve terminals. The light chain enters the presynaptic cytosol and prevents neurotransmitter release by the enzymatic cleavage of SNAP-25 [41].
Cleaving SNAP-25 at different sites, BoNT/A and BoNT/E have very different durations of actions [42]. The paralytic effects of BoNT/A last for months in humans and for weeks in mice; BoNT/E acts for short periods, in the span of days. While BoNT/A reduces the fusion rate, BoNT/E completely inhibits vesicle fusion, akin to the effects of VAMP [41]. In addition, when BoNT/E inhibits neurotransmitter release, it is not influenced by treatments that elevate cytosol (Ca2+). BoNT/E can enter the cultured neuron faster than BoNT/A. With higher potency, it can inhibit transmission at the neuromuscular junction more quickly. These properties of BoNT/E are attractive to improve therapeutic versions of BoNT; however, BoNT/E also has a downside—it can produce transient muscle weakness—compared with the long action duration of BoNT/A. To find a responsible domain for the properties, the C-terminal half of the heavy chain was exchanged to create chimeras.
In Wang et al.’s study, chimeras were produced by swapping the C-terminal half of the heavy chain domains between BoNT/A and /E [39]. Recombinant EA has the light chain and N-terminal half of the heavy chain domains of BoNT/E and the C-terminal half of the heavy chain of BoNT/A, while AE comprises the light chain and N-terminal half of the heavy chain of BoNT/A. Swapping BoNT domains yields novel features; chimera EA was fast-acting and more potent than BoNT/A at the neuromuscular junction. EA was as potent and fast as BoNT/E, and they were equivalently sensitive to dose-dependent inhibition of the vesicular proton pump. AE produced persistent muscle weakness, which can be therapeutic potential. This advanced technology can bring further advances to the therapeutic use of BoNT.
3. Axonal Transport of Botulinum Toxin
Antonucci et al. provided biochemical evidence that BoNT/A can cleave SNAP-25 distant from an injection site, suggesting that axonal transport of BoNT/A occurs within central neurons [43]. There have been reports on the bilateral effects of BoNT/A after a unilateral injection [44,45,46]. In a study by Bach-Rojecky et al., BoNT/A injections were administered to a rat model of diabetic neuropathy that was induced by streptozotocin [45]. After BoNT/A application, mechanical and therapy hyperalgesia improved on both the ipsilateral and contralateral sides. This antinociceptive effect lasted for more than 15 days.
In another study, Bach-Rojecky et al. suggested that the central antinociceptive effects of BoNT/A are driven by axonal transport, which was demonstrated in a unilateral acidic saline-induced animal model with bilateral hyperalgesia [44]. This “mirror pain”, induced by unilateral injections of acidic saline, was suggested to be of central origin. Therefore, the authors had expected that applying BoNT/A peripherally would not show any effects on bilateral pain. However, bilateral pain was reduced when a unilateral subcutaneous injection of BoNT/A (5 units/kg) was performed on the ipsilateral side. In addition, BoNT/A (0.5 units/kg) still reduced bilateral pain when it was injected into a proximal region of a distally transected sciatic nerve. In both cases, a unilateral injection reduced acidic saline-induced bilateral mechanical hyperalgesia.
In an animal study, the antinociceptive effects of BoNT/A were investigated on paclitaxel-induced peripheral neuropathy [46]. After being injected with paclitaxel, a chemotherapeutic drug, rats showed a decreased withdrawal nociceptive reflex bilaterally in their hind paws. Again, after the toxin was injected on the unilateral side, analgesic effects were observed bilaterally. These data suggest that BoNT/A might affect the central nervous system (CNS) [38], as they cannot be explained solely by BoNT/A’s actions on peripheral nerve endings. The toxin might have diffused hematogenously, but the administered dose (20 units/kg subplantar injection) was not sufficiently high to induce systemic side effects. Furthermore, the protein is not sufficiently small to pass through the blood-brain barrier. Therefore, one possible theory is that BoNT/A is axonally transported from the periphery to the CNS. However, this theory has not yet been proven [38].
In the previously mentioned study by Bach-Rojecky et al., to prevent retrograde axonal transport, an axonal transport blocker, colchicine, was injected into the ipsilateral sciatic nerve, after which the bilateral antinociceptive effects disappeared [44]. An injection of colchicine into the contralateral side did not eliminate the antinociceptive effects, suggesting that the axonal transport of BoNT/A from peripheral nerves toward the CNS.
In a study by Wiegand et al., 125I-BoTN/A was injected unilaterally into the gastrocnemius muscle of a cat to trace the toxin [47]. After the injection, radioactivity was progressively observed first in the sciatic nerve and then in the ipsilateral spinal ventral roots and the ipsilateral spinal cord segment after 48 h. This study suggested the possibility of the toxin moving into the CNS via axonal transport; however, it could not prove that the enzymatically active toxin reached the CNS.
There have been studies that have shown the opposite effect. In a study by Tang-Liu et al., an 125I-radiolabeled BoNT-hemagglutinin complex (BoNT/A-complex) and 125I-radiolabeled free BoNT/A were compared; these radioiodinated compounds were injected into the gastrocnemius muscles of cats and the eyelids of rabbits and measured at different time-points [48]. No systemic effects were observed in either the rats or rabbits. The 125I-radiolabeled BoNT/A-complex and free BoNT/A remained near the injection sites. Radioactivity was detected in distal tissues, such as the thyroid gland, and contralateral muscles and skin; however, the authors suggested that this was mainly due to the low molecular weights of 125I-iodide and 125I-containing peptides. In rabbits, neither the 125I-relabeled BoNT/A complex nor the free BoNT/A were observed in any distant tissues. The authors concluded that the majority of the neurotoxin remained near the injection sites, either as a complex or in free form.
As discussed in Section 2, it was suggested that BoNT/A inhibits neurotransmitter release from sensory nerve endings by cleaving peripheral SNAP-25 [8,11]. The trigeminal system of a rat formalin-induced model was employed to identify which neurons participate in BoNT/A axonal transport [48,49]. A low dose (3.5 units/kg) of BoNT/A was injected into either the rat whisker pad or sensory trigeminal ganglion (1 unit/kg). Colchicine was injected into the trigeminal ganglion to prevent axonal transport. Both injections of BoNT/A were effective in reducing formalin-induced pain in the rat. Colchicine completely prevented the antinociceptive effects of BoNT/A. After the toxin was injected into the rat whisker pad, BoNT/A-truncated SNAP-25 was immunohistochemically labeled in the medullary dorsal horn of the trigeminal nucleus; it was evident in the spinal trigeminal nucleus three days after the peripheral application of even the low dose. Therefore, in this study, it was suggested that axonal transport is required for the antinociceptive effects of BoNT/A in sensory neurons and that truncated SNAP-25 in central sensory nociceptive nuclei is also associated with these effects [49,50].
There are arguments about whether BoNT are retrogradely transported from the injection site or not. In this review, the mechanism of the antinociceptive action of BoNT/A at the peripheral and/or central level is investigated. Marinelli and colleagues analyzed the expression of cl-SNAP-25 from nerve endings of the hind paw to the spinal cord after applying BoNT/A peripherally [51]. With chronically injured sciatic nerves of mice, immunostained cl-SNAP-25 in the peripheral nerve endings were evaluated along the sciatic nerve including dorsal root ganglia and spinal dorsal horns after the injections. The injections included pure saline, BoNT/A, or combination of BoNT/A with either glial fibrillar acidic protein, complement receptors, or neuronal nuclei. On the all the examined tissues, there were immunostained cl-SNAP-25 from the peripheral nerve endings to the spinal cord; these results support a retrograde transport of BoNT/A. Additional in vitro experiments were also done to evaluate whether the proliferative state of Schwann cells would interact with BoNT/A or not. As results, BoNT/A modulated the proliferation of Schwann cells, inhibiting the acetylcholine release. These results support the retrograde transport of the BoNT/A along the nerve.
In the study of Restani et al., the BoNT/A was injected into the adult rat optic tectum, producing SNAP-25 cleavage in retinal neurons, which are distanced from the injection site [42]. The retinal endings showed impaired exocytosis including cleaved, enlarged SNAP-25 and an abnormally high number of synaptic vesicles. The injection produced truncated SNAP-25 in cholinergic amacrine cells. The cholinergic-driven wave activities were decreased on the functional images with calcium indicators, meaning impairments in neurotransmission. These results are consistent with the effects of the retrograde trafficking of BoNT/A.
In another study, it was suggested that intraplantar BoNT/B could have not only acute local effects upon the peripheral afferent nerve but could also transport to the central afferent terminals over time [52]. Each mouse received 1 unit of BoNT/B into its unilateral plantar of the mouse and saline into the contralateral side. After 4 h, 1, 7 and 21 days, they received injections of 1% capsaicin into bilateral plantar surfaces. In the results, the injected side showed local early effect of ipsilateral capsaicin-evoked plasma extravasations. This means local uptake and effect on afferent terminals. The ipsilateral injected side had reduced intraplantar formalin-evoked flinching, capsaicin-evoked plasma extravasation, formalin-evoked dorsal horn substance P release, and formalin-evoked dorsal horn neuronal activation (c-fas). It also had reduced ipsilateral dorsal root ganglion VAMP, ipsilateral substance P release otherwise evoked bilaterally by capsaicin, and ipsilateral activation of c-fas otherwise evoked bilaterally. Intrathecal substance P-evoked c-fas activation is unilaterally blocked by the BoNT/B, suggesting a transsynaptic event. The results of this study suggest that BoNT/B can be taken up by the peripheral terminal and be transported to the ipsilateral dorsal root ganglia (DRG) to cleave VAMP. BoNT/B could act presynaptically. In addition, the observations provided evidence for possible transsynaptic effects of intraplantar BoNT. These results suggest that peripheral BoNT/B can change peripheral and central terminal release from a nociceptor and attenuate downstream nociceptive processing via a presynaptic effect, suggesting a possible postsynaptic effect.
The study of Xu et al. [53] did not focus on neuropathic pain, but it did show postsynaptic actions by BoNT/A on the salivary gland. In this study, the authors evaluated the effects of BoNT/A on the apical plasma membrane water channel aquaporin-5 [53]. This study demonstrated that saliva secretion in rat submandibular glands reversibly decreased after the application of BoNT/A. This action was by not only presynaptic SNAP-25 cleavage at the neuroglandular junctions but also the postsynaptic water channel redistribution. The cell surface protein levels of water channels after the applications of BoNT/A reduced without affecting the total protein expression of the water channel, and through immunofluorescence, there was translocation of the water channels from the membrane to the cytoplasm, suggesting the redistribution of the water channels.
4. Botulinum Toxin and Inflammation
In peripheral neuropathies, BoNT/A can reduce neurogenic inflammation [54]. In the rat formalin-induced pain model, BoNT/A was injected into the rat paw one week prior to formalin injection [11]. The post-formalin inflammatory peak of pain was reduced for certain doses of BoNT/A. In examining the injection site, both inflammation and the concentration of glutamate were reduced compared with controls. In a capsaicin-induced prostatitis rat model, BoNT inhibited both cyclooxygenase-2 expression [55] and G protein family expression, including Rho guanosine triphosphatase, which activates interleukin-1, a pro-inflammatory cytokine [56]; in this manner, the BoNT injection suppressed capsaicin-induced prostatitis.
It has been proposed that the antinociceptive and anti-inflammatory activities of BoNT have common peripheral mechanisms [57]. The anti-inflammatory effects were thought to affect pain by reducing the release of peripheral neurotransmitters and inflammatory mediators [54]; however, this relationship is still controversial. BoNT/A was injected into an animal model of carrageenan-induced hyperalgesia [46,57] and was effective in reducing mechanical and thermal hyperalgesia, although no improvements in local tissue inflammatory edema or plasma protein extravagation were observed. These results showed a dissociation between the antinociceptive and anti-inflammatory effects of BoNT/A [54]. In a study by Cui et al., the anti-inflammatory effects of BoNT were dose-dependent, whereas its antinociceptive effects were not [11]. Experimental studies in humans have also shown similar results [58]: Pain relief was observed only when capsaicin was injected into a BoNT/A-pretreated area. Neurogenic inflammation, including flare and vasodilatation, was reduced even when capsaicin was injected adjacently into a toxin-pretreated region where pain was not reduced. It has been suggested that the anti-inflammatory effects of BoNT/A on vasodilatation and neurogenic flare do not completely correlate with its antinociceptive effects. The relationship between the anti-inflammatory and antinociceptive effects of BoNT/A is still controversial.
5. Clinical Evidence of Botulinum Toxin for Neuropathic Pain
Neuropathic pain is caused by any injury to the peripheral or central nervous system [15]. The results from several double-blind, placebo-controlled studies and increasing evidence from case series and reports have suggested that BoNT/A has antinociceptive effects in neuropathic pain [9], and BoNT/A is expected to be an effective treatment for chronic pain. Francisco et al. have suggested that BoNT/A can offer benefits to patients with certain types of neuropathic pain [59]. It is probably effective in relieving postherpetic neuralgia, likely or possibly effective in relieving post-traumatic neuropathic pain, and likely effective in relieving diabetic neuropathy. For allodynia related to postherpetic neuralgia and post-traumatic pain, a neurogenic pain mechanism may be important due to peripheral nerve lesions [60].
There were previous preclinical studies that showed the similar antinociceptive effects of BoNT/A in animal models. In a partial sciatic nerve transection model, BoNT/A reduced neuropathic pain [61]; it also reduced thermal and mechanical hyperalgesia, as well as mechanical and cold allodynia [62]. Additionally, mechanical and cold allodynia were reduced in a spinal nerve ligation model [63]. In a further study, it was also effective in reducing mechanical allodynia in sciatic nerve injury-induced neuropathy [64,65,66]. Recently published clinical studies are reviewed in this section (Table 1).

{kind=link}
{kind=link}
| References | AAN Class | Study Type (Design) | Number of Patients | Diagnosis | Injection Route/Site/Serotype/Dose | Result |
|---|---|---|---|---|---|---|
| Xiao et al. [18] (2010) | I | Randomized, double-blind, placebo-controlled | 60 | Post-herpetic neuralgia | Subcutaneously/over the area of allodynia/BoNT/A/5 IU per site | VAS reduction and sleep quality improvement; superior to control group |
| Apalla et al. [67] (2013) | I | Randomized, double-blind, placebo-controlled | 30 | Post-herpetic neuralgia | Subcutaneously/over the affected area in a chessboard manner/BoNT/A/5 IU per point (Total 100 IU) | VAS at least 50% reduction in 13 patients in the intervention group and significant reduction in sleep scored |
| Ranoux et al. [16] (2008) | I | Randomized, double-blind, placebo-controlled | 29 (4 post-herpetic) | Post-herpetic neuralgia or post-traumatic/post-surgery neuropathy | Intradermally/into painful area/BoNT/A/20–190 IU | Decreased VAS, burning sensation, allodynic brush sensitivity, a reduced number of pain paroxysms, and improvements in quality of life |
| Liu et al. [68] (2006) | IV | Case report | 1 | Post-herpetic neuralgia | Subcutaneously/over the all painful area in a fan pattern/BoNT/A/100 IU | VAS reduction from 10 to 1 (lasting for 52 days) |
| Sotiriou et al. [69] (2009) | IV | Case series | 3 | Post-herpetic neuralgia | Subcutaneously/20 injection in a chessboard pattern/BoNT/A/100 IU | VAS decreased within three days (lasting for 64 days) |
| Wu et al. [70] (2012) | I | Randomized, double-blind, placebo-controlled, parallel design | 42 (22 BoNT, 20 placebo) | Trigeminal Neuralgia | Intradermally or submucosally/into trigger zones/BoNT/A/75 IU | Reduction in VAS (>50%) in 68% (BoNT group) vs. 15% (placebo group) |
| Bohluli et al. [71] (2011) | IV | Prospective, open, case series | 15 | Trigeminal Neuralgia | Not specified injection mode/into trigger zones/BoNT/A/50–100 IU | 100% improvement in global assessment scale, frequency of pain attacks, and VAS scores |
| Zúñiga et al. [72] (2008) | IV | Prospective, open, case series | 12 | Trigeminal Neuralgia | Subcutaneously/into trigger zones/BoNT/A/20–50 IU | Reduction in VAS (from 8.8 to 4) and number of paroxysmal attacks in 10 patients (lasting for two months) |
| Türk et al. [73] (2005) | IV | Prospective, open, case series | 8 | Trigeminal Neuralgia | Two points (depth 1.5–2 cm) around zygomatic arch/BoNT/A/50 IU per point (total 100 units) | Reduction in VAS and the frequency of attacks (100%) |
| Piovesan et al. [74] (2005) | IV | Prospective, open pilot study | 13 | Trigeminal Neuralgia | Subdermally/painful area in a grid pattern/BoNT/A/3 IU per point (total 6–9 IU) | Reduction in VAS for 60 days (100%: Pain-free (4), more than 50% reduction (9)) |
| Borodic et al. [75] (2002) | IV | Prospective, open pilot study | 11 | Trigeminal Neuralgia | Subdermally or Intradermally/subcutaneous trigger zones (depth 1–3 mm, 10 mm apart)/BoNT/A/total 30–50 IU | Reduction in pain (>50%) in eight patients and frequency (lasting for 2–4 months) |
| Ngeow and Nair [76] (2001) | IV | Case report | 1 | Trigeminal Neuralgia | Subcutaneously/two trigger zones over painful area/BoNT/A/100 IU total | Complete pain relief in nasal area and partial at mental region |
| Yoon et al. [77] (2010) | IV | Case report | 1 | Trigeminal Neuralgia | Subcutaneously/one point in the middle chin/BoNT/A/10 IU | Decreased painful area and pain intensity |
| Allam et al. [78] (2005) | IV | Case report | 1 | Trigeminal Neuralgia | Subcutaneous/eight points along the area of V1 and V2/BoNT/A/2 IU per point (total 16 IU) | Reduction in pain (lasting for 90 days) |
| Layeeque et al. [79] (2004) | IV | Prospective, non-randomized, placebo-controlled | 48 (22 BoNT, 26 control) | Post-surgical neuralgia | Pectoralis major, serratus anterior, and rectus abdominis muscles/BoNT/A/100 IU | Significantly reduced post-surgical pain and facilitated reconstruction with tissue expander |
| Yuan et al. [17] (2009) | II | Randomized, double-blind, placebo-controlled, crossover trial | 20 | Diabetic neuropathy | Intradermally/into the dorsum of the foot in a grid distribution patterns/BoNT/A/4 IU per site (50 units into each foot) | Significant VAS reduction at one, eight, and 12 weeks after injection (lasting for 12 weeks) and improvement in sleep quality in BoNT group |
| Ghasemi et al. [80] (2014) | I | Randomized, double-blind, placebo-controlled | 40 | Diabetic neuropathy | Intradermally/in a grid distribution pattern of 12 sites across the dorsum of the affected foot/BoNT/A/100 IU | Reduced NPS scores and DN4 scores and 30% patients pain-free in intervention groups |
| Kapural et al. [81] (2007) | IV | Retrospective, open, case series | 6 | Occipital Neuralgia | Perineural/occipital nerve block/BoNT/A/50 IU | Reduction of VAS and Pain Disability Index Scores in five of six patients at four weeks |
| Taylor et al. [82] (2008) | IV | Prospective, open, case series | 6 | Occipital Neuralgia | Perineural/around the occipital nerve/BoNT/A/100 IU | Significant improvement in sharp/shooting pain scores |
| Breuer et al. [83] (2006) | I | Randomized, double-blind, placebo-controlled | 20 | Carpal tunnel syndrome | Intramuscularly/into three hypothenar muscles/BoNT/B/2500 IU | No difference compared with the placebo group |
| Tsai et al. [84] (2006) | IV | Prospective, open, pilot study | 5 | Carpal tunnel syndrome | Intracarpally/on each side of the carpal tunnel/BoNT/A/60 IU | Insignificant trend toward pain improvement at three months without change in conduction time by NCS in three patients |
| Safarpour et al. [85] (2010) | III | 1. Randomized, double- blind, placebo-controlled study; 2. uncontrolled, unblended, open-label study | 14 (8 BoNT/A, 6 control) | CRPS | Intradermally and subcutaneously/into the allodynic area/BoNT/A/5 IU per point (total 40–200 units) | No response to the BoNT in VAS; study terminated prematurely because of injection intolerance |
| Carroll et al. [86] (2009) | III | Randomized, double-blind, placebo-controlled crossover trial | 18 (9 crossover study) | CRPS | Lumbar sympathetic block/BoNT/A/Bupivacaine 0.5% + 75 IU of BoNT/A | Longer duration of pain reduction (median 71 days) in BoNT/A group than the control group (median 10 days) |
| Kharkar et al. [87] (2011) | IV | Retrospective, uncontrolled, nblended study | 37 | CRPS | Intramuscularly/neck or upper limb girdle muscles/BoNT/A/10–20 IU per muscle (total 100 IU) | The 97% patients reported reduction of pain by 43% |
| Argoff et al. [54] (1999) | IV | Prospective, open, case series | 11 | CRPS | Subcutaneously/into shoulder girdle muscles/BoNT/A/25–50 IU (total 300 IU) | Reduction in VAS, allodynia, and hyperalgesia and improved skin color |
| Safarpour and Jabbari [88] (2010) | IV | Case series | 2 | CRPS | Intramuscularly/trigger points in the proximal muscles/BoNT/A/20 IU per site | Reduction in proximal and distal pain of myofascial pain syndrome and CPRS |
| Wu et al. [89] (2012) | III | Prospective, randomized, double-blind pilot study | 14 | Residual limb pain or phantom limb pain | Intramuscular and cutaneous/subcutaneously/into focal tender points BoNT/A, 50 IU per site (total 250–300 IU) | Reduced residual limb pain, compared with the lidocaine/depomedrol group; not effective for phantom limb pain |
| Jin et al. [90] (2009) | IV | Case series | 3 | Residual limb pain or phantom limb pain | Electromyography (EMG)-guided injection/into the painful stumps points with strong fasciculation/BoNT/A/500 IU | Significant pain reduction, improved prosthesis tolerance, and reduced pain medication (100%) |
| Kern et al. [91] (2004) | IV | Case report | 1 | Residual limb pain or phantom limb pain | Into trigger points of the stump/BoNT/A/4 × 25 IU | Almost completely pain-free and reduced pain medication |
| Uyesugi et al. [92] (2010) | IV | Case report | 1 | Painful keloid | Subcutaneously/throughout the scar in a fan-like distribution BoNT/A, total 100 IU | Reduction in VAS (from 8 to 6) at five weeks and time periods of pain-free increased |
| Jabbari et al. [93] (2003) | IV | Case Report | 2 | Spinal cord injury | Subcutaneously/into the area of burning pain and allodynia (16 to 20 sites)/BoNT/A, 5 IU per site | Significant improvement in VAS (burning pain and allodynia lasting at least three months) |
| Han et al. [94] (2014) | IV | Case Report | 1 | Spinal cord injury | Subcutaneously/into 10 most painful sites of each sole/BoNT/A/20 IU per site | Reduction in VAS from 96 mm to 68 mm and decreased intensity of the paroxysmal bursts VAS 23 mm after eight weeks |
BoNT/A: botulinum toxin type A; CRPS: complex regional pain syndrome; VAS: visual analog scale.
5.1. Post-Herpetic Neuralgia
To examine the direct analgesic effect of BoNT/A, Ranoux et al. conducted a randomized, double-blind, placebo-controlled study of 29 patients with focal painful neuropathies [16]. This study included four patients with postherpetic neuralgia; the remainder had post-traumatic/post-operative neuropathies. They received intradermal injections of BoNT/A of between 20 and 190 units into the painful area. After the injections, pain intensity decreased, allodynia to brushing improved, and pain thresholds to cold were reduced [16]. Later, a randomized, placebo-controlled, double-blind study was conducted on 60 patients with PHN [18]. In this class I study, the patients reported significant pain relief after subcutaneous BoTN/A injection compared with injections of placebo and lidocaine. Pain began to subside three to five days after the injection, and the mean visual analog scale (VAS) score was reduced by 4.5 compared with the placebo group (2.9) [18]. Recently, 30 adults with PHN were randomly divided into BoNT/A and placebo groups in a parallel, randomized, double-bind, single-dose, controlled human study by Apalla et al. [67]. In this class I study, a total of 100 units of BoNT/A was injected subcutaneously all over each affected area in a chessboard-like pattern. Thirteen patients showed a significant VAS score reduction of at least 50% from the baseline. This significant reduction lasted for a median period of 16 weeks [67]. There have been earlier case reports on the antinociceptive effects of BoNT/A in PHN; Liu et al. reported that after the injection of BoNT/A into an allodynia lesion of a PHN patient, the patient’s VAS gradually decreased from a score of 10 to a score of 1; the effect persisted for 52 days [68]. In 2009, Sotiriu et al. reported similar results in a case series of three PHN patients [69]. These patients were treated with subcutaneous BoNT/A injections over their affected areas. Their mean VAS score decreased from 8.3 to 2 after two weeks and increased to 4 after three months. In summary, there are two class I studies that show the efficacy of the antinociceptive effects of BoNT/A when used as a treatment for PHN [18,67].
5.2. Trigeminal Neuralgia
Wu et al. evaluated 42 patients with trigeminal neuralgia in a randomized, double-blind, placebo-controlled study: 22 were treated with BoNT/A, and 20 were treated with a placebo [70]. In this class I study, 75 units of BoNT/A were injected either intradermally or submucosally into the painful areas of each patient in the intervention group. Of the patients administered BoNT/A injections, 68.18% reported more than a 50% reduction in pain intensity on the VAS compared with 15% in the placebo group.
Turk et al. conducted a class IV, open-ended study to investigate the effectiveness of administering BoNT/A to patients with trigeminal neuralgia [73]. Eight patients were injected with 100 units of BoNT/A in the area around the zygomatic arch, and all of the patients experienced beneficial effects. In a class IV, open-label study, 13 patients with idiopathic trigeminal neuralgia were transcutaneously injected with BoNT/A at the trigeminal nerve branches [57]. Four patients were pain-free, and nine patients reported more than a 50% reduction in pain intensity as measured by VAS score, which lasted for 60 days. Borodic et al. conducted a class IV, open-label pilot study; 44 patients with chronic facial pain were treated with BoNT injections into the painful area, and the diagnoses included temporomandibular joint syndrome, idiopathic trigeminal neuralgia, and post-surgical pain syndrome, among others [75]. Eleven patients with idiopathic trigeminal neuralgia were transcutaneously injected with 25–75 units of BoNT/A. Eight patients reported at least a 50% reduction in pain frequency and intensity, and these beneficial effects lasted for 2–4 months.
In another class IV, open-label study, 20–50 units of BoNT/A were subcutaneously injected into trigger zones in 12 patients with idiopathic trigeminal neuralgia [72]. If mandibular muscles were involved, additional injections were performed in master muscles. Ten patients showed significant improvements in pain based on VAS scores, which lasted for 60 days. At eight weeks post injection, the cumulative mean pain score on the VAS was reduced from 8.83 to 4.08. The number of paroxysmal attacks of pain per 24 h period decreased from 23.4 to 8.8. Similar results were observed in a class IV, open-label study by Bohluli et al., in which 15 patients with trigeminal neuralgia were injected with BoNT/A in their trigger zones [71]. In this study, it was not specified whether the mode of injection was subcutaneous or intradermal. All 15 patients showed improvements in pain frequency and severity after the intervention, which lasted for up to six months. The frequency of attacks per day reduced from 33 to 8; seven patients reported complete eradication of pain after the injection.
There have been several case reports with similar successful results. Both Ngeow and Nair and Allam et al. reported cases that exhibited reduced pain after subcutaneous injections of BoNT/A into painful areas [76,78]. In a case report by Yoon et al., BoNT/A was subcutaneously injected into the area surrounding the middle of the chin [77]. The size of the painful area was reduced after one month, and there was a slight pain reduction after two months.
There have been a few case reports and open-label studies, including several class IV studies, that report the beneficial effects of BoNT/A injections for the management of trigeminal neuralgia, but there is only one class I study [70]. BoNT/A injection is likely effective for trigeminal neuralgia, but well-designed, randomized, controlled, double-blind trials are still necessary to investigate the therapeutic efficacy of BoNT/A for trigeminal neuralgia.
5.3. Post-Traumatic Neuralgia or Post-Surgical Neuralgia
As mentioned in Section 5.1, Ranoux and colleagues conducted a randomized, double-blind, placebo-controlled study that evaluated eight patients with post-traumatic neuralgia, 17 patients with post-surgical neuralgia, and four patients with postherpetic [16]. In this class I study, BoNT injections were effective at reducing neuropathic pain. The patients were evaluated at baseline and at 4, 12 and 24 weeks after BoNT injection. The patients showed significantly reduced brush allodynia, non-evoked pain, and cold allodynia. There were no changes in their responses to thermal or mechanical pain. These effects began two weeks after the injection and lasted for up to 24 weeks.
In a randomized, placebo-controlled study, 48 patients were injected with 100 units of BoNT/A before mastectomy into the pectoralis major, serratus anterior, and rectus abdominis muscles [79]. In this class IV study, post-surgical pain was significantly reduced, and more pain medication was used by the patients in the placebo group than those in the intervention group. BoNT is likely effective as a treatment for post-traumatic and post-surgical neuralgia, but another well-organized, randomized study is necessary to confirm this conclusion.
5.4. Diabetic Neuropathy
Yuan et al. concluded that BoNT/A can be an effective treatment for painful diabetic neuropathy based on the results of a randomized, double-blind, placebo-controlled study [17]. In this class II study, there was a significant decrease in the VAS score of a treatment group that included 18 patients with diabetic neuropathy at 1, 4, 8 and 12 weeks (p < 0.05). The antinociceptive effects lasted for up to 12 weeks. Additionally, there was improvement in the scores of a Chinese version of the Pittsburgh Sleep Quality Index four weeks after the injection [17]. Furthermore, Chen and Yuan et al. conducted another study that suggested the possibility that tactile and mechanical pain reception might be improved by BoNT/A injection in patients with diabetic polyneuropathy [95].
In 2014, a randomized, double-blind, placebo-controlled clinical trial was performed on diabetic patients [95]. In this class I study, the patients were diagnosed with diabetic neuropathy using the Douleur Neuropathique 4 (DN4) questionnaire and nerve conduction studies. They were under 70 years old and presented with neuropathic pain in their feet. Forty patients were randomly assigned into two groups: the BoNT/A and placebo groups. One hundred units of BoNT/A were injected into each patient in the intervention group, and normal saline was injected into the other 20 patients. After the BoNT/A injections, the patients’ neuropathy pain scale (NPS) scores were reduced for all items except cold sensation (p < 0.01). Their DN4 scores also decreased, which were related to electric shocks, pins and needles, and burning and brushing (p < 0.05). According to the class I and class II studies described above [17,80], BoNT is likely effective as a treatment for diabetic neuropathy.
5.5. Occipital Neuralgia
Kapural et al. retrospectively analyzed a case series of six patients with occipital neuralgia who received occipital nerve blocks with 50 units of BoNT/A [81]. VAS scores were significantly reduced, and the pain disability index improved in five out of the six patients at four weeks after the BoNT/A injection. The patients reported long-lasting pain relief, which persisted for more than four months in five patients.
In a prospective, open-label, pilot study by Taylor et al., 50 units of BoNT/A were injected inferolaterally into the occipital protuberance in six patients with occipital neuralgia [82]. The patients reported daily ratings of their headache types based on the Visual Analog Pain and Medication Use Diary and recorded their dosages of daily pain medication for 12 weeks after the injection. The authors found that both sharp/shooting and pins/needles types of headache pain significantly improved over the baseline at various time points. Pins/needles pain improved over baseline with statistical significance at 3–6 weeks, whereas sharp/shooting pain improved during weeks 2–3 and 7–12. However, there was no significant improvement in dull/aching pain. None of the patients reported a cessation of their headaches after being injected, and there were no changes in pain medication dosage.
As there have been only two class IV studies examining BoNT/A as a treatment for occipital neuralgia, there is currently insufficient evidence to prove its efficacy in alleviating this condition.
5.6. Carpal Tunnel Syndrome
In a randomized, double-blind, placebo-controlled study by Breuer et al., 20 patients were included who had been diagnosed with carpal tunnel syndrome by nerve conduction studies [83]. In this class I study, the patients were randomly assigned and received either BoNT/B or normal saline via intramuscular injection into their hypothenar muscles. The patients were monitored every week for 13 weeks for pain severity based on the VAS score and for opiate usage. The authors found that BoNT/B injection produced no beneficial effects in patients with carpal tunnel syndrome with respect to pain or quality of life compared with the normal saline group.
Tsai et al. conducted a prospective, open-label case series that included five females with carpal tunnel syndrome [84]. A total of 30 units of BoNT/A were injected intracarpally on each side of the carpal tunnel. Three out of five patients reported insignificant pain improvement at three months, without electrophysiological changes. According to this class I negative study and the one class IV study with positive results, there is insufficient evidence to prove the efficacy of BoNT as a treatment for carpal tunnel syndrome [83,84]. In both studies, BoNT was delivered differently than in other studies: It was either intramuscularly or intracarpally injected. Thus, the negative results of these studies might be influenced by the mode of administration.
5.7. Complex Regional Pain Syndrome
Safarpour and colleagues conducted a randomized, prospective, double-blind, placebo-controlled, open-label extension study; they observed that subcutaneous and intradermal injections of 5 units/site of BoNT/A (40 to 200 units total) into allodynic areas of patients with complex regional pain syndrome (CRPS) were not effective at reducing pain [85]. There were no differences between the intervention and placebo groups. This study was prematurely terminated due to intolerance of the BoNT/A injection.
A randomized, double-blind, placebo-controlled crossover study was conducted to further investigate the antinociceptive effect of BoNT in CRPS patients [86]. Lumbar sympathetic blocks with BoNT/A were performed instead of peripheral application. Pain was relieved for a significantly prolonged period (71 days) in the treatment group, who were administered a combination of local anesthetics and BoTN/A, compared with a group who was administered anesthetic alone (10 days).
Open-label studies have shown pain relief and improvements in skin color and edema in patients with CRPS. In a study by Argoff, 11 patients with CRPS were injected with 300 units of BoNT/A into the muscles in which the patients complained of feeling maximal pain [54]. Each muscle was subcutaneously injected with between 25–50 units of BoNT/A. After 6–12 weeks, all of the patients reported reduced burning sensations and dysesthetic pain in their affected extremities, with normalized skin and decreased edema. Safarpour and Jabbari reported two cases with CRPS who presented with proximal myofascial pain that responded to BoNT/A [88]. These patients had proximal myofascial pain syndromes in the ipsilateral side to the distal painful limb. After BoNT/A injections into trigger points in the proximal muscles, both the proximal pain of myofascial pain syndrome and the distal painful symptoms of CPRS were improved.
Thirty-seven patients with dystonia or spasm in the neck or upper limb girdle muscles were reviewed in a retrospective, unblinded, uncontrolled study [87]. Local pain scores were measured four weeks after intramuscular injections of BoNT/A (10–20 units per muscle) were performed. The mean pain score was reduced by 43% and 97% of the patients reported a reduction in pain.
5.8. Residual Limb Pain or Phantom Limb Pain
In a prospective, randomized, double-blind pilot study, 14 amputee patients with residual limb pain were intramuscularly, intraneuronally, or subcutaneously injected into painful sites with either 250 to 300 units of BoNT/A or with a combination of lidocaine and depomedrol [89]. The patients were evaluated for residual limb pain and phantom limb pain using the VAS, both at baseline and during each month after the injection for six months. Compared with baseline, both the BoNT/A and lidocaine/depomedrol groups showed immediate improvements in residual limb pain and pain tolerance. These effects lasted for six months in both of the groups, but there were no changes in phantom limb pain.
There was a case report that the antinociceptive effect of BoNT/A was effective in reducing phantom limb pain for over 12 months [91]. BoNT/A was injected into the trigger points of the stump of a lower limb amputee with phantom limb pain. The injections were repeated four times at three-month intervals. The patient’s pain improved, and his dose of intrathecal morphine therapy was reduced to 40% of the initial dose. Intrathecal clonidine and other oral pain medications were completely ceased.
5.9. Miscellaneous
In addition to the previously mentioned sections, there have been studies showing the efficacy of using BoNT/A to treat other conditions that include neuropathic pain. There was a case report that neuropathic pain caused by a keloid was successfully treated with BoNT/A injection [92]. After two surgeries, an 80-year-old woman complained of a painful chest wall scar that produced a burning, stinging sensation and allodynia [96]; she was injected with a total of 100 units of BoNT/A, and after five weeks, her pain reduced from 8 to generally 6 and intermittently to 0 out of 10 on the numeric pain scale. There was another case report that BoNT/A was effective at reducing chronic post-thoracotomy pain [79]. A 67-year-old man who had a thoracotomy scar with a predominantly neuropathic component was treated with 100 units of BoNT/A. After two weeks, he reported an improvement in his pain. His VAS score dropped from 6 to 1, and these effects persisted for more than 12 weeks.
There have been several case reports on using BoNT/A to treat neuropathic pain related to spinal cord injury. Jabbari et al. reported two patients with burning pain and allodynia from a spinal cord lesion. Both patients had cervical spinal cord injuries and complained of skin sensitivity and burning pain in the dermatome [93]. The burning pain was significantly lessened after BoNT/A was injected into multiple points over each patient’s painful area. Han et al. also reported a case with intractable neuropathic pain with a VAS of 96 mm, which was caused by spinal cord injury [94]. The patient reported significant pain relief after 20 units of BoNT/A were injected into the 10 most painful sites on each sole. The patient’s VAS decreased from 96 to 23 mm.
6. Administration Routes and Dosage
There are currently no guidelines for the proper mode of administration or dosage of BoNT injection when used as a treatment for neuropathic pain. However, in this review, the above-mentioned injection techniques primarily include either intradermal or subcutaneous injections into painful areas. However, in a study by Breuer et al., BoNT was injected intramuscularly [83]. The results of this study showed no beneficial effects in patients with carpal tunnel syndrome. This mode of administration might have hindered the antinociceptive efficacy of BoNT. In a study by Tsai et al., BoNT was injected intracarpally [84]; the results of this study might also be limited by the route of administration. The mode of administration might play an important role, as BoNT enters into neurons by binding to the synaptic vesicle protein 2 (SV2) receptor [97]. After binding to the SV2 receptor on the membrane, BoNT/A endocytosis proceeds, and BoNT/A is processed in the acidic compartments of small synaptic vesicles.
In the above-reviewed studies, diverse dosages were used; 2.5 to 50 units per point of BoNT were subcutaneously or intrademally injected over 1–40 sites with a total dosage of 6–300 units. Ranoux et al. intradermally injected five units using a grid pattern over the painful area, with a maximum dose of 200 units [16]. Liu et al. subcutaneously injected BoNT/A over the painful area in a fanning manner, dividing the injections into 20 routes, using five units per route and a maximal dose of 100 units into the area of allodynia [68]. Xiao et al. performed subcutaneous injections within 1–2 cm over the area of allodynia, using a maximum of 40 injection sites and depositing five units per site [18]. In a study by Yuan et al., intradermal BoNT/A injections were applied to the foot dorsum in a grid-like distribution pattern, with four units injected per site and 50 units injected per foot [17]. For the treatment of trigeminal neuralgia, Piovesan et al. subdermally injected three units per point in a grid-like pattern [74]. Ngeow and Nair performed subcutaneous injections into two trigger zones over the painful area; a total dose of 100 units was used [76]. There was also a report of a lumbar sympathetic block by Carroll et al., who administered 75 units of BoNT/A mixed with bupivacaine [86]. Further studies on what the effective dosages of BoNT/A are must be conducted.
7. Potential Adverse Effects
BoNT/A has a high safety profile with few reported irreversible medical adverse effects [98,99]. When a small amount of BoNT/A enters the circulatory system, systemic or regional complications can be produced such as antibody formation and possible immune-related complications. However, to develop antibodies, large amounts of BoNT are required, and amounts of ideal dosages of BoNT for neuropathic pain are not yet known. [98,100,101]
There are trials to measure the safety of BoNT/A for each neuropathic pain disease. For example, Lakhan et al. published an article which was a meta-analysis of two studies using BoNT/A for neuropathic pain, especially painful diabetic neuropathy [102]. In their article, there was only one adverse effect, the infection of an injection site, which was not statistically significant. For chronic migraines, according to the Phase III REsearch Evaluating Migraine Prophylaxis Therapy (PREEMPT) clinical study by Aurora et al., there were more adverse events in the BoNT/A group (28.5%) than the placebo group (12.4%) [103]. The most frequently reported side effect in the BoNT/A group included neck pain (4.3%), injection site pain (2.1%), eyelid ptosis (1.9%), and muscular weakness (1.6%). These adverse effects are consistent with the previously reported adverse events from 24-week double-blind and 56-week PREEMPT clinical trials [12,103,104]. In this study, the rate of adverse events decreased progressively as additional injections were done, suggesting cumulative benefits of continued prophylaxis.
8. Conclusions
BoNT has become more widely used for the treatment of neuropathic pain. To investigate the antinociceptive effects of BoNT, we assessed levels of evidence from clinical and experimental studies according to the American Academy of Neurology guidelines. According to our assessments, recent studies suggest that BoNT injection is effective as a treatment for postherpetic neuralgia and is likely effective in treating trigeminal neuralgia and post-traumatic neuralgia. BoNT may be effective as a treatment for diabetic neuropathy. Its efficacy has not been proven for the treatment of occipital neuralgia or complex regional pain syndrome.
Author Contributions
Hyun-Mi Oh and Myung Eun Chung worked collaboratively on all aspects of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kao, I.; Drachman, D.B.; Price, D.L. Botulinum toxin: Mechanism of presynaptic blockade. Science 1976, 193, 1256–1258. [Google Scholar] [CrossRef] [PubMed]
- Blersch, W.; Schulte-Mattler, W.J.; Przywara, S.; May, A.; Bigalke, H.; Wohlfarth, K. Botulinum toxin A and the cutaneous nociception in humans: A prospective, double-blind, placebo-controlled, randomized study. J. Neurol. Sci. 2002, 205, 59–63. [Google Scholar] [CrossRef]
- Thenganatt, M.A.; Fahn, S. Botulinum toxin for the treatment of movement disorders. Curr. Neurol. Neurosci. Rep. 2012, 12, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Pellizzari, R.; Rossetto, O.; Schiavo, G.; Montecucco, C. Tetanus and botulinum neurotoxins: Mechanism of action and therapeutic uses. Philos. Trans. R. Soc. Lond. B Biol. Sci. 1999, 354, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Simpson, L.L. The origin, structure, and pharmacological activity of botulinum toxin. Pharmacol. Rev. 1981, 33, 155–188. [Google Scholar] [PubMed]
- Mense, S. Neurobiological basis for the use of botulinum toxin in pain therapy. J. Neurol. 2004, 251, I1–I7. [Google Scholar] [CrossRef] [PubMed]
- Verderio, C.; Grumelli, C.; Raiteri, L.; Coco, S.; Paluzzi, S.; Caccin, P.; Rossetto, O.; Bonanno, G.; Montecucco, C.; Matteoli, M. Traffic of botulinum toxins A and E in excitatory and inhibitory neurons. Traffic 2007, 8, 142–153. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.R. Review of a Proposed Mechanism for the Antinociceptive Action of Botulinum Toxin Type A. Neurotoxicology 2005, 26, 785–793. [Google Scholar] [CrossRef] [PubMed]
- Jeynes, L.C.; Gauci, C.A. Evidence for the use of botulinum toxin in the chronic pain setting: A review of the literature. Pain Pract. 2008, 8, 269–276. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.R. Future aspects of botulinum neurotoxins. J. Neural. Trans. 2008, 115, 567–573. [Google Scholar] [CrossRef] [PubMed]
- Cui, M.; Khanijou, S.; Rubino, J.; Aoki, K.R. Subcutaneous administration of botulinum toxin A reduces formalin-induced pain. Pain 2004, 107, 125–133. [Google Scholar] [CrossRef] [PubMed]
- Dodick, D.W.; Turkel, C.C.; de Gryse, R.E.; Aurora, S.K.; Silberstein, S.D.; Lipton, R.B.; Diener, H.C.; Brin, M.F. OnobotulinumtoxinA for treatment of chronic migraine: Pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program. Headache 2010, 50, 921–936. [Google Scholar] [CrossRef] [PubMed]
- Berry, M.G.; Stanek, J.J. Botulinum neurotoxin A: A review. J. Plast. Reconstr. Aesthet. Surg. 2012, 65, 1283–1291. [Google Scholar] [CrossRef] [PubMed]
- Burstein, R.; Zhang, X.; Levy, D.; Aoki, K.R.; Brin, M.F. Selective inhibition of meningeal nociceptors by botulinum neurotoxin type A: Therapeutic implications for migraine and other pains. Cephalalgia 2014, 34, 853–869. [Google Scholar] [CrossRef] [PubMed]
- Jansen, T.S.; Baron, R.; Haanpaa, M.; Kalso, E.; Loeser, J.D.; Rice, A.S.; Treede, R.D. A new definition of neuropathic pain. Pain 2011, 152, 2204–2205. [Google Scholar] [CrossRef] [PubMed]
- Ranoux, D.; Attal, N.; Morain, F.; Bouhassira, D. Botulinum toxin type A induces direct analgesic effects in chronic neuropathic pain. Ann. Neurol. 2008, 64, 274–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yuan, R.Y.; Sheu, J.J.; Yu, J.M.; Chen, W.T.; Tseng, I.J.; Change, H.H.; Hu, C.J. Botulinum toxin for diabetic neuropathic pain: A randomized double-blind crossover trial. Neurology 2009, 72, 1473–1478. [Google Scholar] [CrossRef] [PubMed]
- Xiao, L.; Mackey, S.; Hui, H.; Xong, D.; Zhang, Q.; Zhang, D. Subcutaneous injection of botulinum toxin A is beneficial in postherpetic neuralgia. Pain Med. 2010, 11, 1827–1833. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.H.; Shin, T.J.; Kim, H.J.; Lee, J.K.; Suh, H.W.; Lee, S.C.; Seo, K. Intrathecal administration of botulinum neurotoxin type A attenuates formalin-induced antinociceptive responses in mice. Anesth. Analg. 2011, 112, 228–235. [Google Scholar] [CrossRef] [PubMed]
- Welch, M.J.; Purkiss, J.R.; Foster, K.A. Sensitivity of embryonic rat dorsal root ganglia neurons to Clostridium botulinum neurotoxins. Toxicon 2000, 38, 245–258. [Google Scholar] [CrossRef]
- Durham, P.L.; Cady, R. Regulation of calcitonin gene-related peptide secretion from trigeminal nerve cells by botulinum toxin type A: Implications for migraine therapy. Headache 2004, 44, 35–42. [Google Scholar] [CrossRef] [PubMed]
- Argoff, C.E. The use of botulinum toxins for chronic pain and headaches. Curr. Treat. Options Neurol. 2003, 5, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Morenilla-Palao, C.; Planells-Cases, R.; Garcia-Sanz, N.; Ferrer-Montiel, A. Regulated exocytosis contributes to protein kinase C potentiation of vanilloid receptor activity. J. Biol. Chem. 2004, 279, 25665–25672. [Google Scholar] [CrossRef] [PubMed]
- Cheng, J.; Liu, W.; Duffney, L.J.; Yan, Z. SNARE proteins are essential in the potentiation of NMDA receptors by group II metabotropic glutamate receptors. J. Physiol. 2013, 591, 3935–3947. [Google Scholar] [CrossRef] [PubMed]
- McMahon, H.T.; Foran, P.; Dolly, J.O.; Verhage, M.; Wiegant, V.M.; Nicholls, D.G. Tetanus toxin and botulinum toxins type A and B inhibit glutamate, F-aminobutyric acid, aspartate, and met-enkephalin release from synaptosomes. J. Biol. Chem. 1992, 267, 21338–21343. [Google Scholar] [PubMed]
- Luvisetto, S.; Marinelli, S.; Lucchetti, F.; Marchi, F.; Cobianchi, S.; Rossetto, O.; Montecucco, C.; Pavone, F. Botulinum neurotoxins and formalin-induced pain: Central vs. peripheral effects in mice. Brain Res. 2006, 1082, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Paterson, K.; Lolignier, S.; Wood, J.N.; McMahon, S.B.; Bennett, D.L. Botulinum toxin-A treatment reduces human mechanical pain sensitivity and mechanotransduction. Ann. Neurol. 2014, 75, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Drew, L.J.; Rugiero, F.; Cesare, P.; Gale, J.E.; Abrahamsen, B.; Bowden, S.; Heinzmann, S.; Robinson, M.; Brust, A.; Colless, B.; et al. High-threshold mechanosensitive ion channels blocked by a novel conopeptide mediate pressure-evoked pain. PLoS ONE 2007, 2, e515. [Google Scholar] [CrossRef] [PubMed]
- Di Castro, A.; Drew, L.J.; Wood, J.N.; Cesare, P. Modulation of sensory neuron mechanotransduction by PKC- and nerve growth factor-dependent pathways. Proc. Natl. Acad. Sci. USA 2006, 103, 4699–4704. [Google Scholar] [CrossRef] [PubMed]
- Tsui, J.K.; Eisen, A.; Stoessl, A.J.; Calne, S.; Calne, D.B. Double-blind study of botulinum toxin in spasmodic torticollis. Lancet 1986, 2, 245–247. [Google Scholar] [CrossRef]
- Stell, R.; Thompson, P.D.; Marsden, C.D. Botulinum toxin in spasmodic torticollis. J. Neurol. Neurosurg. Psychiatry 1988, 51, 920–923. [Google Scholar] [CrossRef] [PubMed]
- Aoki, K.R. Evidence for antinociceptive activity of botulinum toxin type A in pain management. Headache 2003, 43, S9–S15. [Google Scholar] [CrossRef] [PubMed]
- Freund, B.; Schwartz, M. Temporal relationship of muscle weakness and pain reduction in subjects treated with botulinum toxin A. J. Pain 2003, 4, 159–165. [Google Scholar] [CrossRef] [PubMed]
- Relja, M.; Klepac, N. Different doses of botulinum toxin A and pain responsiveness in cervical dystonia. Neurology 2002, 58, A474. [Google Scholar]
- Xiao, L.; Cheng, J.; Dai, J.; Zhang, D. Botulinum Toxin Decreases Hyperalgesia and Inhibits P2X3 Receptor Over-Expression in Sensory Neurons Induced by Ventral Root Transection in Rats. Pain Med. 2011, 12, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- McCormick, Z.; Chang-Chien, G.; Marshall, B.; Huang, M.; Harden, R.N. Phantom limb pain: A systematic neuroanatomical-based review of pharmacologic treatment. Pain Med. 2014, 15, 292–305. [Google Scholar] [CrossRef] [PubMed]
- Qerama, E.; Fuglsang-Frederiksen, A.; Jensen, T.S. The role of botulinum toxin in management of pain: An evidence-based review. Curr. Opin. Anaesthesiol. 2010, 23, 602–610. [Google Scholar] [CrossRef] [PubMed]
- Matak, I.; Lackovic, Z. Botulinum toxin A, brain and pain. Prog. Neurobiol. 2014, 119–120, 39–59. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Meng, J.; Lawrence, G.W.; Zurawski, T.H.; Sasse, A.; Bodeker, M.O.; Gilmore, M.A.; Fernández-Salas, E.; Francis, J.; Steward, L.E.; et al. Novel chimeras of botulinum neurotoxins A and E unveil contributions from the binding, translocation, and protease domains to their functional characteristics. J. Biol. Chem. 2008, 283, 16993–17002. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zurawski, T.H.; Meng, J.; Lawrence, G.W.; Aoki, K.R.; Wheeler, L.; Dolly, J.O. Novel chimeras of botulinum and tetanus neurotoxins yield insights into their distinct sites of neuroparalysis. FASEB J. 2012, 26, 5035–5048. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zurawski, T.H.; Bodeker, M.O.; Meng, J.; Boddul, S.; Aoki, K.R.; Dolly, J.O. Longer-acting and highly potent chimaeric inhibitors of excessive exocytosis created with domains from botulinum neurotoxin A and B. Biochem. J. 2012, 444, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Restani, L.; Antonucci, F.; Gianfranceschi, L.; Rossi, C.; Rossetto, O.; Caleo, M. Evidence for anterograde transport and transcytosis of botulinum neurotoxin A (BoNT/A). J. Neurosci. 2011, 31, 15650–15659. [Google Scholar] [CrossRef] [PubMed]
- Antonucci, F.; Rossi, C.; Gianfrancesci, L.; Rosetto, O.; Calleo, M. Long-distance retrograde effects of botulinum neurotoxin A. J. Neurosci. 2008, 28, 3689–3696. [Google Scholar] [CrossRef] [PubMed]
- Bach-Rojecky, L.; Lackovic, Z. Central origin of the antinociceptive action of botulinum toxin type A. Parmacol. Biochem. Behav. 2009, 94, 234–238. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bach-Rojecky, L.; Salkovic-Petrisic, M.; Lackovic, Z. Botulinum toxin type A reduces pain supersensitivity in experimental diabetic neuropathy: Bilateral effects after unilateral injection. Eur. J. Pharmacol. 2010, 633, 10–14. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Favre-Guilmard, C.; Auguet, M.; Chabrier, P.E. Different antinociceptive effects of botulinum toxin type A in inflammatory and peripheral polyneuropathic rat models. Eur. J. Pharmacol. 2009, 617, 48–53. [Google Scholar] [CrossRef] [PubMed]
- Wiegand, H.; Erdmann, G.; Wellhoner, H.H. 125I-labelled botulinum A neuro-toxin: Pharmacokinetics in cats after intramuscular injection. Naunyn Schmie Arch. Pharmacol. 1976, 292, 161–165. [Google Scholar] [CrossRef]
- Tang-Liu, D.D.; Aoki, K.R.; Dolly, J.O.; de Paiva, A.; Houchen, T.L.; Chasseaud, L.F.; Webber, C. Intramuscular injection of 125I-botulinum neurotoxin-com-plex vs. 125I-botulinum-free neurotoxin: Time course of tissue distribution. Toxicon 2003, 42, 461–469. [Google Scholar] [CrossRef]
- Filipovic, B.; Matak, I.; Bach-Rojecky, L.; Lackovic, Z. Central action of peripherally applied botulinum toxin type A on pain and dural protein extravasation in rat model of trigeminal neuropathy. PLoS ONE 2012, 7, e29803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matak, I.; Bach-Rojecky, L.; Filipovic, B.; Lackovic, Z. Behavioral and immunohistochemical evidence for central antinociceptive activity of botulinum toxin A. Neuroscience 2011, 186, 201–207. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marinelli, S.; Vacca, V.; Ricordy, R.; Uggenti, C.; Tata, A.M.; Luvisetto, S.; Pavone, F. The analgesic effect on neuropathic pain of retrogradely transported botulinumneurotoxin A involves Schwann cells and astrocytes. PLoS ONE 2012, 7, e47977. [Google Scholar] [CrossRef] [PubMed]
- Marino, M.J.; Terashima, T.; Steinauer, J.J.; Eddinger, K.A.; Yaksh, T.L.; Xu, Q. Botulinum toxin B in the sensory afferent: Transmitter release, spinal activation, and pain behavior. Pain 2014, 155, 674–684. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Shan, X.F.; Cong, X.; Yang, N.Y.; Wu, L.L.; Yu, G.Y.; Zhang, Y.; Cai, Z.G. Pre- and Post-synaptic Effects of Botulinum Toxin A on Submandibular Glands. J. Dent. Res. 2015. [Google Scholar] [CrossRef] [PubMed]
- Argoff, C.E. Botulinum toxin type A treatment of myofascial pain in patients with CRPS Type 1 (reflex sympathetic dystrophy): A pilot study. In Proceedings of the World Pain Congress (IASP) Meeting, Vienna, Austria, 22–27 August 1999.
- Chuang, Y.C.; Yoshimura, N.; Huang, C.C.; Wu, M.; Chiang, P.H.; Chancellor, M.B. Intraprostatic botulinum toxin a injection inhibits cyclooxygenase-2 expression and suppresses prostatic pain on capsaicin induced prostatitis model in rat. J. Urol. 2008, 180, 742–748. [Google Scholar] [CrossRef] [PubMed]
- Namazi, H. Intravesical botulinum toxin A injections plus hydrodistension can reduce nerve growth factor production and control bladder pain in interstitial cystitis: A molecular mechanism. Urology 2008, 72, 463–464. [Google Scholar] [CrossRef] [PubMed]
- Bach-Rojecky, L.; Dominis, M.; Lackovic, Z. Lack of anti-inflammatory effects of botulinum toxin A in experimental models of inflammation. Fundam. Clin. Pharmacol. 2008, 22, 503–509. [Google Scholar] [CrossRef] [PubMed]
- Tugnoli, V.; Capone, J.G.; Eleopra, R.; Quatrale, R.; Sensi, M.; Gastaldo, E.; Tola, M.R.; Geppetti, P. Botulinum toxin type A reduces capsaicin-evoked pain and neurogenic vasodilatation in human skin. Pain 2007, 130, 76–83. [Google Scholar] [CrossRef] [PubMed]
- Francisco, G.E.; Tan, H.; Green, M. Do botulinum toxins have a role in the management of neuropathic pain? A focused review. Am. J. Phys. Med. Rehabil. 2012, 91, 899–909. [Google Scholar] [CrossRef] [PubMed]
- Zieglgänsberger, W.; Berthele, A.; Tölle, T.R. Understanding neuropathic pain. CNS Spectr. 2005, 10, 298–308. [Google Scholar] [PubMed]
- Bach-Rojecky, L.; Relja, M.; Lackovic, Z. Botulinum toxin type A in experimental neuropathic pain. J. Neural. Trans. 2005, 112, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Drinovac, V.; Bach-Rojecky, L.; Matak, I.; Lackovic, Z. Involvement of μ-opioid receptors in antinociceptive action of botulinum toxin type A. Neuropharmacology 2013, 70, 331–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, H.J.; Lee, Y.; Lee, J.; Park, C.; Moon, D.E. The effects of botulinum toxin A on mechanical and cold allodynia in a rat model of neuropathic pain. Can. J. Anaesth. 2006, 53, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Luvisetto, S.; Marinelli, S.; Cobianchi, S.; Pavone, F. Anti-allodynic efficacy of botulinum neurotoxin A in a model of neuropathic pain. Neuroscience 2007, 145, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Marinelli, S.; Luvisetto, S.; Cobianchi, S.; Makuch, W.; Obara, I.; Mezzaroma, E.; Caruso, M.; Straface, E.; Przewlocka, B.; Pavone, F. Botulinum neurotoxin type A counteracts neuropathic pain and facilitates functional recovery after peripheral nerve injury in animal models. Neuroscience 2010, 171, 316–328. [Google Scholar] [CrossRef] [PubMed]
- Mika, J.; Rojewska, E.; Makuch, W.; Korostynski, M.; Luvisetto, S.; Marinelli, S.; Pavone, F.; Przewlocka, B. The effect of botulinum neurotoxin A on sciatic nerve injury-induced neuroimmunological changes in rat dorsal root ganglia and spinal cord. Neuroscience 2011, 175, 358–366. [Google Scholar] [CrossRef] [PubMed]
- Apalla, Z.; Sotiriou, E.; Lallas, A.; Lazaridou, E.; Ioannides, D. Botulinum toxin A in postherpetic neuralgia: A parallel, randomized, double-blind, single-dose, placebo-controlled trial. Clin. J. Pain 2013, 29, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.T.; Tsai, S.K.; Kao, M.C.; Hu, J.S. Botulinum toxin A relieved neuropathic pain in a case of post-herpetic neuralgia. Pain Med. 2006, 7, 89–91. [Google Scholar] [CrossRef] [PubMed]
- Sotiriu, E.; Apalla, Z.; Panagiotidou, D.; Ioannidis, D. Severe post-herpetic neuralgia successfully treated with botulinum toxin A: Three case reports. Acta Derm. Venereol. 2009, 89, 214–215. [Google Scholar]
- Wu, C.J.; Lian, Y.J.; Zheng, Y.K.; Zhang, H.F.; Chen, Y.; Xie, N.C.; Wang, L.J. Botulinum toxin type A for the treatment of trigeminal neuralgias: Results from a randomized, double-blind, placebo-controlled trial. Cephalgia 2012, 32, 443–450. [Google Scholar] [CrossRef] [PubMed]
- Bohluli, B.; Motamedi, M.H.; Bagheri, S.C.; Bayat, M.; Lassemi, E.; Navi, F.; Moharamnejad, N. Use of botulinum toxin A for drug-refractory trigeminal neuralgia: Preliminary report. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2011, 111, 47–50. [Google Scholar] [CrossRef] [PubMed]
- Zuniga, C.; Diaz, S.; Piedimonte, F.; Micheli, F. Beneficial effects of botulinum toxin type A in trigeminal neuralgia. Arq. Neuropsiquiatr. 2008, 66, 500–503. [Google Scholar] [CrossRef] [PubMed]
- Turk, U.; Ilhan, S.; Alp, R.; Sur, H. Botulinum toxin and intractable trigeminal neuralgia. Clin. Neuropharmacol. 2005, 28, 161–162. [Google Scholar] [PubMed]
- Piovesan, E.J.; Teive, H.G.; Kowacs, P.A.; Della Coletta, M.V.; Werneck, L.C.; Silberstein, S.D. An open study of botulinum-A toxin treatment of trigeminal neuralgia. Neurology 2005, 65, 1306–1308. [Google Scholar] [CrossRef] [PubMed]
- Borodic, G.E.; Acquadro, M.A. The use of botulinum toxin for the treatment of chronic facial pain. J. Pain 2002, 1, 21–27. [Google Scholar] [CrossRef]
- Ngeow, W.C.; Nair, R. Injection of botulinum toxin type A (BOTOX) into trigger zone of trigeminal neuralgia as a means to control pain. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2010, 109, e47–e50. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.H.; Merril, R.L.; Choi, J.H.; Kim, S.T. Use of botulinum toxin type A injection for neuropathic pain after trigeminal nerve injury. Pain Med. 2010, 11, 630–632. [Google Scholar] [CrossRef] [PubMed]
- Allam, N.; Brasil-Neto, J.P.; Brown, G.; Tomaz, C. Injections of botulinum toxin type A produce alleviation of intractable trigeminal neuralgia. Clin. J. Pain. 2005, 21, 182–184. [Google Scholar] [CrossRef] [PubMed]
- Layeeque, R.; Hochberg, J.; Siegel, E.; Kunkel, K.; Kepple, J.; Henry-Tillman, R.S.; Dunlap, M.; Seibert, J.; Klimberg, V.S. Botulinum toxin infiltration for pain control after mastectomy and expander reconstruction. Ann. Surg. 2004, 240, 608–613. [Google Scholar] [CrossRef] [PubMed]
- Ghasemi, M.; Ansari, M.; Basiri, K.; Shaigannejad, V. The effects of intradermal botulinum toxin type A injections on pain symptoms of patients with diabetic neuropathy. J. Res. Med. Sci. 2014, 19, 106–111. [Google Scholar] [PubMed]
- Kapural, L.; Stillman, M.; Kapural, M.; Mclntyre, P.; Guirgius, M.; Mekhail, N. Botulinum toxin occipital nerve block for the treatment of severe occipital neuralgia: A case series. Pain Pract. 2007, 7, 337–340. [Google Scholar] [CrossRef] [PubMed]
- Taylor, M.; Silva, S.; Cottrell, C. Botulinum toxin type A in the treatment of occipital neuralgia: A pilot study. Headache 2008, 48, 1476–1481. [Google Scholar] [CrossRef] [PubMed]
- Breuer, B.; Sperber, K.; Wallenstein, S.; Kiprovski, K.; Calapa, A.; Snow, B.; Pappagallo, M. Clinically significant placebo analgesic response in a pilot trial of botulinum B in patients with hand pain and carpel tunnel syndrome. Pain Med. 2006, 7, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Tsai, C.P.; Liu, C.Y.; Lin, K.P.; Wnag, K.C. Efficacy of botulinum toxin type A in the relief of carpal tunnel syndrome. Clin. Drug Investig. 2006, 26, 511–515. [Google Scholar] [CrossRef] [PubMed]
- Safarpour, D.; Salardini, A.; Richardson, D.; Jabbari, B. Botulinum toxin A for treatment of allodynia of complex regional pain syndrome: A pilot study. Pain Med. 2010, 11, 1411–1414. [Google Scholar] [CrossRef] [PubMed]
- Carroll, I.; Clark, J.D.; Mackey, S. Sympathetic block with botulinum toxin to treat complex regional pain syndrome. Ann. Neurol. 2009, 65, 348–351. [Google Scholar] [CrossRef] [PubMed]
- Kharkar, S.; Ambady, P.; Venkatesh, Y.; Schwartzman, R.J. Intramuscular botulinum toxin in complex regional pain syndrome: Case series and literature review. Pain Phys. 2011, 14, 419–424. [Google Scholar]
- Safarpour, D.; Jabbari, B. Botulinum toxin a (Botox) for treatment of proximal myofascial pain in complex regional pain syndrome: Two cases. Pain Med. 2010, 11, 1415–1418. [Google Scholar] [CrossRef] [PubMed]
- Wu, H.; Sultana, R.; Taylor, K.B.; Szabo, A. A prospective randomized double-blinded pilot study to examine the effect of botulinum toxin type A injection vs. Lidocaine/Depomedrol injection on residual and phantom limb pain. Clin. J. Pain 2012, 28, 108–112. [Google Scholar]
- Jin, L.; Kollewe, K.; Krampfl, K.; Dengler, R.; Mohammadi, B. Treatment of phantom limb pain with botulinum toxin type A. Pain Med. 2009, 10, 300–303. [Google Scholar] [PubMed]
- Kern, U.; Martin, C.; Scheicher, S.; Muler, H. Long-term treatment of phantom and stump pain with Botulinum toxin type A over 12 months. A first clinical observation. Nervenarzt 2004, 75, 336–340. [Google Scholar] [CrossRef] [PubMed]
- Uyesugi, B.; Lippincott, B.; Dave, S. Treatment of a painful keloid with botulinum toxin type A. Am. J. Phys. Med. Rehabil. 2010, 89, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Jabbari, B.; Maher, N.; Difazio, M.P. Botulinum toxin A improved burning pain and allodynia in two patients with spinal cord pathology. Pain Med. 2003, 4, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Han, Z.A.; Song, D.H.; Chung, M.E. Effect of subcutaneous injection of botulinum toxin A on spinal cord injury-associated neuropathic pain. Spinal Cord 2014, 52, S5–S6. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.T.; Yuan, R.Y.; Chiang, S.C.; Sheu, J.J.; Yu, J.M.; Tseng, I.J.; Yang, S.K.; Chang, H.H.; Hu, C.J. OnabotulinumtoxinA improves tactile and mechanical pain perception in painful diabetic polyneuropathy. Clin. J. Pain 2013, 29, 305–310. [Google Scholar] [CrossRef] [PubMed]
- Fabregat, G.; Asensio-Samper, J.M.; Palmisani, S.; Villanueva-Perez, V.L.; Andres, J.D. Subcuaneous botulinum toxin for chronic post-thoracotomy pain. Pain Pract. 2012, 13, 231–234. [Google Scholar] [CrossRef] [PubMed]
- Dong, M.; Yeh, F.; Tepp, W.H.; Dean, C.; Johnson, E.A.; Janz, R.; Chapman, E.R. SV2 is the protein receptor for botulinum neurotoxin A. Science 2006, 312, 592–596. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, A.; Kiene, K.; Carruthers, J. Botulinum A exotoxin use in clinical dermatology. J. Am. Acad. Dermatol. 1996, 34, 788–797. [Google Scholar] [CrossRef]
- Matarasso, S.L. Complications of botulinum A exotoxin for hyperfunctional lines. Dermatol. Surg. 1998, 24, 1249–1254. [Google Scholar] [CrossRef] [PubMed]
- Matarasso, A.; Deva, A.K. Botulinum toxin. Plast. Reconstr. Surg. 2002, 109, 1191–1197. [Google Scholar] [CrossRef] [PubMed]
- Lange, D.J.; Rubin, M.; Greene, P.E.; Kang, U.J.; Moskowitz, C.B.; Brin, M.F.; Lovelace, R.E.; Fahn, S. Distant effects of locally injected botulinum toxin: A double-blind study of single fiber EMG changes. Muscle Nerve 1991, 14, 672–675. [Google Scholar] [CrossRef] [PubMed]
- Lakhan, S.E.; Velasco, D.N.; Tepper, D. Botulinum Toxin-A for Painful Diabetic Neuropathy: A Meta-Analysis. Pain Med. 2015. [Google Scholar] [CrossRef] [PubMed]
- Aurora, S.K.; Dodick, D.W.; Diener, H.C.; de Gryse, R.E.; Turkel, C.C.; Lipton, R.B.; Silberstein, S.D. OnabotulinumtoxinA for chronic migraine: Efficacy, safety, and tolerability in patients who received all five treatment cycles in the PREEMPT clinical program. Acta Neurol. Scand. 2014, 129, 61–70. [Google Scholar] [CrossRef] [PubMed]
- Diener, H.C.; Dodick, D.W.; Aurora, S.K.; Turkel, C.C.; de Gryse, R.E.; Lipton, R.B.; Silberstein, S.D.; Brin, M.F.; PREEMPT 2 Chronic Migraine Study Group. OnabotulinumtoxinA for treatment of chronic migraine: Results from the double-blind, randomized, placebo-controlled phase of the PREEMPT 2 trial. Cephalalgia 2010, 30, 804–814. [Google Scholar] [CrossRef] [PubMed]
© 2015 by the authors; licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Oh, H.-M.; Chung, M.E. Botulinum Toxin for Neuropathic Pain: A Review of the Literature. Toxins 2015, 7, 3127-3154. https://doi.org/10.3390/toxins7083127
AMA Style
Oh H-M, Chung ME. Botulinum Toxin for Neuropathic Pain: A Review of the Literature. Toxins. 2015; 7(8):3127-3154. https://doi.org/10.3390/toxins7083127
Chicago/Turabian StyleOh, Hyun-Mi, and Myung Eun Chung. 2015. "Botulinum Toxin for Neuropathic Pain: A Review of the Literature" Toxins 7, no. 8: 3127-3154. https://doi.org/10.3390/toxins7083127