
Side Effects and Perceptions Following COVID-19 Vaccination in Jordan: A Randomized, Cross-Sectional Study Implementing Machine Learning for Predicting Severity of Side Effects

 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. The Online Survey Tool
2.3. Sample Size
2.4. Statistical Analysis
2.5. Machine Learning
2.5.1. Random Forest (RF)
2.5.2. eXtreme Gradient Boosting (XGBoost)
2.5.3. Multilayer Perceptron (MLP)
2.5.4. K-Star (K*)
2.5.5. ML Model Evaluation
3. Results
3.1. Demographic Data
3.2. Pre-Vaccination
3.3. Post-Vaccination
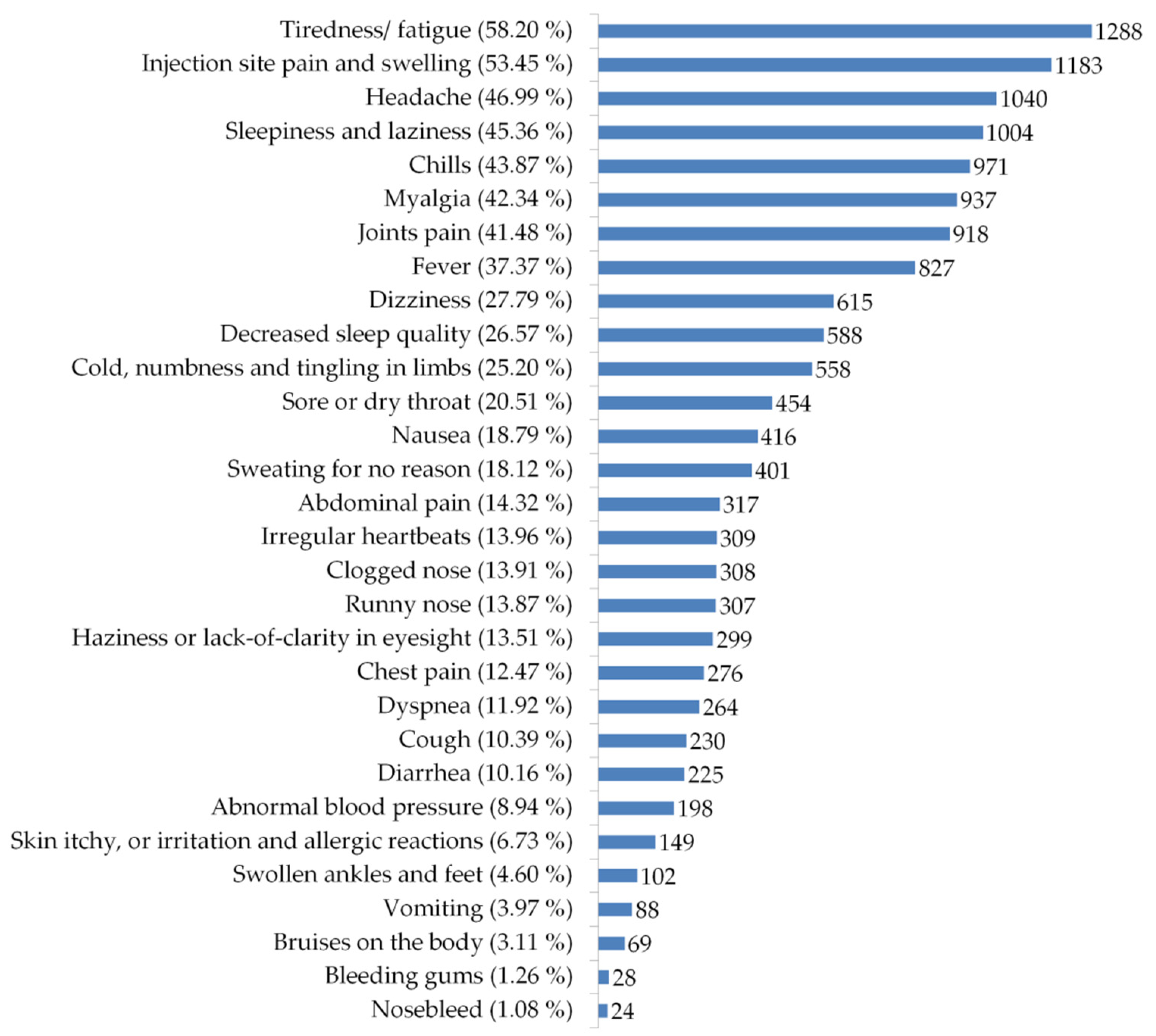
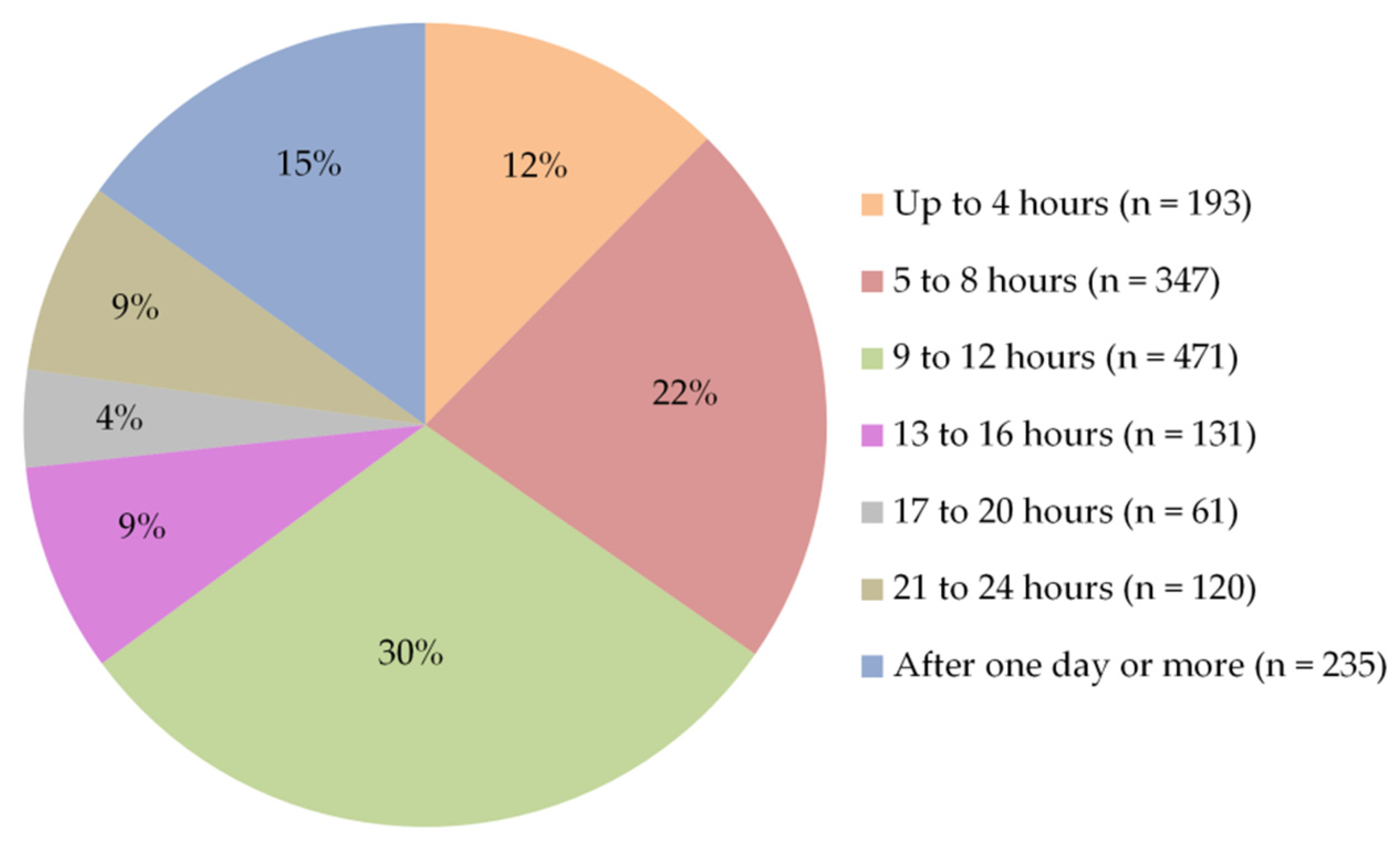
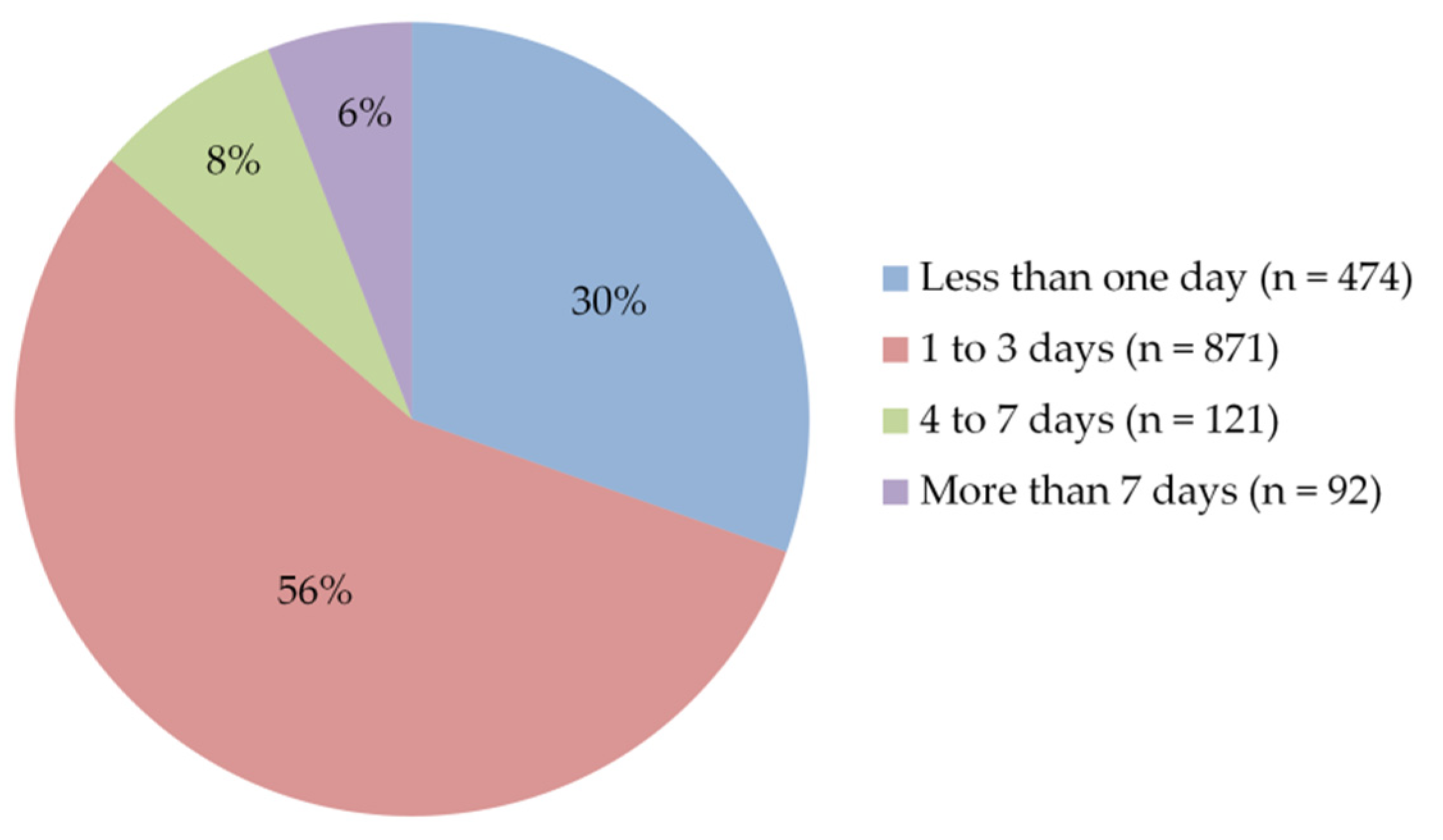
3.3.1. Post-Vaccination Side Effects
3.3.2. Side Effects and Number of Doses
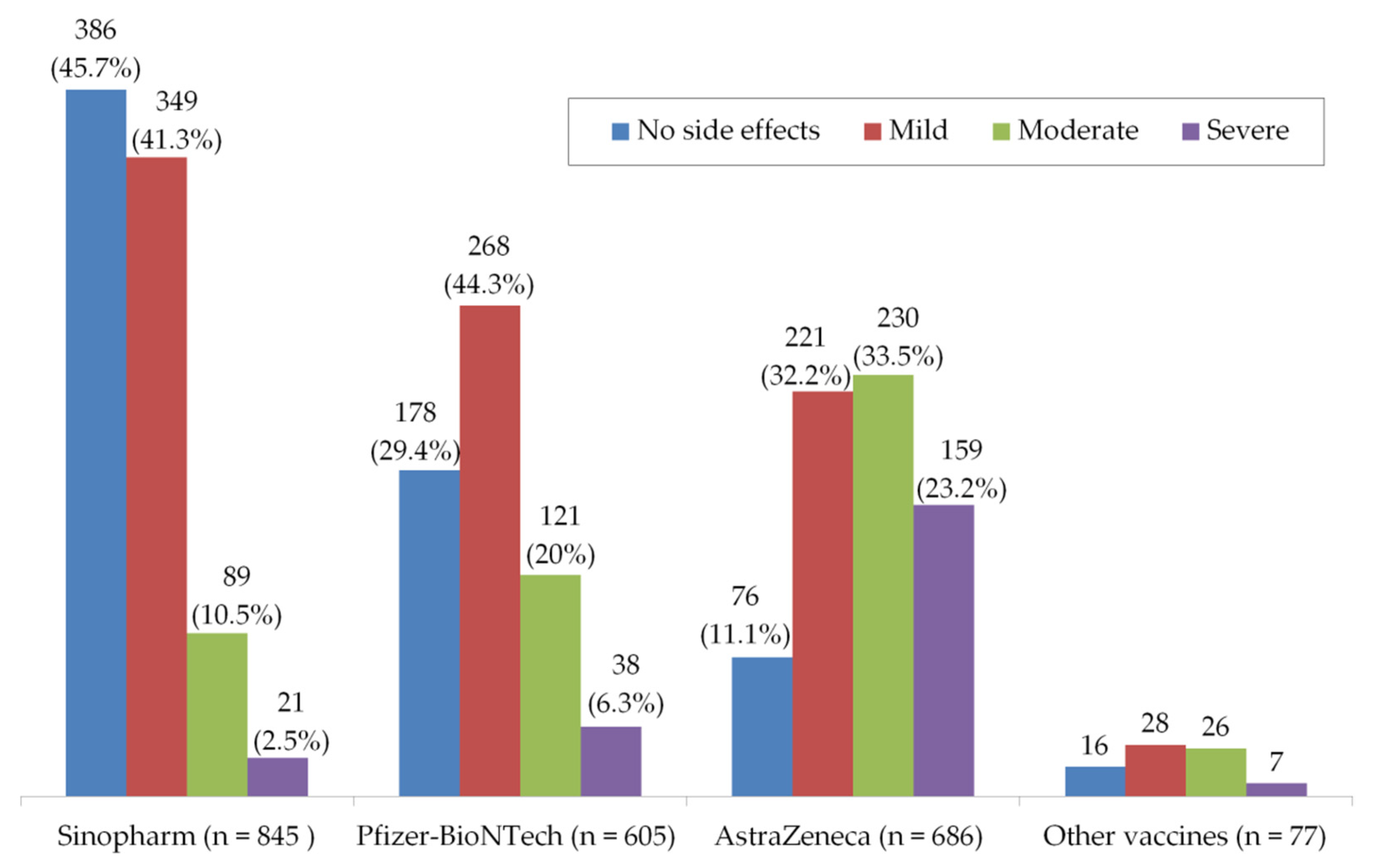
3.3.3. Side Effects and Types of Vaccines
3.4. ML to Predict the Severity of Side Effects
4. Discussion
5. Study Implications
6. Study Strengths and Limitations
7. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hatmal, M.M.; Alshaer, W.; Al-Hatamleh, M.A.I.; Hatmal, M.; Smadi, O.; Taha, M.O.; Oweida, A.J.; Boer, J.C.; Mohamud, R.; Plebanski, M. Comprehensive Structural and Molecular Comparison of Spike Proteins of SARS-CoV-2, SARS-CoV and MERS-CoV, and Their Interactions with ACE2. Cells 2020, 9, 2638. [Google Scholar] [CrossRef]
- Al-Hatamleh, M.A.I.; Hatmal, M.M.; Alshaer, W.; Rahman, E.N.S.E.A.; Mohd-Zahid, M.H.; Alhaj-Qasem, D.M.; Yean, C.Y.; Alias, I.Z.; Jaafar, J.; Ferji, K.; et al. COVID-19 infection and nanomedicine applications for development of vaccines and therapeutics: An overview and future perspectives based on polymersomes. Eur. J. Pharmacol. 2021, 896, 173930. [Google Scholar] [CrossRef]
- Al-Hatamleh, M.A.I.; Hatmal, M.M.; Sattar, K.; Ahmad, S.; Mustafa, M.Z.; Bittencourt, M.D.C.; Mohamud, R. Antiviral and Immunomodulatory Effects of Phytochemicals from Honey against COVID-19: Potential Mechanisms of Action and Future Directions. Molecules 2020, 25, 5017. [Google Scholar] [CrossRef]
- Swetha, G.; Rani, S.L.; Brundha, M. Awareness of the side effects of vaccination among general public. Drug Invention Today 2020, 14, 3. [Google Scholar]
- Haidere, M.F.; Ratan, Z.A.; Nowroz, S.; Zaman, S.B.; Jung, Y.J.; Hosseinzadeh, H.; Cho, J.Y. COVID-19 Vaccine: Critical Questions with Complicated Answers. Biomol. Ther. 2021, 29, 1–10. [Google Scholar] [CrossRef]
- Chung, Y.H.; Beiss, V.; Fiering, S.N.; Steinmetz, N.F. COVID-19 Vaccine Frontrunners and Their Nanotechnology Design. ACS Nano 2020, 14, 12522–12537. [Google Scholar] [CrossRef]
- Petousis-Harris, H. Assessing the Safety of COVID-19 Vaccines: A Primer. Drug Saf. 2020, 43, 1205–1210. [Google Scholar] [CrossRef]
- Milken Institute’s COVID-19 Treatment and Vaccine Tracker. Available online: https://covid-19tracker.milkeninstitute.org/#vaccines_intro (accessed on 19 April 2021).
- COVID-19 Statistical Report. Available online: https://corona.moh.gov.jo/ar (accessed on 17 April 2021).
- Jordan Reports Highest Daily Tally of COVID-19 Cases. Available online: https://www.reuters.com/article/health-coronavirus-jordan-idUSL1N2LD1JZ (accessed on 17 April 2021).
- The Lightning-Fast Quest for COVID Vaccines—And What It Means for Other Diseases. Available online: https://www.nature.com/articles/d41586-020-03626-1 (accessed on 25 April 2021).
- Episode #24—Vaccine Myths vs. Science. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/media-resources/science-in-5/episode-24---vaccine-myths-vs-science (accessed on 24 April 2021).
- Abu-Farha, R.K.; Alzoubi, K.H.; Khabour, O.F. Public Willingness to Participate in COVID-19 Vaccine Clinical Trials: A Study from Jordan. Patient Prefer Adherence 2020, 14, 2451–2458. [Google Scholar] [CrossRef] [PubMed]
- Sallam, M.; Dababseh, D.; Eid, H.; Al-Mahzoum, K.; Al-Haidar, A.; Taim, D.; Yaseen, A.; Ababneh, N.A.; Bakri, F.G.; Mahafzah, A. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines 2021, 9, 42. [Google Scholar] [CrossRef] [PubMed]
- Nunez-Lopez, Y.O.; Retnakaran, R.; Zinman, B.; Pratley, R.E.; Seyhan, A.A. Predicting and understanding the response to short-term intensive insulin therapy in people with early type 2 diabetes. Mol. Metab. 2019, 20, 63–78. [Google Scholar] [CrossRef] [PubMed]
- Kappel, B.A.; De Angelis, L.; Heiser, M.; Ballanti, M.; Stoehr, R.; Goettsch, C.; Mavilio, M.; Artati, A.; Paoluzi, O.A.; Adamski, J.; et al. Cross-omics analysis revealed gut microbiome-related metabolic pathways underlying atherosclerosis development after antibiotics treatment. Mol. Metab. 2020, 36, 100976. [Google Scholar] [CrossRef]
- Tao, C.; Pan, H.; Li, Y.; Zou, Z. Unsupervised Spectral–Spatial Feature Learning With Stacked Sparse Autoencoder for Hyperspectral Imagery Classification. IEEE Geosci. Remote Sens. Lett. 2015, 12, 2438–2442. [Google Scholar] [CrossRef]
- Rozinajová, V.; Ezzeddine, A.B.; Lóderer, M.; Loebl, J.; Magyar, R.; Vrablecová, P. Computational Intelligence in Smart Grid Environment. In Computational Intelligence for Multimedia Big Data on the Cloud with Engineering Applications; Sangaiah, A.K., Sheng, M., Zhang, Z., Eds.; Academic Press: Cambridge, MA, USA, 2018; pp. 23–59. [Google Scholar]
- Ren, X.; Guo, H.; Li, S.; Wang, S.; Li, J. A Novel Image Classification Method with CNN-XGBoost Model. In Digital Forensics and Watermarking; Kraetzer, C., Shi, Y.Q., Dittmann, J., Kim, H., Eds.; Springer: Cham, Switzerland, 2017; Volume 10431, pp. 378–390. [Google Scholar]
- Babajide Mustapha, I.; Saeed, F. Bioactive Molecule Prediction Using Extreme Gradient Boosting. Molecules 2016, 21, 983. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Riedmiller, M.; Braun, H. A direct adaptive method for faster backpropagation learning: The RPROP algorithm. In Proceedings of the IEEE International Conference on Neural Networks, San Francisco, CA, USA, 28 March–1 April 1993; Volume 581, pp. 586–591. [Google Scholar]
- Wiharto, W.; Kusnanto, H.; Herianto, H. Intelligence System for Diagnosis Level of Coronary Heart Disease with K-Star Algorithm. Health Inform. Res. 2016, 22, 30–38. [Google Scholar] [CrossRef] [Green Version]
- Hatmal, M.M.; Abderrahman, S.M.; Nimer, W.; Al-Eisawi, Z.; Al-Ameer, H.J.; Al-Hatamleh, M.A.I.; Mohamud, R.; Alshaer, W. Artificial Neural Networks Model for Predicting Type 2 Diabetes Mellitus Based on VDR Gene FokI Polymorphism, Lipid Profile and Demographic Data. Biology 2020, 9, 222. [Google Scholar] [CrossRef]
- McHugh, M.L. Interrater reliability: The kappa statistic. Biochem. Med. 2012, 22, 276–282. [Google Scholar] [CrossRef]
- Shekhar, R.; Sheikh, A.B.; Upadhyay, S.; Singh, M.; Kottewar, S.; Mir, H.; Barrett, E.; Pal, S. COVID-19 Vaccine Acceptance among Health Care Workers in the United States. Vaccines 2021, 9, 119. [Google Scholar] [CrossRef]
- Chew, N.; Cheong, C.; Kong, G.; Phua, K.; Ngiam, J.N.; Tan, B.; Wang, B.; Hao, F.; Tan, W.; Han, X.; et al. An Asia-Pacific study on healthcare workers’ perceptions of, and willingness to receive, the COVID-19 vaccination. Int. J. Infect. Dis. 2021, 106, 52–60. [Google Scholar] [CrossRef] [PubMed]
- Riad, A.; Pokorná, A.; Attia, S.; Klugarová, J.; Koščík, M.; Klugar, M. Prevalence of COVID-19 Vaccine Side Effects among Healthcare Workers in the Czech Republic. J. Clin. Med. 2021, 10, 1428. [Google Scholar] [CrossRef] [PubMed]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Gajula, V.; Madathala, R.R.; Chennaiahgari, N.; Malayala, S.V. Adverse effects of COVID-19 mRNA-1273 vaccine: A randomized, cross-sectional study on healthcare workers with detailed self-reported symptoms. J. Med. Virol. 2021. [Google Scholar] [CrossRef]
- Kadali, R.A.K.; Janagama, R.; Peruru, S.; Malayala, S.V. Side effects of BNT162b2 mRNA COVID-19 vaccine: A randomized, cross-sectional study with detailed self-reported symptoms from healthcare workers. Int. J. Infect. Dis. 2021, 106, 376–381. [Google Scholar] [CrossRef]
- Jayadevan, R.; Shenoy, R.; Anithadevi, T. Survey of symptoms following COVID-19 vaccination in India. medRxiv 2021. [Google Scholar] [CrossRef]
- El-Shitany, N.A.; Harakeh, S.; Badr-Eldin, S.M.; Bagher, A.M.; Eid, B.; Almukadi, H.; Alghamdi, B.S.; Alahmadi, A.A.; Hassan, N.A.; Sindi, N. Minor to Moderate Side Effects of Pfizer-BioNTech COVID-19 Vaccine Among Saudi Residents: A Retrospective Cross-Sectional Study. Int. J. Gen. Med. 2021, 14, 1389–1401. [Google Scholar] [CrossRef] [PubMed]
- Chapin-Bardales, J.; Gee, J.; Myers, T. Reactogenicity Following Receipt of mRNA-Based COVID-19 Vaccines. JAMA 2021. [Google Scholar] [CrossRef] [PubMed]
- Menni, C.; Klaser, K.; May, A.; Polidori, L.; Capdevila, J.; Louca, P.; Sudre, C.H.; Nguyen, L.H.; Drew, D.A.; Merino, J.; et al. Vaccine side-effects and SARS-CoV-2 infection after vaccination in users of the COVID Symptom Study app in the UK: A prospective observational study. Lancet Infect. Dis. 2021. [Google Scholar] [CrossRef]
- Possible Side Effects After Getting a COVID-19 Vaccine. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/expect/after.html (accessed on 25 April 2021).
- Kashte, S.; Gulbake, A.; El-Amin Iii, S.F.; Gupta, A. COVID-19 vaccines: Rapid development, implications, challenges and future prospects. Hum. Cell 2021, 34, 711–733. [Google Scholar] [CrossRef]
- Folegatti, P.M.; Ewer, K.J.; Aley, P.K.; Angus, B.; Becker, S.; Belij-Rammerstorfer, S.; Bellamy, D.; Bibi, S.; Bittaye, M.; Clutterbuck, E.A.; et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: A preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet 2020, 396, 467–478. [Google Scholar] [CrossRef]
- Walsh, E.E.; Frenck, R.W.; Falsey, A.R.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Neuzil, K.; Mulligan, M.J.; Bailey, R.; et al. Safety and Immunogenicity of Two RNA-Based Covid-19 Vaccine Candidates. N. Engl. J. Med. 2020, 383, 2439–2450. [Google Scholar] [CrossRef]
- Silveira, M.M.; Moreira, G.; Mendonca, M. DNA vaccines against COVID-19: Perspectives and challenges. Life Sci. 2021, 267, 118919. [Google Scholar] [CrossRef]
- Xia, S.; Zhang, Y.; Wang, Y.; Wang, H.; Yang, Y.; Gao, G.F.; Tan, W.; Wu, G.; Xu, M.; Lou, Z. Safety and immunogenicity of an inactivated SARS-CoV-2 vaccine, BBIBP-CorV: A randomised, double-blind, placebo-controlled, phase 1/2 trial. Lancet Infect. Dis. 2021, 21, 39–51. [Google Scholar] [CrossRef]
- Van Doremalen, N.; Lambe, T.; Spencer, A.; Belij-Rammerstorfer, S.; Purushotham, J.N.; Port, J.R.; Avanzato, V.A.; Bushmaker, T.; Flaxman, A.; Ulaszewska, M.; et al. ChAdOx1 nCoV-19 vaccine prevents SARS-CoV-2 pneumonia in rhesus macaques. Nature 2020, 586, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhang, Y.; Huang, B.; Deng, W.; Quan, Y.; Wang, W.; Xu, W.; Zhao, Y.; Li, N.; Zhang, J.; et al. Development of an Inactivated Vaccine Candidate, BBIBP-CorV, with Potent Protection against SARS-CoV-2. Cell 2020, 182, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Wise, J. Covid-19: European countries suspend use of Oxford-AstraZeneca vaccine after reports of blood clots. BMJ 2021, 372, n699. [Google Scholar] [CrossRef]
- AstraZeneca’s COVID-19 Vaccine: EMA Finds Possible Link to Very Rare Cases of Unusual Blood Clots with Low Blood Platelets. Available online: https://www.ema.europa.eu/en/news/astrazenecas-covid-19-vaccine-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood (accessed on 28 April 2021).
- Carli, G.; Nichele, I.; Ruggeri, M.; Barra, S.; Tosetto, A. Deep vein thrombosis (DVT) occurring shortly after the second dose of mRNA SARS-CoV-2 vaccine. Intern. Emerg. Med. 2021, 16, 803–804. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, S.; Banerjee, M. Immune Thrombocytopenia Secondary to COVID-19: A Systematic Review. SN Compr. Clin. Med. 2020, 2, 2048–2058. [Google Scholar] [CrossRef] [PubMed]
- Wool, G.D.; Miller, J.L. The Impact of COVID-19 Disease on Platelets and Coagulation. Pathobiology 2021, 88, 15–27. [Google Scholar] [CrossRef]
- Wold, W.S.; Toth, K. Adenovirus vectors for gene therapy, vaccination and cancer gene therapy. Curr. Gene. Ther. 2013, 13, 421–433. [Google Scholar] [CrossRef]
- Othman, M.; Labelle, A.; Mazzetti, I.; Elbatarny, H.S.; Lillicrap, D. Adenovirus-induced thrombocytopenia: The role of von Willebrand factor and P-selectin in mediating accelerated platelet clearance. Blood 2007, 109, 2832–2839. [Google Scholar] [CrossRef]
- WHO Issues Its First Emergency Use Validation for a COVID-19 Vaccine and Emphasizes Need for Equitable Global Access. Available online: https://www.who.int/news/item/31-12-2020-who-issues-its-first-emergency-use-validation-for-a-covid-19-vaccine-and-emphasizes-need-for-equitable-global-access (accessed on 25 April 2021).
- Amit, S.; Regev-Yochay, G.; Afek, A.; Kreiss, Y.; Leshem, E. Early rate reductions of SARS-CoV-2 infection and COVID-19 in BNT162b2 vaccine recipients. Lancet 2021, 397, 875–877. [Google Scholar] [CrossRef]
- Tripathi, R.; Alqahtani, S.S.; Albarraq, A.A.; Meraya, A.M.; Tripathi, P.; Banji, D.; Alshahrani, S.; Ahsan, W.; Alnakhli, F.M. Awareness and Preparedness of COVID-19 Outbreak Among Healthcare Workers and Other Residents of South-West Saudi Arabia: A Cross-Sectional Survey. Front. Public Health 2020. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleiss, J.L.; Levin, B.; Paik, M.C. Statistical Methods for Rates and Proportions, 3rd ed.; John Wiley & Sons, Inc.: New York, NY, USA, 2003. [Google Scholar]
- Mahmood, D.Y.; Hussein, M.A. Intrusion detection system based on K-star classifier and feature set reduction. IOSR J. Comput. Eng. 2013, 15, 107–112. [Google Scholar]
- Purdey, S.; Huntley, A. Predicting and preventing avoidable hospital admissions: A review. J. R. Coll. Physicians Edinb. 2013, 43, 340–344. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Wu, L.; Yu, X.; Zhao, F.; Russell, A.; Song, M.; Wang, W. The expected number of background disease events during mass immunization in China. PLoS ONE 2013, 8, e71818. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Wu, L.; Yu, X.; Zhao, F.; Russell, A.; Song, M.; Wang, W. Awareness of the background rate of sudden cardiac death during mass immunization with pandemic H1N1 influenza vaccines increases the intended vaccination rate. Prev. Med. 2010, 51, 445–446. [Google Scholar] [CrossRef]











{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable (n, %) | Participants (n = 2213) | |
|---|---|---|
| Male n = 869 (39.2 %) | Female n = 1344 (60.8 %) | |
| Healthcare workers (726, 32.7) | 269 (30.91) | 457 (69.09) |
| Age categories (year): | ||
| Less than 20 (8, 0.36) | 3 (0.34) | 5 (0.37) |
| 29–20 (564, 25.42) | 185 (21.26) | 379 (28.11) |
| 39–30 (577, 26.01) | 254 (29.19) | 323 (23.96) |
| 49–40 (490, 22.09) | 169 (19.42) | 321 (23.81) |
| 59–50 (365, 16.45) | 152 (17.47) | 213 (15.80) |
| 60 or more (214, 9.64) | 107 (12.29) | 107 (7.93) |
| Educational levels: | ||
| High school or less (319, 14.38) | 125 (14.36) | 194 (14.39) |
| Diploma/Bachelor’s degree (1453, 65.50) | 562 (64.59) | 891 (66.09) |
| Postgraduate studies (446, 20.10) | 183 (21.03) | 263 (19.51) |
| Places of residence: | ||
| City (1923, 86.69) | 717 (82.41) | 1206 (89.46) |
| Village (266, 11.99) | 136 (15.63) | 130 (9.64) |
| Badia (7, 0.31) | 4 (0.45) | 3 (0.22) |
| Refugee camp (22, 0.99) | 13 (1.49) | 9 (0.66) |
| Sources of Information about COVID-19 Vaccines | n | % |
|---|---|---|
| Source (1): Medical and scientific websites | 632 | 28 |
| Source (2): Public media | 290 | 13 |
| Source (3): Social media platforms | 248 | 11 |
| Source (4): Colleagues, friends and relatives | 96 | 4 |
| Sources 1, 2, 3, and 4 | 163 | 7 |
| Sources 1, 2, and 3 | 166 | 7 |
| Sources 2, 3, and 4 | 75 | 3 |
| Sources 1, 2, and 4 | 24 | 1 |
| Sources 1, 3, and 4 | 30 | 1 |
| Sources 2 and 3 | 94 | 4 |
| Sources 1 and 2 | 155 | 7 |
| Sources 1 and 4 | 30 | 1 |
| Sources 3 and 4 | 48 | 2 |
| Sources 2 and 4 | 31 | 1 |
| Sources 1 and 3 | 96 | 4 |
| No information | 42 | 2 |
| Vaccine | Participants n (%) | First Dose n (%) | Second Dose n (%) |
|---|---|---|---|
| Sinopharm | 845 (38.2) | 700 (82.84) | 145 (17.16) |
| AstraZeneca | 686 (31%) | 669 (97.52) | 17 (2.48) |
| Pfizer-BioNTech | 605 (27.34) | 342 (56.53) | 263 (43.47) |
| Sputnik V | 65 (2.93) | 63 (96.92) | 2 (3.08) |
| Moderna | 7 (0.31) | 5 (71.4) | 2 (28.6) |
| Covaxin | 3 (0.13) | 1 (33.3) | 2 (66.7) |
| Johnson & Johnson | 2 (0.09) | 2 (100) | 0 (0.00) |
| Total | 2213 (100) | 1782 (80.6) | 431 (19.4) |
| One Dose (n = 1782) n (%) | Two Doses (n = 431) n (%) | p-Value | |
|---|---|---|---|
| Side effects | 0.01 * | ||
| Presence | 1279 (71.8) | 279 (64.7) | |
| Absence | 503 (28.2) | 152 (35.3) | |
| Number of side effects | 0.00 * | ||
| 0 | 504 (28.3) | 151 (35) | |
| 1–6 | 449 (25.2) | 122 (28.3) | |
| 7–12 | 491 (27.5) | 97 (22.5) | |
| >12 | 338 (19.0) | 61 (14.2) | |
| Infected with COVID-19 after vaccination | 79 (4.4) | 34 (7.9) | 0.00 * |
| Feeling more reassured after vaccination | 1397 (78.4) | 376 (87.2) | 0.00 * |
| One Dose (n = 1782) | Two Doses (n = 431) | χ2 | p-Value | ||
|---|---|---|---|---|---|
| The severity of side effects | Non | 504 | 151 | 2.92 | 0.09 |
| Mild | 705 | 162 | |||
| Moderate | 378 | 88 | |||
| Severe | 195 | 30 | |||
| Infected after vaccination | Yes | 78 | 35 | 8.02 | 0.00 ** |
| No | 1704 | 396 | |||
| Tiredness | Present | 1068 | 220 | 3.24 | 0.07 |
| Absent | 210 | 60 | |||
| Fever | Present | 688 | 139 | 1.32 | 0.25 |
| Absent | 590 | 141 | |||
| Headache | Present | 868 | 172 | 3.78 | 0.05 |
| Absent | 410 | 108 | |||
| Haziness or lack-of-clarity in eyesight | Present | 254 | 45 | 1.84 | 0.17 |
| Absent | 1024 | 235 | |||
| Injection site pain and swelling | Present | 965 | 218 | 0.73 | 0.39 |
| Absent | 313 | 62 | |||
| Joint pain | Present | 766 | 152 | 2.6 | 0.11 |
| Absent | 512 | 128 | |||
| Swollen ankles and feet | Present | 76 | 26 | 3.72 | 0.05 |
| Absent | 1202 | 254 | |||
| Myalgia | Present | 779 | 158 | 1.61 | 0.20 |
| Absent | 499 | 122 | |||
| Nausea | Present | 356 | 60 | 4.4 | 0.04 ** |
| Absent | 922 | 220 | |||
| Abdominal pain | Present | 272 | 45 | 3.44 | 0.06 |
| Absent | 1006 | 235 | |||
| Diarrhea | Present | 189 | 36 | 0.51 | 0.48 |
| Absent | 1089 | 244 | |||
| Vomiting | Present | 74 | 14 | 0.13 | 0.72 |
| Absent | 1204 | 266 | |||
| Bruises on the body | Present | 58 | 11 | 0.08 | 0.78 |
| Absent | 1220 | 269 | |||
| Bleeding gums | Present | 23 | 5 | 0.06 | 0.80 |
| Absent | 1255 | 275 | |||
| Nosebleed | Present | 21 | 3 | 0.18 | 0.67 * |
| Absent | 1257 | 277 | |||
| Chills | Present | 812 | 159 | 3.91 | 0.05 ** |
| Absent | 466 | 121 | |||
| Itchy skin, or irritation and allergic reactions | Present | 120 | 29 | 0.16 | 0.69 |
| Absent | 1158 | 251 | |||
| Sweating for no reason | Present | 339 | 62 | 2 | 0.16 |
| Absent | 939 | 218 | |||
| Cold, numbness, and tingling in limbs | Present | 486 | 72 | 14.35 | 0.00 ** |
| Absent | 792 | 208 | |||
| Dizziness | Present | 522 | 93 | 5.1 | 0.02 ** |
| Absent | 756 | 187 | |||
| Clogged nose | Present | 249 | 59 | 0.3 | 0.58 |
| Absent | 1029 | 221 | |||
| Runny nose | Present | 259 | 48 | 1.17 | 0.28 |
| Absent | 1019 | 232 | |||
| Dyspnea | Present | 218 | 46 | 0.02 | 0.89 |
| Absent | 1060 | 234 | |||
| Chest pain | Present | 232 | 44 | 0.74 | 0.39 |
| Absent | 1046 | 236 | |||
| Sleepiness and laziness | Present | 848 | 156 | 10.45 | 0.00 ** |
| Absent | 430 | 124 | |||
| Irregular heartbeats | Present | 255 | 54 | 0.02 | 0.89 |
| Absent | 1023 | 226 | |||
| Abnormal blood pressure | Present | 152 | 46 | 3.95 | 0.05 ** |
| Absent | 1126 | 234 | |||
| Sore or dry throat | Present | 380 | 74 | 0.99 | 0.32 |
| Absent | 898 | 206 | |||
| Cough | Present | 194 | 36 | 0.77 | 0.38 |
| Absent | 1084 | 244 |
| Vaccines | χ2 | p-Value | |||||
|---|---|---|---|---|---|---|---|
| Sino. | Pfizer. | Astra. | O. | ||||
| Severity of side effects | Non | 386 | 178 | 76 | 16 | 12.24 | 0.00 ** |
| Mild | 349 | 268 | 221 | 28 | |||
| Moderate | 89 | 121 | 230 | 26 | |||
| Severe | 21 | 38 | 159 | 7 | |||
| Infected after vaccination | Yes | 33 | 39 | 39 | 2 | 2.57 | 0.11 |
| No | 812 | 566 | 647 | 75 | |||
| Tiredness | Present | 354 | 319 | 563 | 52 | 0.36 | 0.55 |
| Absent | 105 | 108 | 47 | 9 | |||
| Fever | Present | 168 | 187 | 434 | 38 | 2.33 | 0.13 |
| Absent | 291 | 240 | 176 | 23 | |||
| Headache | Present | 276 | 260 | 460 | 44 | 0.01 | 0.92 |
| Absent | 183 | 167 | 150 | 17 | |||
| Haziness or lack-of-clarity in eyesight | Present | 84 | 57 | 147 | 11 | 1.68 | 0.19 |
| Absent | 375 | 370 | 463 | 50 | |||
| Injection site pain and swelling | Present | 281 | 373 | 484 | 45 | 45.68 | 0.00 ** |
| Absent | 178 | 54 | 126 | 16 | |||
| Joint pain | Present | 220 | 201 | 456 | 41 | 0.01 | 0.92 |
| Absent | 239 | 226 | 154 | 20 | |||
| Swollen ankles and feet | Present | 26 | 19 | 53 | 4 | 0.14 | 0.71 |
| Absent | 433 | 408 | 557 | 57 | |||
| Myalgia | Present | 221 | 219 | 455 | 42 | 0.40 | 0.53 |
| Absent | 238 | 208 | 155 | 19 | |||
| Nausea | Present | 107 | 96 | 193 | 20 | 0.01 | 0.92 |
| Absent | 352 | 331 | 417 | 41 | |||
| Abdominal pain | Present | 97 | 68 | 141 | 11 | 1.80 | 0.18 |
| Absent | 362 | 359 | 469 | 50 | |||
| Diarrhea | Present | 55 | 52 | 110 | 8 | 0.00 | 1.00 |
| Absent | 404 | 375 | 500 | 53 | |||
| Vomiting | Present | 17 | 16 | 52 | 3 | 0.03 | 0.86 |
| Absent | 442 | 411 | 558 | 58 | |||
| Bruises on the body | Present | 20 | 12 | 34 | 3 | 0.39 | 0.53 |
| Absent | 439 | 415 | 576 | 58 | |||
| Bleeding gums | Present | 11 | 1 | 15 | 1 | 2.22 | 0.14 * |
| Absent | 448 | 426 | 595 | 60 | |||
| Nosebleed | Present | 9 | 2 | 11 | 2 | 0.99 | 0.32 * |
| Absent | 450 | 425 | 599 | 59 | |||
| Chills | Present | 207 | 238 | 481 | 45 | 5.63 | 0.02 ** |
| Absent | 252 | 189 | 129 | 16 | |||
| Itchy skin, or irritation and allergic reactions | Present | 47 | 31 | 62 | 9 | 0.97 | 0.32 |
| Absent | 412 | 396 | 548 | 52 | |||
| Sweating for no reason | Present | 93 | 71 | 224 | 13 | 0.69 | 0.41 |
| Absent | 366 | 356 | 386 | 48 | |||
| Cold, numbness, and tingling in limbs | Present | 140 | 115 | 278 | 25 | 0.55 | 0.46 |
| Absent | 319 | 312 | 332 | 36 | |||
| Dizziness | Present | 168 | 131 | 288 | 28 | 1.61 | 0.20 |
| Absent | 291 | 296 | 322 | 33 | |||
| Clogged nose | Present | 115 | 70 | 108 | 15 | 5.42 | 0.02 ** |
| Absent | 344 | 357 | 502 | 46 | |||
| Runny nose | Present | 111 | 66 | 114 | 16 | 5.52 | 0.02 ** |
| Absent | 348 | 361 | 496 | 45 | |||
| Dyspnea | Present | 71 | 54 | 127 | 12 | 0.53 | 0.47 |
| Absent | 388 | 373 | 483 | 49 | |||
| Chest pain | Present | 60 | 63 | 139 | 14 | 0.14 | 0.71 |
| Absent | 399 | 364 | 471 | 47 | |||
| Sleepiness and laziness | Present | 308 | 230 | 420 | 46 | 9.06 | 0.00 ** |
| Absent | 151 | 197 | 190 | 15 | |||
| Irregular heartbeats | Present | 66 | 72 | 158 | 13 | 0.34 | 0.56 |
| Absent | 393 | 355 | 452 | 48 | |||
| Abnormal blood pressure | Present | 46 | 50 | 95 | 7 | 0.19 | 0.66 |
| Absent | 413 | 377 | 515 | 54 | |||
| Sore or dry throat | Present | 153 | 100 | 180 | 21 | 5.52 | 0.02 ** |
| Absent | 306 | 327 | 430 | 40 | |||
| Cough | Present | 61 | 57 | 100 | 12 | 0.01 | 0.92 |
| Absent | 398 | 370 | 510 | 49 | |||
| Number of side effects | 0 | 386 | 178 | 76 | 16 | 18.85 | 0.00 ** |
| 1–6 | 205 | 202 | 146 | 17 | |||
| 7–12 | 169 | 147 | 248 | 24 | |||
| >12 | 86 | 78 | 216 | 19 | |||
| Predicted Side Effects | Side Effects | |||
|---|---|---|---|---|
| (A) No Side Effects | (B) Mild | (C) Moderate | (D) Severe | |
| (A) No side effects | TPA | EBA | ECA | EDA |
| (B) Mild | EAB | TPB | ECB | EDB |
| (C) Moderate | EAC | EBC | TPC | EDC |
| (D) Severe | EAD | EBD | ECD | TPD |
| MLP | XGBoost | RF | K* | |
|---|---|---|---|---|
| Accuracy | 0.70 | 0.79 | 0.80 | 0.44 |
| Cohen’s κ | 0.56 | 0.70 | 0.71 | 0.19 |
| TPRA | 0.74 | 1.00 | 1.00 | 0.32 |
| TNRA | 0.92 | 1.00 | 1.00 | 0.72 |
| TPRB | 0.76 | 0.79 | 0.80 | 0.55 |
| TNRB | 0.49 | 0.44 | 0.44 | 0.60 |
| TPRC | 0.52 | 0.53 | 0.56 | 0.42 |
| TNRC | 0.73 | 0.70 | 0.70 | 0.81 |
| TPRD | 0.61 | 0.65 | 0.66 | 0.50 |
| TNRD | 0.86 | 0.86 | 0.86 | 0.88 |
| Study ID [Reference] | Country | Study Population | Sample Size | Vaccine Type (n) |
|---|---|---|---|---|
| El-Shitany et al., 2021 [31] | Saudi Arabia | General inhabitants | 455 | Pfizer-BioNTech |
| Riad et al., 2021 [27] | Czech Republic | Healthcare workers | 877 | Pfizer–BioNTech |
| Kadali et al., 2021a [28] | United States | Healthcare workers | 1116 | Moderna |
| Kadali et al., 2021b [29] | United States | Healthcare workers | 1245 | Pfizer–BioNTech |
| Jayadevan et al., 2021 [30] | India | Healthcare workers | 5396 | Covishield (5128), Covaxin (180), Pfizer–BioNTech (44), and Sinopharm (44) |
| Menni et al., 2021 [33] | United Kingdom | General inhabitants | 627,383 | Pfizer-BioNTech (282,103) and AstraZeneca (345,280) |
| Chapin-Bardales et al., 2021 [32] | United States | General inhabitants | 3,643,918 | Pfizer-BioNTech (1,659,724) and Moderna (1,984,194) |
| Participant | Gender | Age Category | Vaccine | Number of Doses | Diagnosed with Blood Clots |
|---|---|---|---|---|---|
| 1 | Male | 20–29 | Pfizer-BioNTech | 2 | Yes |
| 2 | Male | 50–59 | Pfizer-BioNTech | 1 | No |
| 3 | Male | 20–29 | AstraZeneca | 2 | Yes |
| 4 | Female | 50–59 | Sinopharm | 1 | No |
| 5 | Female | >60 | Sinopharm | 1 | No |
| 6 | Female | 30–39 | AstraZeneca | 2 | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hatmal, M.M.; Al-Hatamleh, M.A.I.; Olaimat, A.N.; Hatmal, M.; Alhaj-Qasem, D.M.; Olaimat, T.M.; Mohamud, R. Side Effects and Perceptions Following COVID-19 Vaccination in Jordan: A Randomized, Cross-Sectional Study Implementing Machine Learning for Predicting Severity of Side Effects. Vaccines 2021, 9, 556. https://doi.org/10.3390/vaccines9060556
Hatmal MM, Al-Hatamleh MAI, Olaimat AN, Hatmal M, Alhaj-Qasem DM, Olaimat TM, Mohamud R. Side Effects and Perceptions Following COVID-19 Vaccination in Jordan: A Randomized, Cross-Sectional Study Implementing Machine Learning for Predicting Severity of Side Effects. Vaccines. 2021; 9(6):556. https://doi.org/10.3390/vaccines9060556
Chicago/Turabian StyleHatmal, Ma’mon M., Mohammad A. I. Al-Hatamleh, Amin N. Olaimat, Malik Hatmal, Dina M. Alhaj-Qasem, Tamadur M. Olaimat, and Rohimah Mohamud. 2021. "Side Effects and Perceptions Following COVID-19 Vaccination in Jordan: A Randomized, Cross-Sectional Study Implementing Machine Learning for Predicting Severity of Side Effects" Vaccines 9, no. 6: 556. https://doi.org/10.3390/vaccines9060556