

Abstract
Objective. The relationship between osteoarthritis (OA) and osteoporosis (OP) remains controversial. An inverse relationship between spine OA and the presence of prevalent vertebral fractures has been shown in osteoporotic women. Our objective was to assess this relationship in osteoporotic men.
Methods. All the patients had OP based on densitometric data and were aged ≥ 65 years. Spine radiographs were performed according to a standardized procedure. Vertebral fractures were assessed from T4 to L4 by a semiquantitative method. Disc degenerative changes were assessed by the presence and severity of osteophytes and disc narrowing at levels T12–L1 to L5–S1. Logistic regression was used to study the relationship between the presence of vertebral fracture and lumbar disc degeneration.
Results. The study included 261 osteoporotic men. The prevalence of vertebral fractures was 26.4% (69/261). At least 1 osteophyte was found in 91.6% (239/261) of patients, and at least 1 disc space narrowing in 63.5% (165/260). The prevalence of at least 1 osteophyte and/or at least 1 disc space narrowing was similar in patients with and those without vertebral fracture. No relationship was found between the presence and/or the severity of osteophytes and disc narrowings and the presence of prevalent vertebral radiographic fractures.
Conclusion. In osteoporotic men, the prevalence of lumbar spine degeneration is high. There is no relationship between lumbar disc degeneration and the presence of vertebral fracture in osteoporotic men.
Osteoporosis (OP) and osteoarthritis (OA) are 2 common diseases, particularly in the elderly. The prevalence of spine OA varies according to the definition and the population1. There is no standard definition of disc degeneration, thus prevalence of spine OA remains difficult to determine2. The individual radiographic features are similar to those of peripheral OA joints (narrowing, osteophytes, sclerosis). According to the method of Kellgren, the prevalence of radiographic lumbar disc degeneration was 75.8% in a Japanese cohort3,4. In the Zoetermeer survey, the peak of prevalence of radiographic lumbar OA was 71.9% in men and 67.3% in women5.
Although much focus has been placed on cartilage degeneration in OA research, there is a growing interest in the role of bone in the development of OA. Different studies have shown an association between high bone mineral density (BMD) and OA of the hips, knees, or spine6,7,8,9,10. The relationship between OA and bone has a strong biological plausibility: Diarra, et al showed that Dickkopf-1 (DKK-1; an inhibitor of the Wnt pathway) is a regulator of joint remodeling11. They suggested that the mechanisms of joint destruction (such as narrowing) and construction (such as osteophytes) are regulated by determinants of bone metabolism, such as Wnt and DKK-1. Moreover, it has been shown in a mouse model that osteoprotegerin (OPG) might prevent cartilage degradation through its action on bone. Thus, modulating the receptor activator of nuclear factor-κB ligand (RANKL)/OPG balance could contribute to the prevention of cartilage degradation12. Antiosteoporotic treatments have been assessed in OA based on their effect on subchondral bone remodeling. In posthoc analysis, alendronate was associated with fewer spinal osteophytes and less progression of disc space narrowing13, and a posthoc analysis of data from strontium ranelate trials suggested reduced radiographic spinal OA progression in osteoporotic women with prevalent spinal OA14.
The relationship between spine OA and osteoporotic vertebral fractures is complex and 2 theories are in contradiction. One study suggested that disc space narrowing and osteophytes were associated with decreased prevalence of vertebral fracture in postmenopausal women with OP15. One explanation is that disc space narrowing and facet joint arthritis lead to a lower mobility of the affected segment, thus decreasing both the exposure of vertebrae to high stress and the risk of fractures. However, another study showed that disc space narrowing at the lower part of the lumbar spine was associated with an increased risk of vertebral fractures in postmenopausal women16. In this latter study, the hypothesis was that degenerative discs lead to alteration in load transfer between disc and vertebral body. Thus, the strain distribution is modified and the vertebral fracture risk increases.
To clarify the relationship between spinal OA and vertebral fractures, we designed this study in another population, i.e., osteoporotic men. The aim was to assess the prevalence and the characteristics of lumbar disc degeneration (both disc narrowing and osteophytes) in osteoporotic men and to assess the relationship between lumbar disc degeneration and prevalent vertebral fractures in this population.
MATERIALS AND METHODS
Patients
Baseline data of a prospective study of men with OP were used for this analysis. That study aimed to assess the effect of an antiosteoporotic treatment on BMD. Our study was approved by the appropriate ethics committee and was performed in accord with the ethical standards of the 1964 Declaration of Helsinki and its later amendments.
All the patients were ambulatory white men at least 65 years of age. All gave written consent for the study. They had no life-threatening diseases, no severe liver or renal insufficiency, no other bone disease, and no treatment likely to interfere with bone metabolism.
They were osteoporotic on the basis of BMD measured by dual-energy X-ray absorptiometry (DEXA) at the spine and femoral neck. The BMD criteria were a mean lumbar spine (L2–L4) BMD ≤ 0.840 g/cm2 or a femoral neck BMD ≤ 0.600 g/cm2, measured with a Hologic apparatus, or a mean lumbar spine BMD ≤ 0.949 g/cm2 or a femoral neck BMD ≤ 0.743 g/cm2, measured using a Lunar apparatus. These criteria were based on the well known differences in absolute values among manufacturers. Presence of a vertebral fracture was not required as an inclusion criterion. Use of an antiosteoporotic treatment before the study was an exclusion criterion. None of the inclusion/exclusion criteria were based on back pain or radiographic OA measures.
Assessment of vertebral fractures
Spine radiographs were performed in each investigator center by specifically trained technicians according to standardized procedures for image acquisition. Radiographs were sent to a single central reading facility (Centre d’Evaluation des Maladies Osseuses CEMO, Cochin Hospital, Paris) for confirmation of the quality of radiographs and evaluation of vertebral fractures. Vertebrae from T4 to L4 were evaluated to determine the presence and grades of fractures according to Genant’s semiquantitative method17,18. This grading was performed on 3 lateral views: thoracic (T4–L1), thoraco-lumbar junction, and lumbar (T12–L4) views of the spine radiographs. A fracture was defined as a grade ≥ 1. Careful attention was paid to diagnosis of vertebral deformities of nonosteoporotic origin15,18, excluding from the diagnosis of fracture all the wedge deformities at the thoracic spine without evidence of a fracture in the middle part of the vertebral endplate. Deformities with isolated short vertebral anterior heights were excluded from the diagnosis of fracture.
Assessment of lumbar disc degeneration
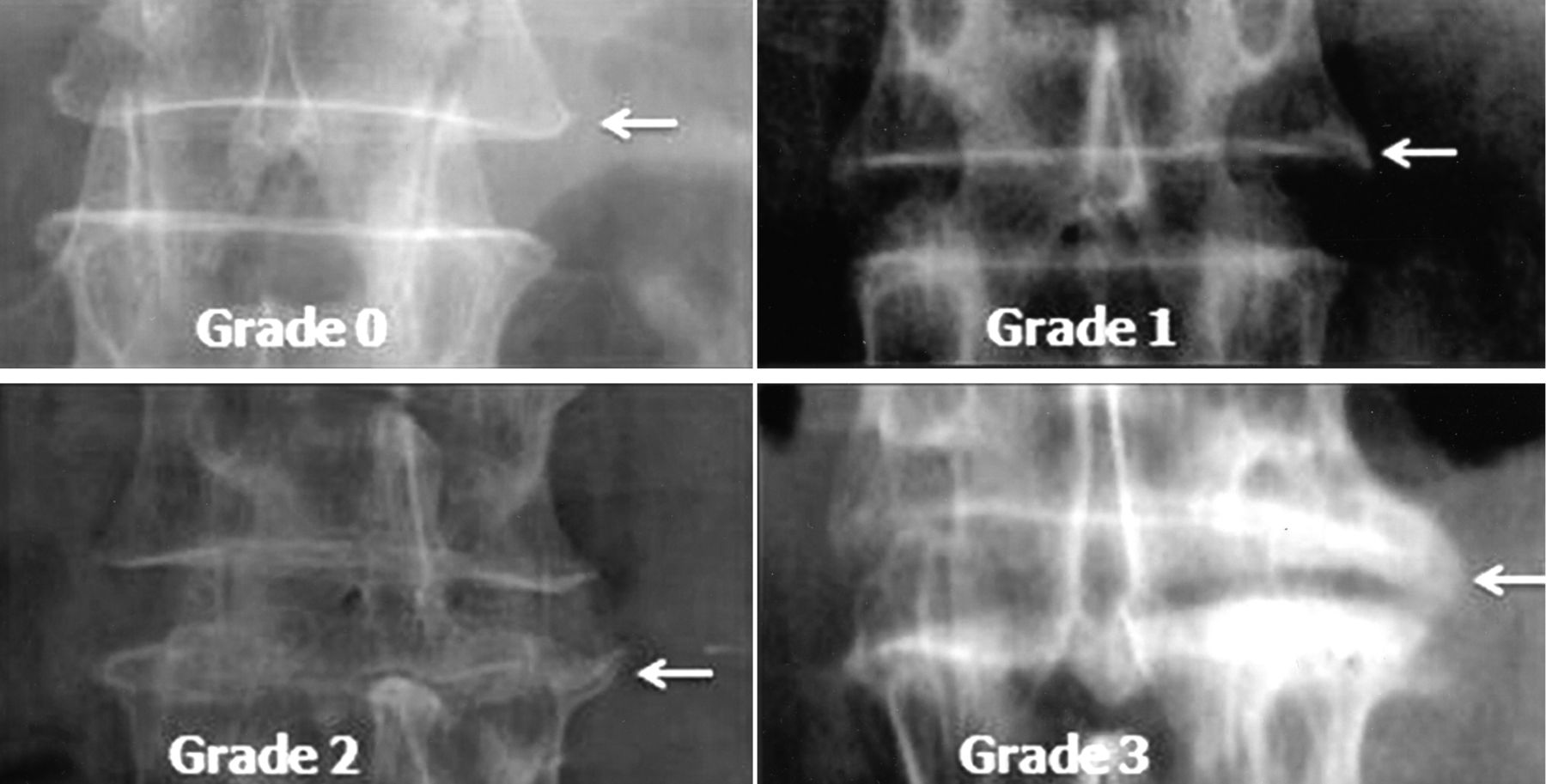
We used a method adapted from Lane, et al19. We defined lumbar disc degeneration as the presence and severity of osteophytes (anterior and lateral) and disc space narrowing. The intervertebral spaces involved were T12–L1 to L5–S1 for the lateral views and T12–L1 to L4–L5 for the anteroposterior view. Each intervertebral space was assigned 1 of 4 grades according to the presence and severity of osteophyte and disc space narrowing (Table 1). For each level, the highest grade between anterior osteophytes and lateral osteophytes was retained. Neither the posterior osteophytes nor the sclerosis of the vertebral endplates or the facet joint arthritis were assessed. Lane, et al assessed both thoracic and lumbar disc degeneration. However, only the 2 worst or more involved intervertebral levels from T4–T5 to T12–L1 were scored in detail19. Thus, we have assessed only the lumbar spine disc degeneration from T12–L1 to L5–S1.
Individual radiographic features on lumbar spine film.
An atlas of standard radiographic disc degeneration findings, adapted from Lane, was developed for self-training before starting the reading and consulted while reading to maintain consistency (Figure 1).


A. Anterior osteophytes, lateral view. B. Disc space narrowing.
C. Lateral osteophytes, anteroposterior view.
The radiographs were read by 2 trained expert assessors. One assessor read the vertebral fractures and the other read the lumbar spine disc degeneration. Interrater reliability was not assessed, because the assessors did not read the same radiographic features. The assessors were not blinded to the purpose of the study but were blinded to the treatment.
BMD measurement
BMD was measured by DEXA at the lumbar spine and hip. The densitometry operators had to be specifically trained by the DEXA central reading center team to ensure that each center used a standard acquisition procedure. To obtain optimum concordance between measurements of the different centers, each machine was cross-calibrated, using an external phantom (European Spine Phantom), by the DEXA central reading center. Lumbar vertebral fractures were excluded from the analyses.
Statistical methods
All the analyses were performed on SAS 9.1 (SAS Institute). Results were expressed in mean ± SD for the continuous variables and in percentage for binary variables. Differences between populations of patients (vertebral fracture vs no vertebral fracture) were analyzed by applying the nonparametric Wilcoxon test for the continuous variables and applying Fisher’s exact test for binary variables. Logistic regression (univariate and adjusted for age, BMI, and BMD) was performed to quantify, through OR estimations, the strength of the association between the risk of vertebral fracture and the number, severity, and location of disc degeneration. OR were computed with 95% CI. The kappa statistic was used to examine intraobserver agreement. A p value < 0.05 was considered significant.
RESULTS
Characteristics of the patients are reported in Table 2. They were on average 73.4 years old. The characteristics were similar between patients with and those without vertebral fracture.
Characteristics of the patients. Values are mean (SD).
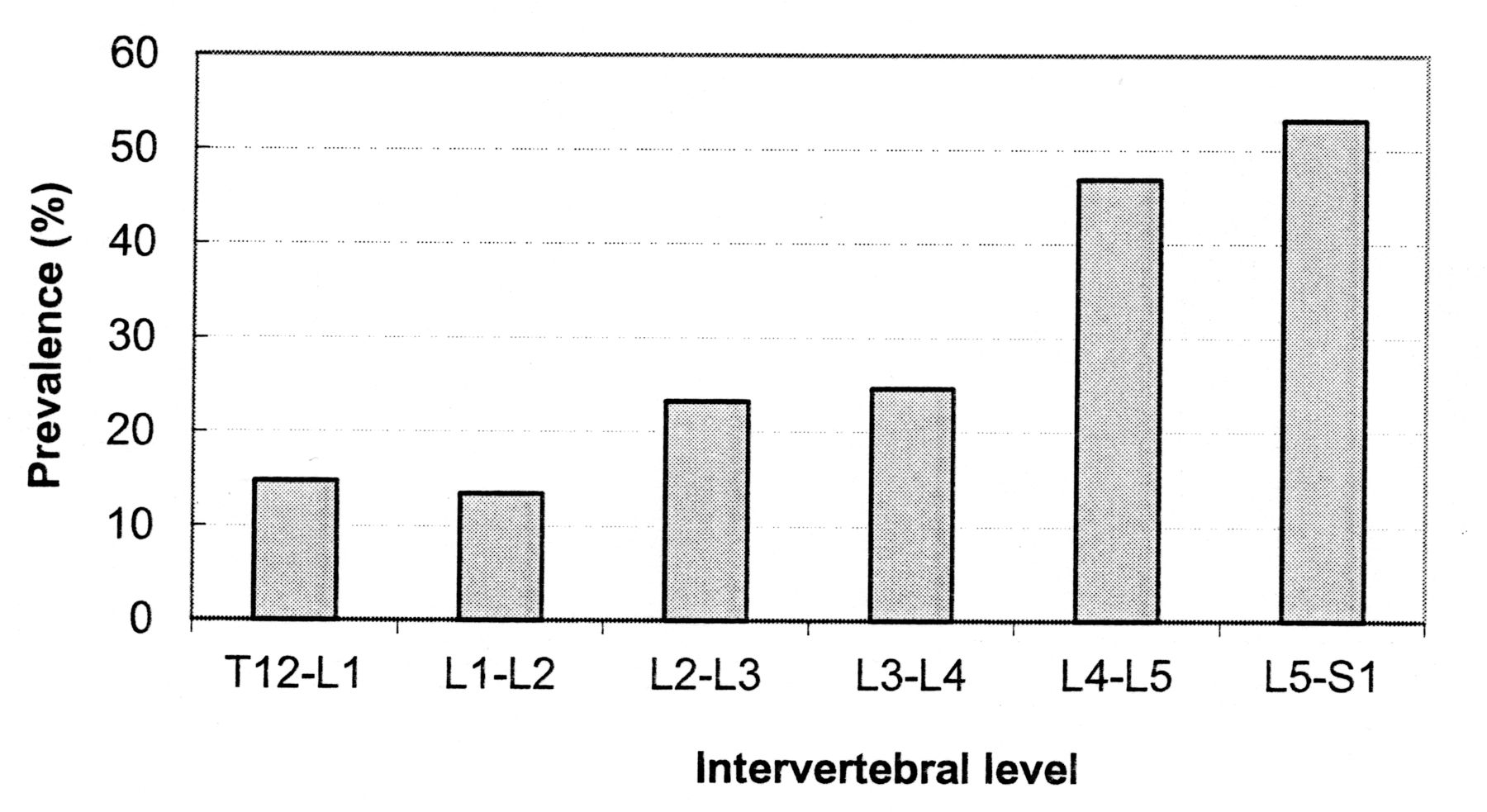
A total of 26.4% (69/261) of patients had fracture (grade ≥ 1) and 8.8% (23/261) had at least 1 grade 3 fracture. The mean (SD) number of fractures was 0.5 (1.2). The prevalence of vertebral fractures according to the vertebral level is shown in Figure 2 for the 69 patients with such fractures. This distribution is similar to that observed in populations of postmenopausal women.

Prevalence of vertebral fractures by location in 69 men.
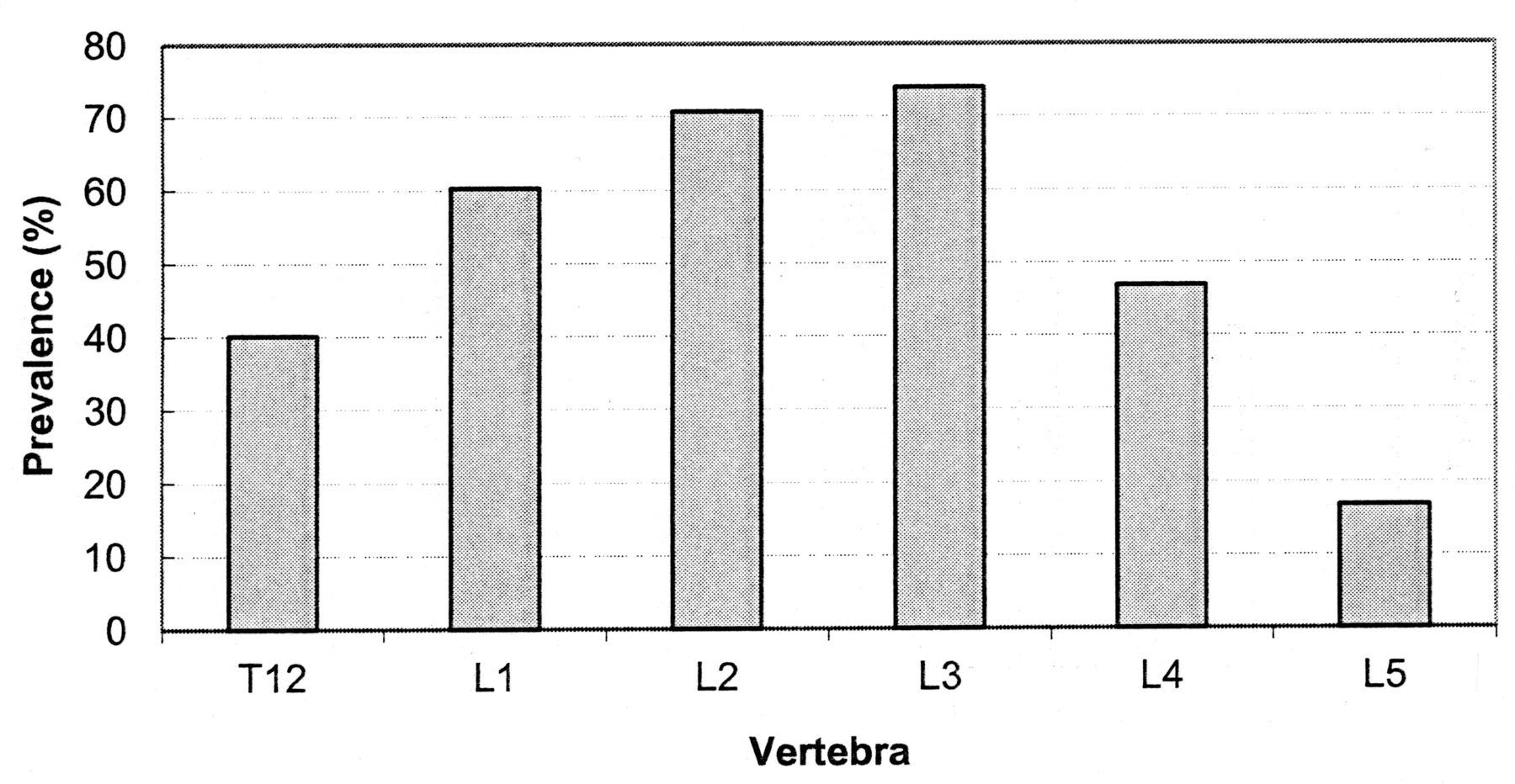
The prevalence of disc degeneration was high: 91.6% of patients had at least 1 osteophyte (239/261; 95% CI 88% to 95%) and 63.5% had at least 1 disc space narrowing (165/260; 95% CI 58% to 69%). Mean number (SD) of osteophytes was 2.8 (1.5), and 69.3% of patients had at least 1 osteophyte of grade ≥ 2 (181/261; 95% CI 64% to 75%; Table 3). The prevalence of osteophytes according to the vertebral level is presented in Figure 3. Mean (SD) number of disc narrowings was 1.1 (1.1), and 39.6% had at least 1 disc space narrowing of grade ≥ 2 (103/260; 95% CI 34% to 46%; Table 3). The prevalence of disc narrowings according to the intervertebral level is presented in Figure 4.

Prevalence of osteophytes by level in 239 men with at least 1 osteophyte.
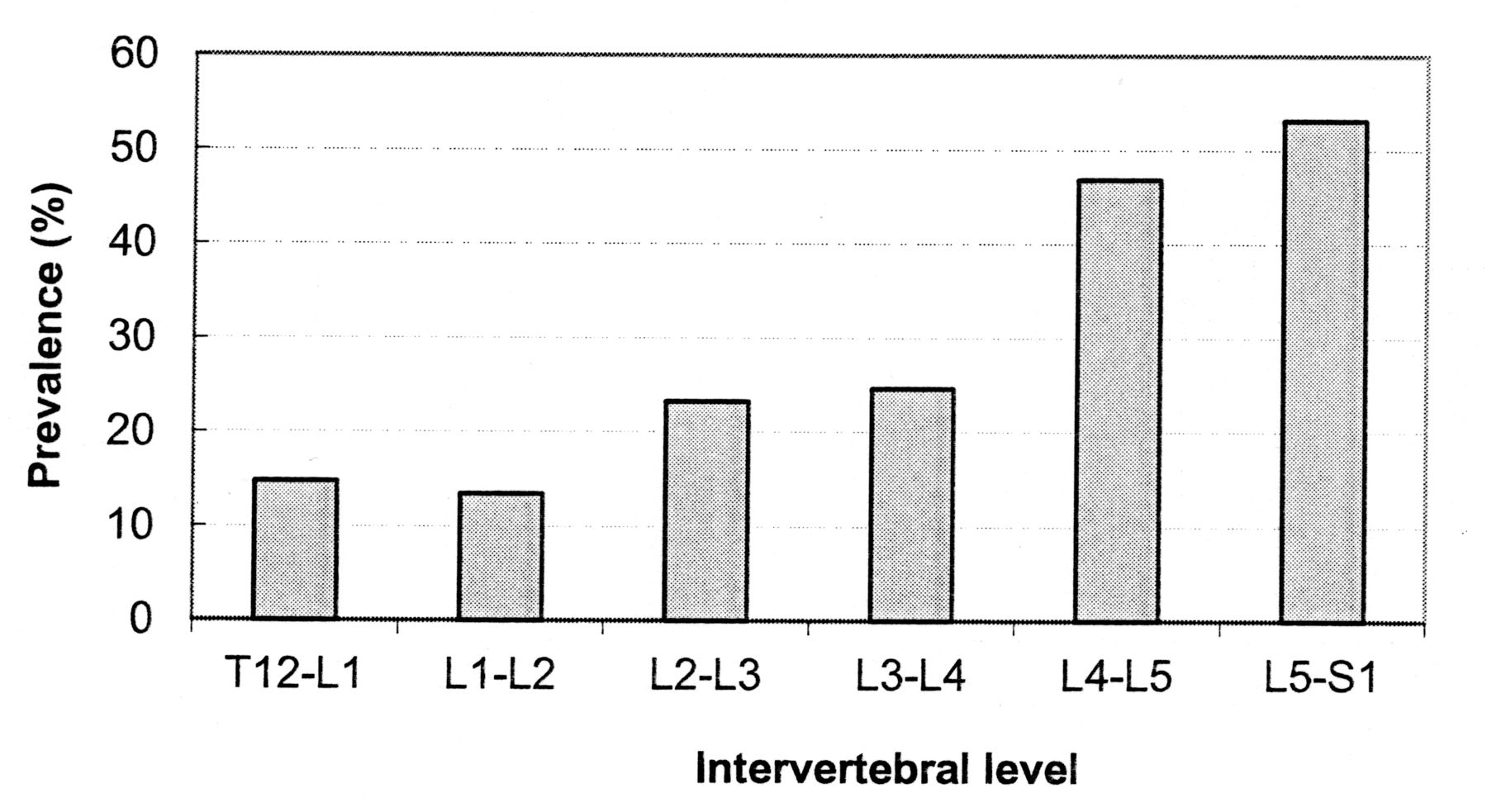
Prevalence of disc narrowing by location in 160 men with at least 1 disc narrowing.
Description of osteophytes and disc space narrowings.
The prevalence of at least 1 osteophyte and/or at least 1 disc narrowing was similar in patients with and those without any vertebral fracture (Table 4). No association was found between the presence and/or severity of lumbar disc degeneration (osteophytes and disc space narrowing) and the presence of prevalent vertebral fractures (Table 5).
Prevalence of at least 1 osteophyte and/or disc narrowing.
Relationship between vertebral fractures and lumbar spine degeneration.
DISCUSSION
Our data show a high prevalence of lumbar disc degeneration in men selected on the diagnosis of OP, i.e., having a low BMD, with a mean age of 74 years. These data are consistent with studies in men aged ≥ 50 years from the general population. Indeed, de Schepper, et al showed a prevalence of lumbar osteophytes and disc narrowings of 95% and 53%, respectively, and Liu, et al showed a prevalence of 75% and 43%, respectively20,21. In a Japanese cohort, the prevalence of radiographic lumbar OA with Kellgren-Lawrence score ≥ 2 was 84% in men ≥ 60 years old4. The variations in prevalence rates between studies are due to the number of disc levels included, the different definitions of disc degeneration, and population differences.
In our study, the distribution of osteophytes and disc space narrowing was comparable to that described in the general population. Indeed, we found a high prevalence of osteophytes at L3, similar to other studies22. This distribution coincides with the zone of maximum lumbar curvature with important loads in standing position. Moreover, we found that disc narrowings were more common in L4-L5 and L5-S1, which is in accord with previous studies20. Mechanical factors could explain this latter finding, because the lower lumbar levels are used more in biomechanical applications. Thus, our results suggest that the underlying OP modifies neither the prevalence nor the distribution of lumbar disc degeneration in men. This result is confirmed while using a conservative threshold for spinal OA definition as the presence of at least 2 disc narrowings or 2 osteophytes. In a Chinese study of men and women, there was no evidence that OP protected against or predisposed to disc degeneration23.
In the absence of a control group we cannot draw conclusions about the frequency of OA in osteoporotic versus nonosteoporotic men. Our study was designed to assess OA in an osteoporotic population, because 2 studies previously found contradictory results on the association between OA and vertebral fractures15,16. Those studies, conducted in women, found either a positive or a negative association. In contrast, we did not find any relationship between disc degeneration (assessed in the lumbar spine) and the presence of vertebral fractures; these discrepancies could be explained by different factors involved in the pathogenesis of OP and spine OA in the 2 sexes. Hormonal factors could play a different role in men and women. Indeed, menopause is associated with an increase in OA prevalence and the role of estrogen deficiency has been suggested in OA24. In some studies, 17β-estradiol and testosterone receptors have been localized in human intervertebral discs of men and women25,26. Yet the exact role of sex hormones in the physiopathology of OA remains uncertain. In a prospective study of women, no association was found between use of hormone replacement therapy or multiparity and incident disc degeneration27. Mechanical spine factors could differ in the 2 sexes. Men are more physically active than women28, and heavy physical loading has long been suspected as a risk factor for disc degeneration. However, studies have shown that heredity appears to play a dominant role in lumbar disc degeneration2. Moreover, altered expression of sets of genes may in part explain the sex disparity observed in OA. Indeed, a subset of genes involved in osteoclast function was identified as being differentially expressed in OA bone between women and men29. In a review, Kauppila found an association between atherosclerosis and disc degeneration30, suggesting that unequal cardiovascular risk between men and women could be a determinant of the differences in the physiopathology of spine OA.
To our knowledge, this is the first study to describe the prevalence and characteristics of lumbar spine degeneration in osteoporotic males. Radiographs were performed using a standardized method and all the vertebral fractures were assessed by a single expert. Lumbar spine degeneration was assessed by another expert. The grading system of Lane was recommended for use in epidemiological studies, because its intraclass correlation coefficient for interobserver reliability was > 0.60, except for sclerosis19,31. Moreover, Lane’s atlas has the advantage of allowing separate assessment of disc narrowings and osteophytes. It seems important to describe these radiographic features separately, because their pathogenesis might be different.
Our study has several limitations. The study design is cross-sectional, therefore no temporal or causal inference can be made. Apart from T12-L1 level, thoracic spine degeneration was not assessed, which underestimates the prevalence of spine disc degeneration. Neither endplate sclerosis nor facet joint degeneration was assessed, underestimating the prevalence of spine OA. Moreover, the study was not a priori powered to detect a significant difference. The number of patients was limited and the results apply to only a selected population.
OP and lumbar disc degeneration can coexist in men, and this study suggests the absence of a relationship between vertebral fractures and spine OA in this population.
- Accepted for publication February 20, 2013.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}