Effectiveness and Impact of the 4CMenB Vaccine against Group B Meningococcal Disease in Two Italian Regions Using Different Vaccination Schedules: A Five-Year Retrospective Observational Study (2014–2018)

 , , , , , and
, , , , , and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Setting
2.2. Vaccination Schedules and Coverage
2.3. Study Design
2.4. Case Definition
2.5. Laboratory Methods
2.6. Evaluation of Vaccine Effectiveness
VE = 1 1 − PCV
PPV
1 − PPV
2.7. Evaluation of Incidence and Impact of Vaccination
2.8. Statistical Analysis
3. Results
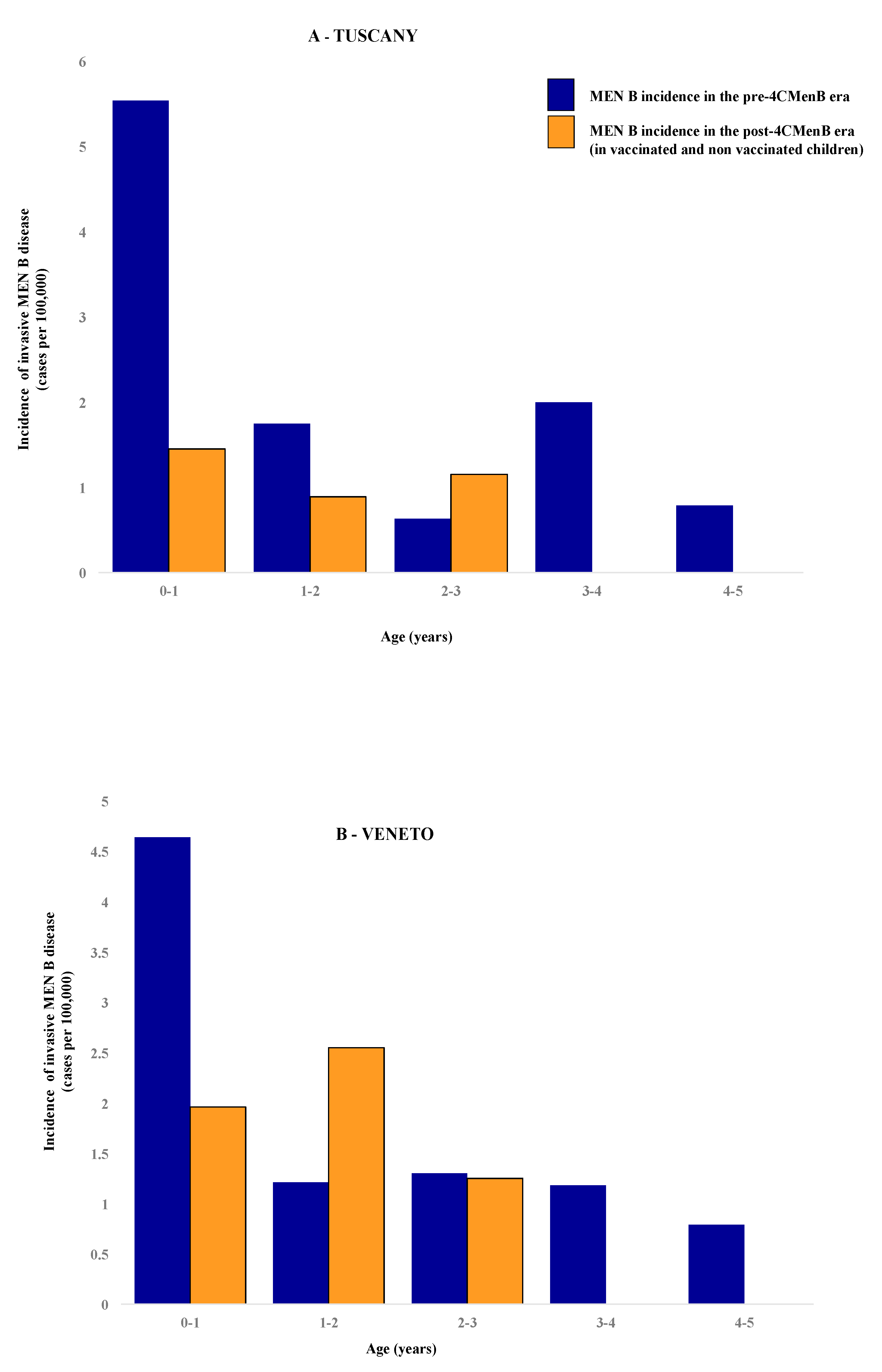
3.1. Incidence of Invasive Meningococcal Disease in Pre- and Post 4CMenB Era
3.2. Effectiveness of Vaccination
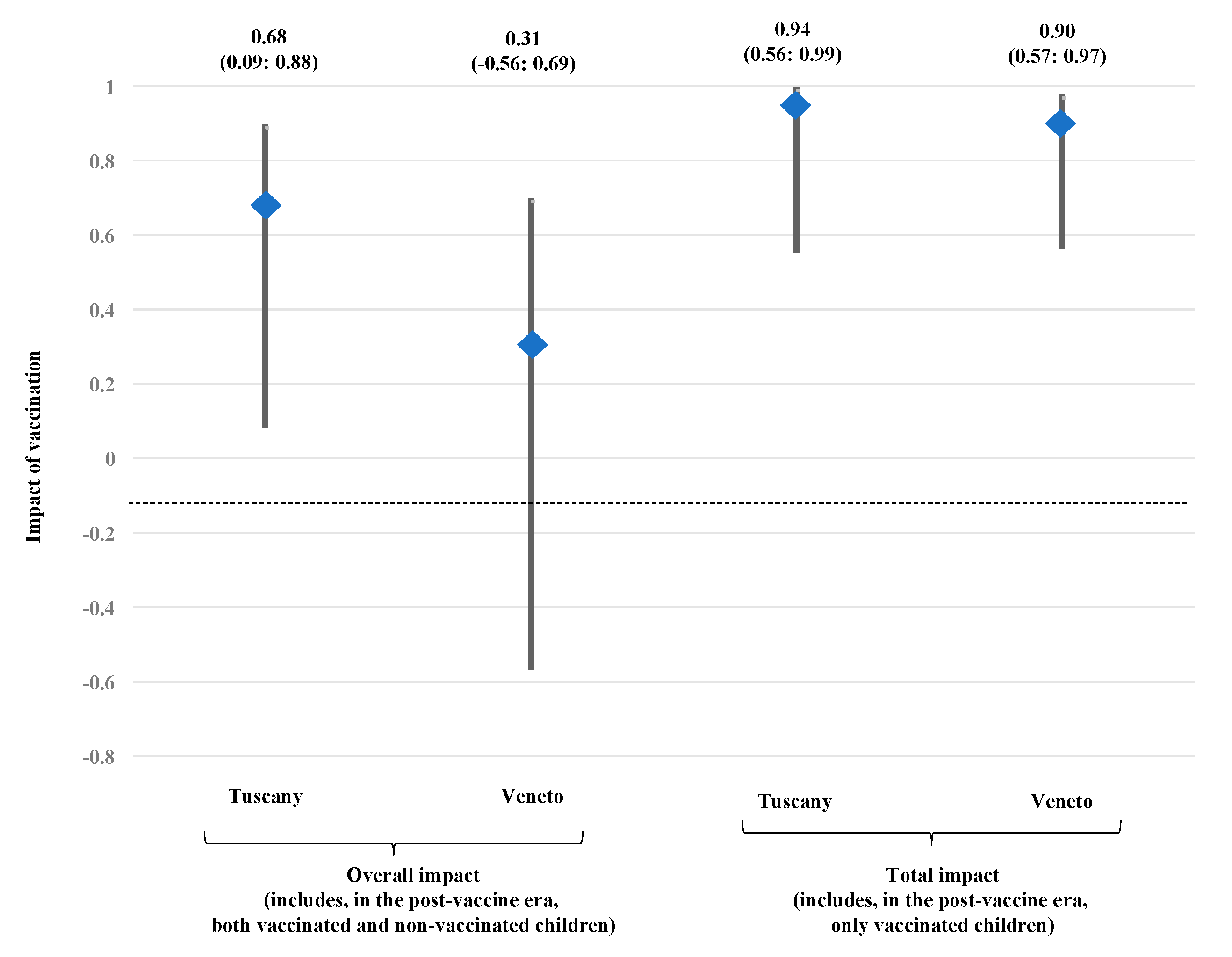
3.3. Impact of Vaccination in Tuscany and Veneto
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Boeddha, N.P.; Schlapbach, L.J.; Driessen, G.J.; Herberg, J.A.; Rivero-Calle, I.; Cebey-Lopez, M.; Klobassa, D.S.; Philipsen, R.; de Groot, R.; Inwald, D.P.; et al. Mortality and morbidity in community-acquired sepsis in European pediatric intensive care units: A prospective cohort study from the European Childhood Life-threatening Infectious Disease Study (EUCLIDS). Crit. Care 2018, 22, 143. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villena, R.; Safadi, M.A.P.; Valenzuela, M.T.; Torres, J.P.; Finn, A.; O’Ryan, M. Global epidemiology of serogroup B meningococcal disease and opportunities for prevention with novel recombinant protein vaccines. Hum. Vaccin. Immunother. 2018, 14, 1042–1057. [Google Scholar] [CrossRef] [PubMed]
- Istituto Superiore di Sanità. Sorveglianza delle Malattie Batteriche in Italia. Available online: old.iss.it/binary/mabi/cont/interim_Report_2018_finale.pdf (accessed on 16 July 2020).
- Azzari, C.; Canessa, C.; Lippi, F.; Moriondo, M.; Indolfi, G.; Nieddu, F.; Martini, M.; de Martino, M.; Castiglia, P.; Baldo, V.; et al. Distribution of invasive meningococcal B disease in Italian pediatric population: Implications for vaccination timing. Vaccine 2014, 32, 1187–1191. [Google Scholar] [CrossRef] [PubMed]
- Ladhani, S.N.; Flood, J.S.; Ramsay, M.E.; Campbell, H.; Gray, S.J.; Kaczmarski, E.B.; Mallard, R.H.; Guiver, M.; Newbold, L.S.; Borrow, R. Invasive meningococcal disease in England and Wales: Implications for the introduction of new vaccines. Vaccine 2012, 30, 3710–3716. [Google Scholar] [CrossRef] [PubMed]
- Piano Nazionale Prevenzione Vaccinale (PNPV) 2017–2019. Available online: salute.gov.it/mgs/C_17_pubblicazioni_2571_allegato.pdf (accessed on 14 July 2020).
- Baldovin, T.; Lazzari, R.; Cocchio, S.; Furlan, P.; Bertoncello, C.; Saia, M.; Russo, F.; Baldo, V. Invasive meningococcal disease in the Veneto region of Italy: A capture-recapture analysis for assessing the effectiveness of an integrated surveillance system. BMJ Open 2017, 7, e012478. [Google Scholar] [CrossRef] [PubMed]
- Azzari, C.; Nieddu, F.; Moriondo, M.; Indolfi, G.; Canessa, C.; Ricci, S.; Bianchi, L.; Serranti, D.; Poggi, G.M.; Resti, M.; et al. Underestimation of invasive meningococcal disease in Italy. Emerg. Infect. Dis. 2016, 22, 469–475. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harrison, O.B.; Claus, H.; Jiang, Y.; Bennett, J.S.; Bratcher, H.B.; Jolley, K.A.; Corton, C.; Care, R.; Poolman, J.T.; Zollinger, W.D.; et al. Description and nomenclature of Neisseria meningitidis capsule locus. Emerg. Infect. Dis. 2013, 19, 566–573. [Google Scholar] [CrossRef] [PubMed]
- Guiducci, S.; Moriondo, M.; Nieddu, F.; Ricci, S.; De Vitis, E.; Casini, A.; Poggi, G.M.; Indolfi, G.; Resti, M.; Azzari, C. Culture and Real-time Polymerase Chain reaction sensitivity in the diagnosis of invasive meningococcal disease: Does culture miss less severe cases? PLoS ONE 2019, 14, e0212922. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Farrington, C.P. Estimation of vaccine effectiveness using the screening method. Int. J. Epidemiol. 1993, 22, 742–746. [Google Scholar] [CrossRef] [PubMed]
- Parikh, S.R.; Andrews, N.J.; Beebeejaun, K.; Campbell, H.; Ribeiro, S.; Ward, C.; White, J.M.; Borrow, R.; Ramsay, M.E.; Ladhani, S.N. Effectiveness and impact of a reduced infant schedule of 4CMenB vaccine against group B meningococcal disease in England: A national observational cohort study. Lancet 2016, 388, 2775–2782. [Google Scholar] [CrossRef] [Green Version]
- Ladhani, S.N.; Andrews, N.; Parikh, S.R.; Campbell, H.; White, J.; Edelstein, M.; Bai, X.; Lucidarme, J.; Borrow, R.; Ramsay, M.E.; et al. Vaccination of infants with Meningococcal Group B Vaccine (4CMenB) in England. N. Engl. J. Med. 2020, 382, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Medini, D.; Stella, M.; Wassil, J. MATS: Global coverage estimates for 4CMenB, a novel multicomponent meningococcal B vaccine. Vaccine 2015, 33, 2629–2636. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Institut National de santé Public du Quebec. Impact épidémiologique de la Campagne de Vaccination contre le méningocoque de sérogroupe B dans la région du Saguenay-Lac-Saint-Jean, en 2014: Rapport au 30 juin 2018. Available online: https://www.inspq.qc.ca/publications/2491 (accessed on 16 July 2020).
- Deceuninck, G.; Lefebvre, B.; Tsang, R.; Betala-Belinga, J.F.; De Serres, G.; De Wals, P. Impact of a mass vaccination campaign against Serogroup B meningococcal disease in the Saguenay-Lac-Saint-Jean region of Quebec four years after its launch. Vaccine 2019, 37, 4243–4245. [Google Scholar] [CrossRef] [PubMed]
- Biolchi, A.; Tomei, S.; Santini, L.; Welsch, J.A.; Toneatto, D.; Gaitatzis, N.; Bai, X.; Borrow, R.; Giuliani, M.M.; Mori, E.; et al. Evaluation of strain coverage of the multicomponent meningococcal serogroup B vaccine (4CMenB) administered in infants according to different immunisation schedules. Hum. Vaccin. Immunother. 2019, 15, 725–731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azzari, C.; Moriondo, M.; Indolfi, G.; Cortimiglia, M.; Canessa, C.; Becciolini, L.; Lippi, F.; de Martino, M.; Resti, M. Realtime PCR is more sensitive than multiplex PCR for diagnosis and serotyping in children with culture negative pneumococcal invasive disease. PLoS ONE 2010, 5, e9282. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Cohort Group by Age of Birth | Coverage % at 24 Months Per Year | |
|---|---|---|
| TUSCANY | VENETO | |
| 2017 | 84.9 (2019) | 84.7 (2019) |
| 2016 | 86.1 (2018) | 82.0 (2018) |
| 2015 | 88.1 (2017) | 78.6 (2017) |
| 2014 | 76.8 (2016) | n.a. |
| Mean coverage | 83.9 | 81.7 |
| (A) TUSCANY | |||||||||||||
| 2006 | 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | |
| Age class | |||||||||||||
| 4–5 | 1 | 1 | 1 | ||||||||||
| 3–4 | 1 | 1 | 1 | 2 | 1 | 1 | |||||||
| 2–3 | 1 | 1 | 1 | ||||||||||
| 1–2 | 2 | 1 | 1 | 0 | 1 | 1 | |||||||
| 0–1 | 2 | 1 | 3 | 1 | 2 | 1 | 2 | 2 | 2 | ||||
| TOTAL | 3 | 1 | 3 | 5 | 5 | 2 | 4 | 4 | 2 | 2 | 0 | 1 | 3 |
| (B) VENETO | |||||||||||||
| 2007 | 2008 | 2009 | 2010 | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | ||
| Age class | |||||||||||||
| 3–4 | 1 | 1 | 1 | 1 | 1 | 1 | |||||||
| 2–3 | 1 | 1 | 2 | 1 | 1 | ||||||||
| 1–2 | 1 | 1 | 1 | 2 | 1 | 1 | 2 | ||||||
| 0–1 | 1 | 3 | 2 | 3 | 1 | 3 | 3 | 1 | 1 | 1 | 1 | ||
| TOTAL | 4 | 5 | 2 | 4 | 6 | 5 | 5 | 2 | 2 | 0 | 3 | 3 |
| PRE—4CMenB | POST—4CMenB | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age Groups | Number of Cases | Incidence * (Cases/100.000) | Number of Cases | Vaccinated Cases | Crude Incidence * (Cases/100.000) | ASR | Crude Incidence on Vaccinated Cases | ASR on Vaccinated Cases | IRR | IRR on Vaccinated Cases | Overall Impact (%) | Total Impact (%) |
| (A) TUSCANY | ||||||||||||
| 0–1 | 14 | 5.537 (5.44–5.62) | 2 | 1 | 1.452 (1.39–1.51) | 0.232 | 0.726 | 0.116 | 0.260 | 0.131 | 74% | 87% |
| 1–2 | 5 | 1.749 (1.70–1.80) | 1 | 0.887 (0.68–1.02) | 0.160 | 0.507 | 49% | |||||
| 2–3 | 2 | 0.631 (0.60–0.66) | 1 | 1.160 (1.00–1.50) | 0.232 | 1.838 | ||||||
| 3–4 | 7 | 2.007 (1.96–2.05) | 0 | |||||||||
| 4–5 | 3 | 0.789 (0.76–0.82) | 0 | |||||||||
| TOTAL | 31 | 1.956 | 4 | 1 | 0.941 | 0.624 | 0.726 | 0.116 | 0.320 | 0.060 | 68% | 94% |
| (B) VENETO | ||||||||||||
| 0–1 | 17 | 4.647 (4.33–4.97) | 3 | 1.956 (1.52–2.40) | 0.409 | 0.421 | 58% | |||||
| 1–2 | 6 | 1.447 (1.41–1.48) | 3 | 2 | 2.552 (2.46–2.64) | 0.605 | 0.851 | 0.200 | 1.764 | 0.590 | 41% | |
| 2–3 | 5 | 1.082 (1.05–1.11) | 1 | 1.253 (1.18–1.33) | 0.330 | 1.158 | ||||||
| 3–4 | 6 | 1.181 (1.15–1.21) | 0 | |||||||||
| TOTAL | 34 | 1.942 | 7 | 2 | 1.789 | 1.344 | 0.851 | 0.200 | 0.692 | 0.103 | 31% | 90% |
| Age Groups | Observed Cases | Vaccinated Cases | Expected Cases | SIR | SIR on Vaccinated Population | RCR | RCR on Vaccinated Population |
|---|---|---|---|---|---|---|---|
| (A) TUSCANY | |||||||
| 0–1 | 2 | 1 | 7.628 | 0.262 | 0.131 | 0.738 | 0.869 |
| 1–2 | 1 | - | 1.972 | 0.507 | - | 0.493 | - |
| 2–3 | 1 | - | 0.544 | 1.838 | - | 0.838 | - |
| 3–4 | 0 | - | 1.180 | 0 | - | 1 | - |
| 4–5 | 0 | - | 0.234 | 0 | - | 1 | - |
| TOTAL | 4 | 1 | 11.558 | 0.346 | 0.087 | 0.654 | 0.913 |
| (B) VENETO | |||||||
| 0–1 | 3 | - | 7.128 | 0.421 | - | 0.579 | - |
| 1–2 | 3 | 2 | 1.701 | 1.764 | 1.176 | −0.764 | −0.176 |
| 2–3 | 1 | - | 0.864 | 1.158 | - | −0.158 | |
| 3–4 | 0 | - | 0.480 | 0 | - | 1 | |
| TOTAL | 7 | 2 | 10.173 | 0.688 | 0.197 | 0.312 | 0.803 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Azzari, C.; Moriondo, M.; Nieddu, F.; Guarnieri, V.; Lodi, L.; Canessa, C.; Indolfi, G.; Giovannini, M.; Napoletano, G.; Russo, F.; et al. Effectiveness and Impact of the 4CMenB Vaccine against Group B Meningococcal Disease in Two Italian Regions Using Different Vaccination Schedules: A Five-Year Retrospective Observational Study (2014–2018). Vaccines 2020, 8, 469. https://doi.org/10.3390/vaccines8030469
Azzari C, Moriondo M, Nieddu F, Guarnieri V, Lodi L, Canessa C, Indolfi G, Giovannini M, Napoletano G, Russo F, et al. Effectiveness and Impact of the 4CMenB Vaccine against Group B Meningococcal Disease in Two Italian Regions Using Different Vaccination Schedules: A Five-Year Retrospective Observational Study (2014–2018). Vaccines. 2020; 8(3):469. https://doi.org/10.3390/vaccines8030469
Chicago/Turabian StyleAzzari, Chiara, Maria Moriondo, Francesco Nieddu, Valentina Guarnieri, Lorenzo Lodi, Clementina Canessa, Giuseppe Indolfi, Mattia Giovannini, Giuseppina Napoletano, Francesca Russo, and et al. 2020. "Effectiveness and Impact of the 4CMenB Vaccine against Group B Meningococcal Disease in Two Italian Regions Using Different Vaccination Schedules: A Five-Year Retrospective Observational Study (2014–2018)" Vaccines 8, no. 3: 469. https://doi.org/10.3390/vaccines8030469