

Abstract
Objective. Magnetic resonance imaging (MRI) is increasingly used in rheumatoid arthritis (RA) research. A European League Against Rheumatism (EULAR) task force recently suggested that MRI can improve the certainty of RA diagnosis. Because this recommendation may reflect a tendency to use MRI in daily practice, thorough studies on the value of MRI are required. Thus far no large studies have evaluated the accuracy of MRI to differentiate early RA from other patients with early arthritis. We performed a large cross-sectional study to determine whether patients who are clinically classified with RA differ in MRI features compared to patients with other diagnoses.
Methods. In our study, 179 patients presenting with early arthritis (median symptom duration 15.4 weeks) underwent 1.5T extremity MRI of unilateral wrist, metacarpophalangeal, and metatarsophalangeal joints according to our arthritis protocol, the foot without contrast. Images were scored according to OMERACT Rheumatoid Arthritis Magnetic Resonance Imaging Scoring (RAMRIS) by 2 independent readers. Tenosynovitis was also assessed. The main outcome was fulfilling the 1987 American College of Rheumatology (ACR) criteria for RA. Test characteristics and areas under the receiver-operator-characteristic curves (AUC) were evaluated. In subanalyses, the 2010 ACR/EULAR criteria were used as outcome, and analyses were stratified for anticitrullinated protein antibodies (ACPA).
Results. The ACR 1987 criteria were fulfilled in 43 patients (24.0%). Patients with RA had higher scores for synovitis, tenosynovitis, and bone marrow edema (BME) than patients without RA (p < 0.05). ACPA-positive patients had more BME (median scores 6.5 vs. 4.25, p = 0.016) than ACPA-negative patients. For all MRI features, the predictive value for the presence of RA was low (< 50%). For all MRI features the AUC were < 0.70. Patients who fulfilled ACR/EULAR 2010 criteria but not ACR87 criteria for RA had less synovitis than patients who were positive for RA according to both sets of criteria (p = 0.029).
Conclusion. Although patients with RA had higher scores of MRI inflammation and ACPA-positive patients had more BME, the severity of MRI inflammation assessed according to RAMRIS does not accurately differentiate patients with RA from other early arthritis patients.
Early identification of rheumatoid arthritis (RA) is important because early initiation of aggressive treatment results in a better outcome1. However, this requires that patients with RA be identified among other patients with early arthritis. Magnetic resonance imaging (MRI) in RA is mainly used for research purposes. The value of MRI is supported by its sensitivity to depict changes that are not detectable by physical examination, and the association of bone marrow edema (BME) with radiographic progression over time2. A recent European League Against Rheumatism (EULAR) task force recommended that in case of diagnostic doubt, MR imaging can improve the certainty of a diagnosis of RA3. Because this recommendation may reflect a tendency to use MRI in daily practice, thorough studies on the value of MRI in a general setting of patients with early arthritis are required. To date, no large studies to our knowledge have evaluated the accuracy of MRI to differentiate patients with RA from patients with early arthritis and other diagnoses. The majority of studies performed on the diagnostic accuracy primarily evaluated patients with undifferentiated arthritis (UA) or RA, but not the entire spectrum of early arthritis patients4,5. Further, those studies included a low number of patients with early arthritis (< 50) and reported variable test characteristics (the sensitivity and specificity of certain MR imaging findings ranged between 20–100% and 0–100%).
At present, the accuracy of MRI to differentiate patients with RA from other patients with early arthritis is unclear. We performed a large cross-sectional study to determine this. The outcome was the diagnosis according to classification criteria at 2 weeks. On purpose we did not explore the additional value of MRI when added to clinical diagnoses. We started with a more basic question: whether patients who are clinically classified with RA differ in MRI features compared to patients with other diagnoses. Because these patients are clinically distinctive, among other characteristics in the joints that are typically involved and the extent of inflammation, we anticipated finding differences at 1.5T extremity MRI of the joints most frequently involved in RA. These findings will serve as a basis for further analyses in the current cohort of patients.
MATERIALS AND METHODS
Patients
Patients were included in the Leiden Early Arthritis Clinic (EAC). Inclusion required the presence of clinically confirmed arthritis of ≥ 1 joint and symptoms for ≤ 2 years. Variables collected at inclusion were medical history, questionnaires, joint counts, laboratory tests, and radiographs of hands and feet6. Anticitrullinated protein antibodies (ACPA) were measured (Eurodiagnostica). After 2 weeks, when the laboratory results were known, patients were diagnosed with RA or other diagnoses according to existing classification criteria, blinded to magnetic resistance (MR) findings. RA was classified according to the 1987 criteria; in subanalyses RA according to the 2010 criteria was also studied as outcome. These cross-sectional data were studied.
From August 2010 until April 2012, 350 patients were included in the EAC. MR imaging was performed in 179 patients based on voluntary participation. The patients with and without MR did not significantly differ in age, sex, symptom duration, or ACPA status (data not shown). This study was approved by the local ethical committee. All patients signed informed consent.
MR imaging
MR imaging of the hand (wrist and metacarpophalangeal joints) and forefoot (metatarsophalangeal joints) was performed within 2 weeks after inclusion, at the most painful side, or in case of completely symmetric symptoms, at the dominant side. The presence of clinical arthritis at physical examination of the joints that were scanned was not a prerequisite. There were 2 patients excluded because of contraindications for MR imaging. Patients with impaired renal function, or known hypersensitivity, or allergic reactions to contrast media were imaged without contrast administration (n = 2).
MR imaging was performed on an MSK Extreme 1.5T extremity MR imaging system (General Electric) using a 145 mm coil for the foot and a 100 mm coil for the hand. The patient was positioned in a chair beside the scanner, with the hand or foot fixed in the coil with cushions.
The forefoot was scanned using a T1-weighted fast spin-echo (FSE) sequence in the axial plane with repetition time (TR) of 650 ms, echo time (TE) 17 ms, acquisition matrix 388 × 288, echo train length (ETL) 2, and a T2-weighted FSE sequence with frequency selective fat saturation in the axial plane (TR/TE 3000/61.8; acquisition matrix 300 × 224, ETL 7). Due to time constraints, imaging of the foot was limited to precontrast sequences only.
In the hand, the following sequences were acquired before contrast injection: T1-weighted FSE sequence in the coronal plane (TR/TE 650/17 ms, acquisition matrix 388 × 88, ETL 2); T2-weighted FSE sequence with frequency selective fat saturation in the coronal plane (TR/TE 3000/61.8 ms, acquisition matrix 300×224, ETL 7). After intravenous injection of gadolinium contrast (gadoteric acid, Guerbet, standard dose 0.1 mmol/kg) the following sequences were obtained: T1-weighted FSE sequence with frequency selective fat saturation in the coronal plane (TR/TE 650/17 ms, acquisition matrix 364×224, ETL 2), T1-weighted FSE sequence with frequency selective fat saturation in the axial plane (TR/TE 570/7 ms, acquisition matrix 320×192, ETL 2).
Field-of-view was 100 mm for the hand and 140 mm for the foot. Coronal sequences had 18 slices with a slice thickness of 2 mm and a slice gap of 0.2 mm. All axial sequences had a slice thickness of 3 mm and a slice gap of 0.3 mm, with 20 slices for the hand and 16 for the foot. Total imaging time was approximately 75 minutes.
MR imaging scoring
MR images were scored by 2 readers (WS and AK), blinded to clinical data. Each reader separately analyzed each set of images and the mean total scores for each feature of both readers were used for further analyses. Synovitis, BME, and erosions were scored semiquantitatively according to OMERACT Rheumatoid Arthritis Magnetic Resonance Imaging Scoring (RAMRIS) definitions and score. Tenosynovitis in the metacarpophalangeal (MCP) and wrist joints was evaluated using the method proposed by Haavardsholm, et al with tenosynovitis assessed for the flexor and extensor tendons of each MCP joint at the same 0–3 scale as for the wrist7. Tenosynovitis was not assessed in the foot because of the lack of axial images.
Total RAMRIS score was defined as the total of all scores including tenosynovitis. Some joints could not be completely scored due to insufficient image quality (1.1% of all individual scores), in most cases due to incomplete fat suppression or movement artifacts. In these cases, values were imputed with the median value for that feature across all joints or bones within the same patient. The interreader reliability was assessed by computing the intraclass correlation for total scores of each MR imaging parameter. In addition, a subset of 25 randomly selected MR image sets (14.0%) was scored twice by each reader to determine intrareader ICC. Intrareader ICC for total RAMRIS-score were 0.98 for reader 1 and 0.83 for reader 2, and interreader ICC for total RAMRIS-score was 0.89. For synovitis intrareader, ICC were 0.93 and 0.64, and interreader ICC 0.65; for tenosynovitis 0.91, 0.93, and 0.90; for BME 0.96, 0.72, and 0.86; and for erosions 0.89, 0.65, and 0.76 respectively.
Statistical analysis
The Wilcoxon Rank Sum and Kruskal-Wallis tests were used where appropriate. To evaluate the discriminative ability of MRI, areas under the receiver-operator-characteristic curves (AUC), test characteristics, and positive and negative likelihood ratio (LR+, LR–) were assessed. Optimal cutoff points for dichotomization were determined per MRI feature using Youden’s method8. Analyses were performed using R, version 2.15.0 (R Development Core Team). P-values < 0.05 were considered significant.
RESULTS
Patient characteristics
Of the 179 patients, 99 were female (55.3%). The median age was 57 years [interquartile range (IQR) 20], the median symptom duration 15.4 weeks (IQR 21), and 45 (25.1%) of the patients were ACPA-positive. Patients were classified according to the following diagnoses: 1987-RA 43 (24.0%), undifferentiated arthritis 88 (49.2%), inflammatory osteoarthritis 12 (6.7%), psoriatic arthritis 15 (8.4%), and other rheumatic diagnoses 21 (11.7%). The patient characteristics per diagnosis are presented in Table 1.
Patient characteristics per diagnosis.
MRI scores per group of diagnoses
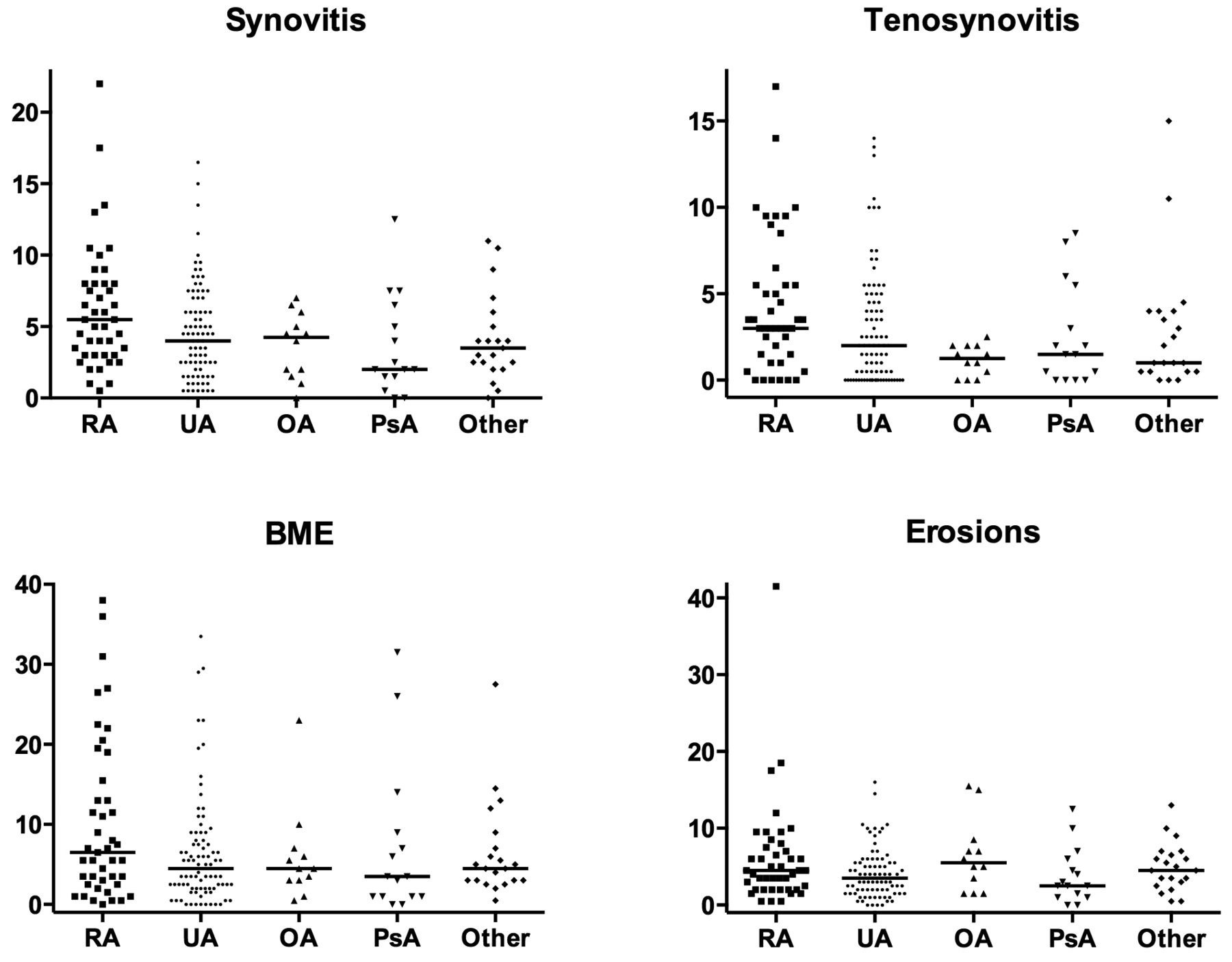
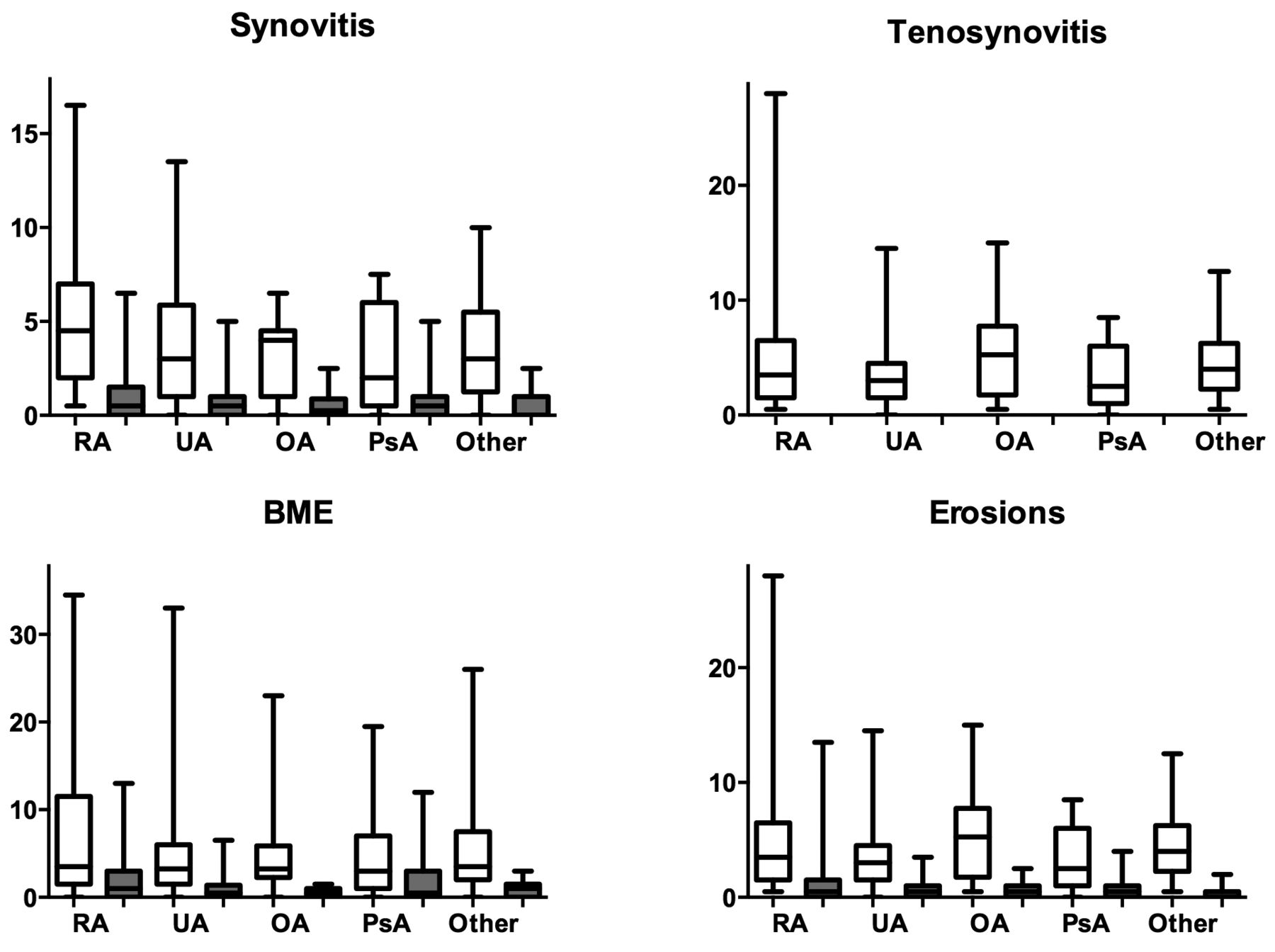
The median scores for synovitis, BME, erosions, and tenosynovitis per joint group are presented in Table 2. Figure 1 depicts the scores for patients with different diagnoses. Scores for synovitis, tenosynovitis, and BME seemed higher in patients with RA than in patients with early arthritis and other diagnoses (Figure 1). Subsequently, we tested whether patients with RA had different MR imaging results than patients with other diagnoses. These differences were statistically significant when comparing RA with all patients with other diagnoses. The median scores for RA and other diagnoses were respectively 5.5 and 4.0 for synovitis (p = 0.003), 3.0 and 1.5 for tenosynovitis (p = 0.005), and 6.5 and 4.5 for BME (p = 0.038). The erosion scores were not statistically significantly different (4.5 and 3.5 for RA and other diagnoses respectively, p = 0.15).

RAMRIS scores for the different MRI features per group of diagnoses. Horizontal lines represent median values. Total RAMRIS: sum of synovitis, tenosynovitis, BME, and erosion scores. RA: rheumatoid arthritis; UA: undifferentiated arthritis; OA: inflammatory osteoarthritis; PsA: psoriatic arthritis; other: other rheumatic diagnoses including reactive arthritis (n = 6), spondylarthropathy (n = 3), gout (n = 2), pseudogout (1), palindromic arthritis (n = 1), paramalignant arthritis (n = 1), lyme disease (n = 1), systemic lupus erythematosus (n = 1), remitting seronegative symmetrical synovitis with pitting edema (n = 1), sarcoidosis (1), and unspecified other (n = 3); RAMRIS: Rheumatoid Arthritis Magnetic Resonance Imaging Scoring; BME: bone marrow edema.
Median values for the total RAMRIS and the individual features and the diagnostic accuracy to differentiate RA from other diagnoses per MRI feature. Scores per feature by joint area, median (IQR) values. The cutoffs to dichotomize the scores were 1.75 for synovitis, 2.75 for tenosynovitis, 10.50 for BME, and 5.75 for erosion.
Accuracy of MR imaging in differentiating RA from other diagnoses
The accuracy to differentiate patients with RA from patients with other diagnoses was evaluated by determining the test characteristics and the AUC (Table 2). In the presence of a certain MRI feature, the chance that this patient had RA was low (low positive predictive value). The AUC of all features were lower than 0.70.
RA according to the 1987 ACR or 2010 ACR/EULAR criteria
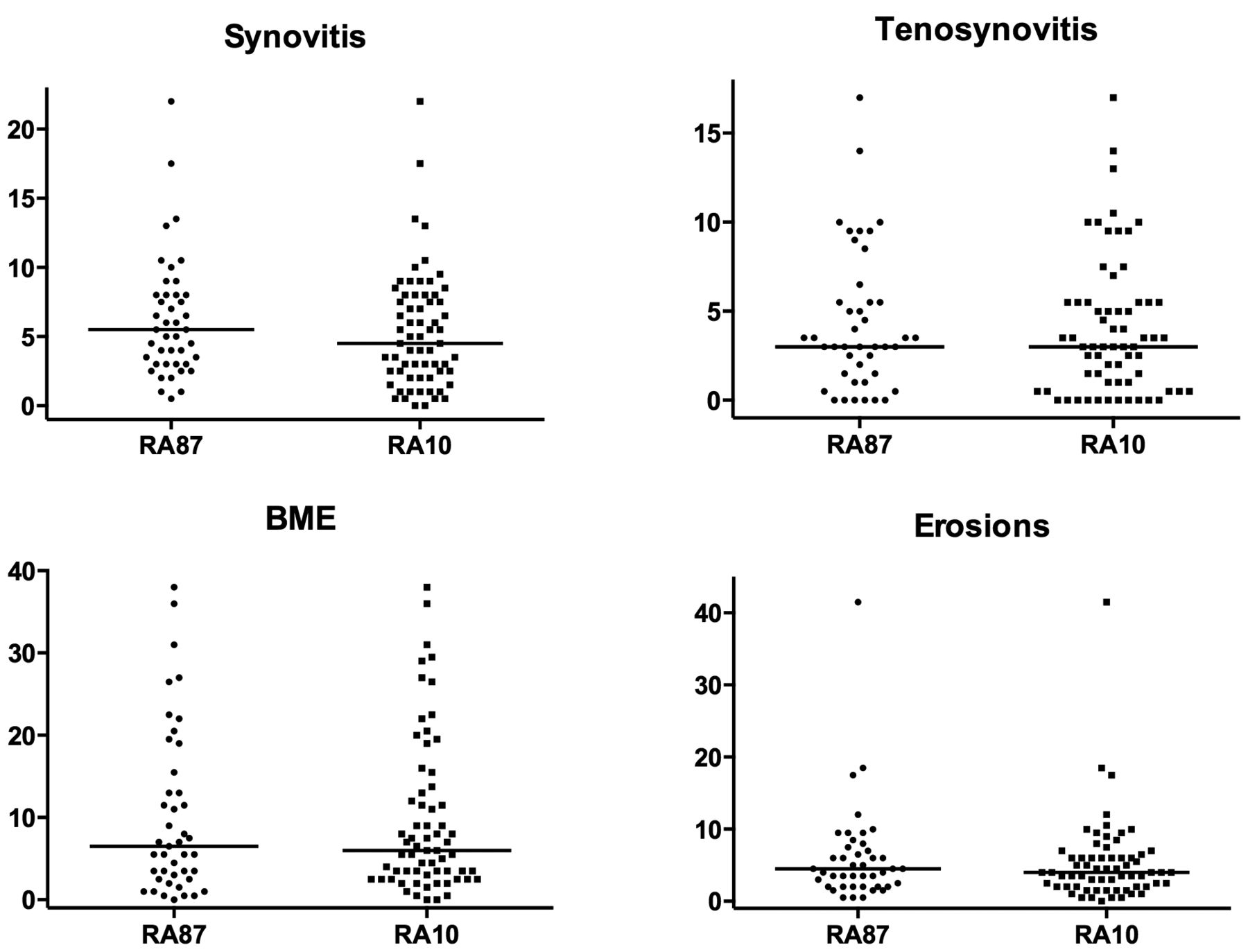
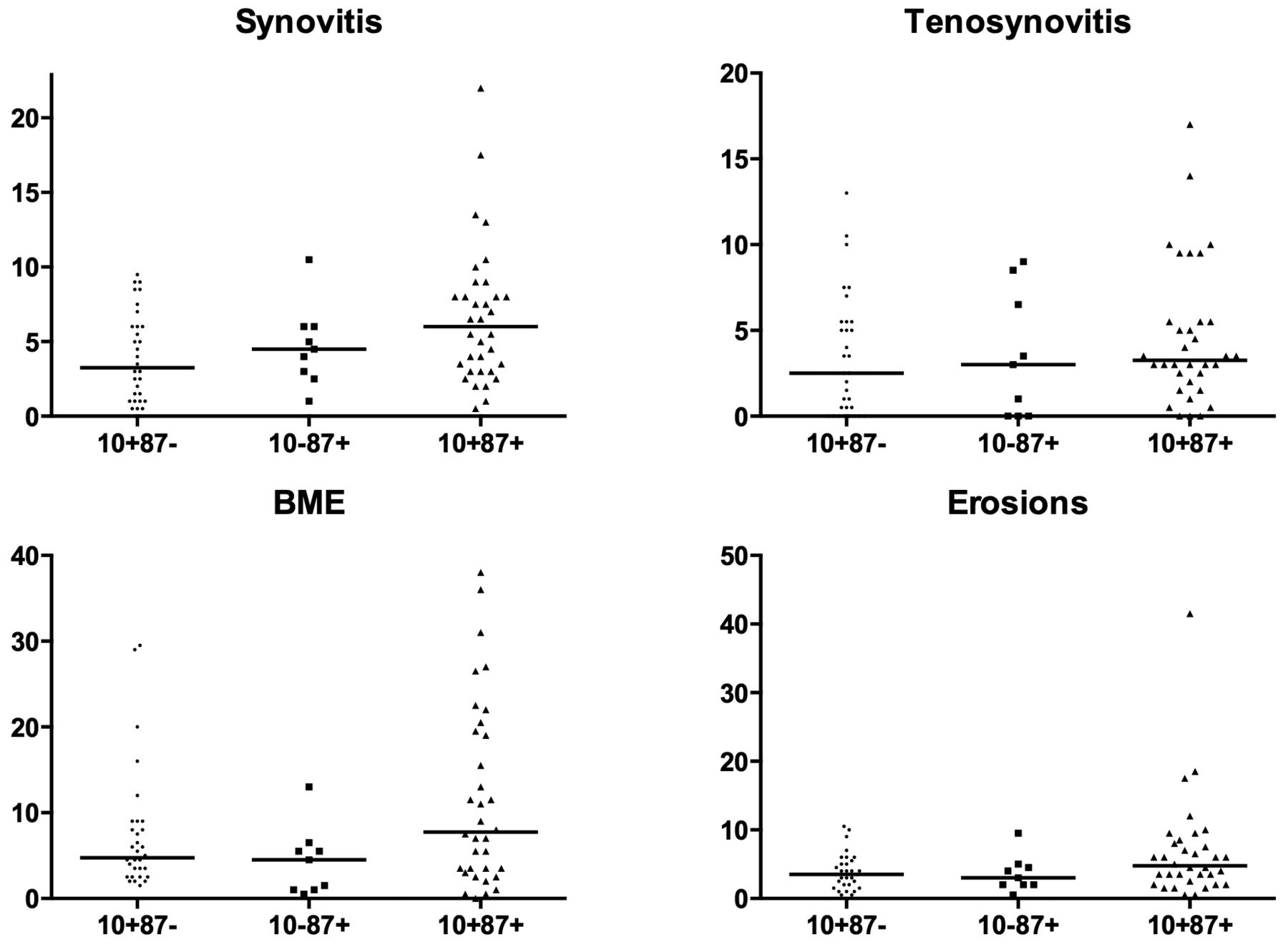
We subsequently questioned whether the results would be different when the 2010 criteria would be used to classify RA. Analyses were repeated with 2010 RA as outcome, yielding similar results (Appendix 1). Because many patients classified positive on both criteria sets, we also compared patients with RA that were 1987+/2010+ (n = 34), 1987+2010– (n = 9), and 1987–/2010+ (n = 32; patients with clear diagnoses other than RA and UA were not included). This showed that 1987–/2010+ patients had lower synovitis scores (median 3.25 vs 6.0, p = 0.029) than 1987+/2010+ patients (Appendix 2). No differences were found between 1987+/2010+ and 1987+/2010– patients with RA.
ACPA-positive versus ACPA-negative arthritis
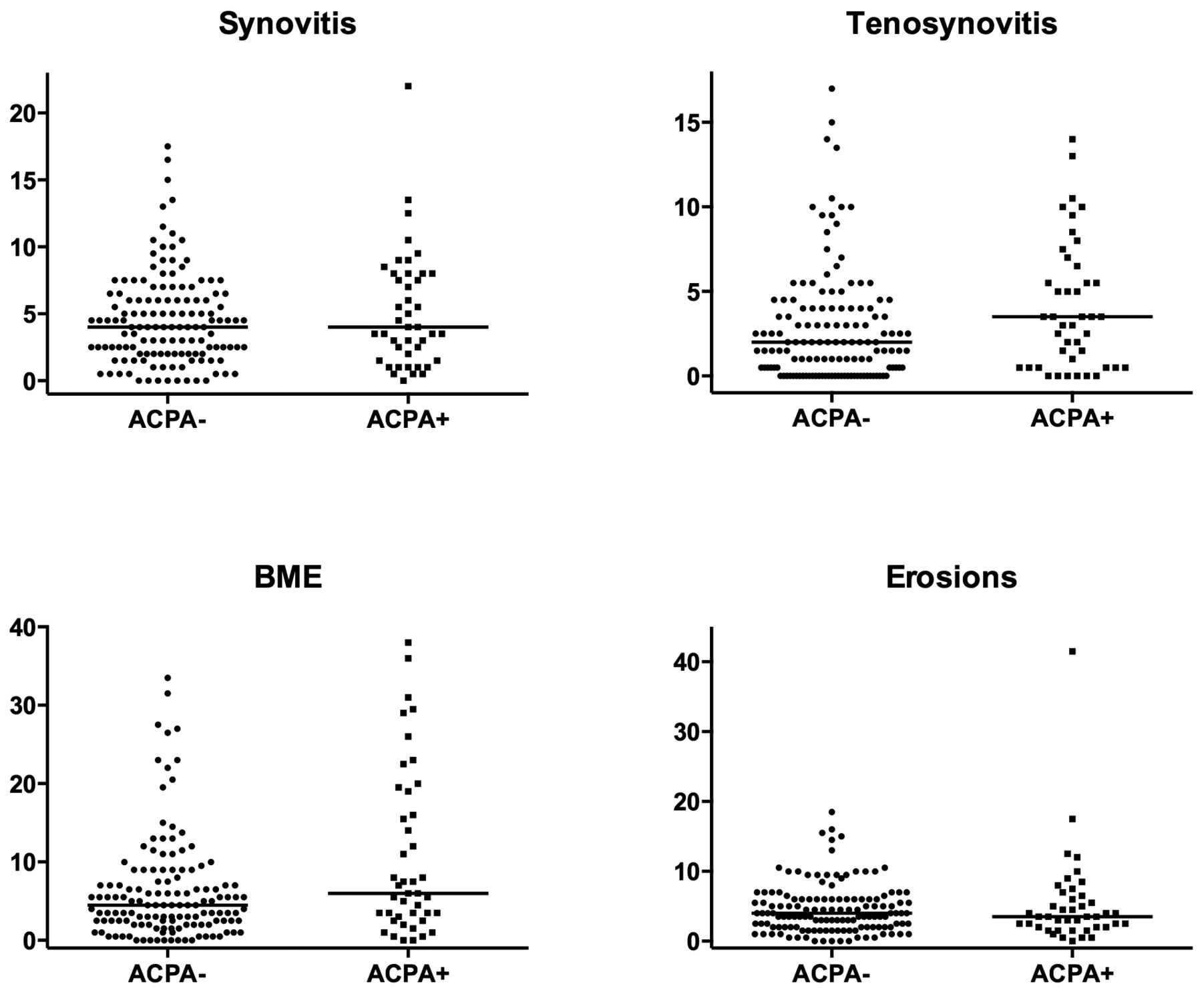
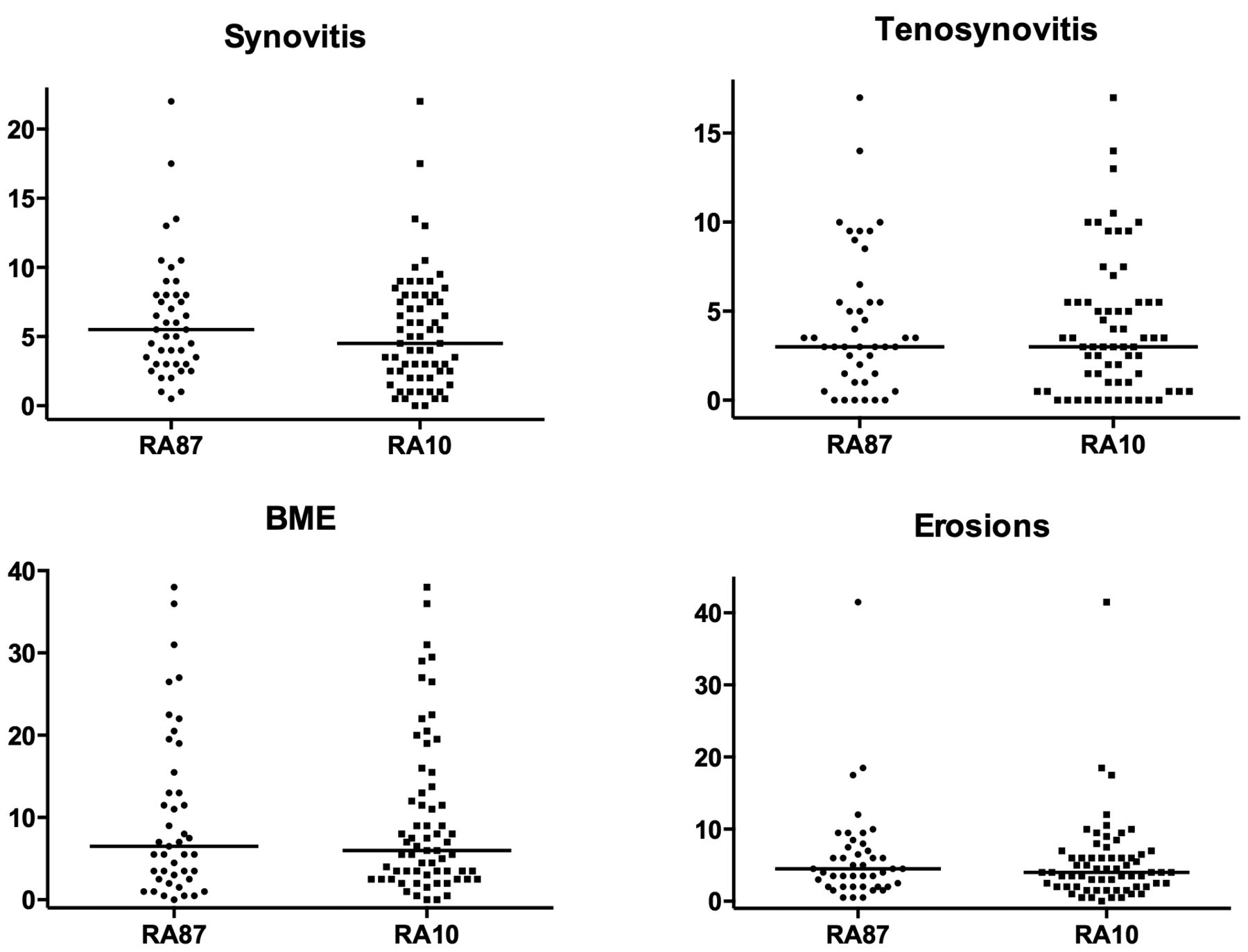
We evaluated whether patients with RA and patients with UA (according to the 1987 criteria) with (n = 39) or without ACPA (n = 92) had differences in scores. ACPA-positive patients showed higher scores for BME (median 6.5) than ACPA-negative patients (median 4.25, p = 0.016). However, no differences in the extent of synovitis, tenosynovitis, and erosions scores were observed (Figure 2).
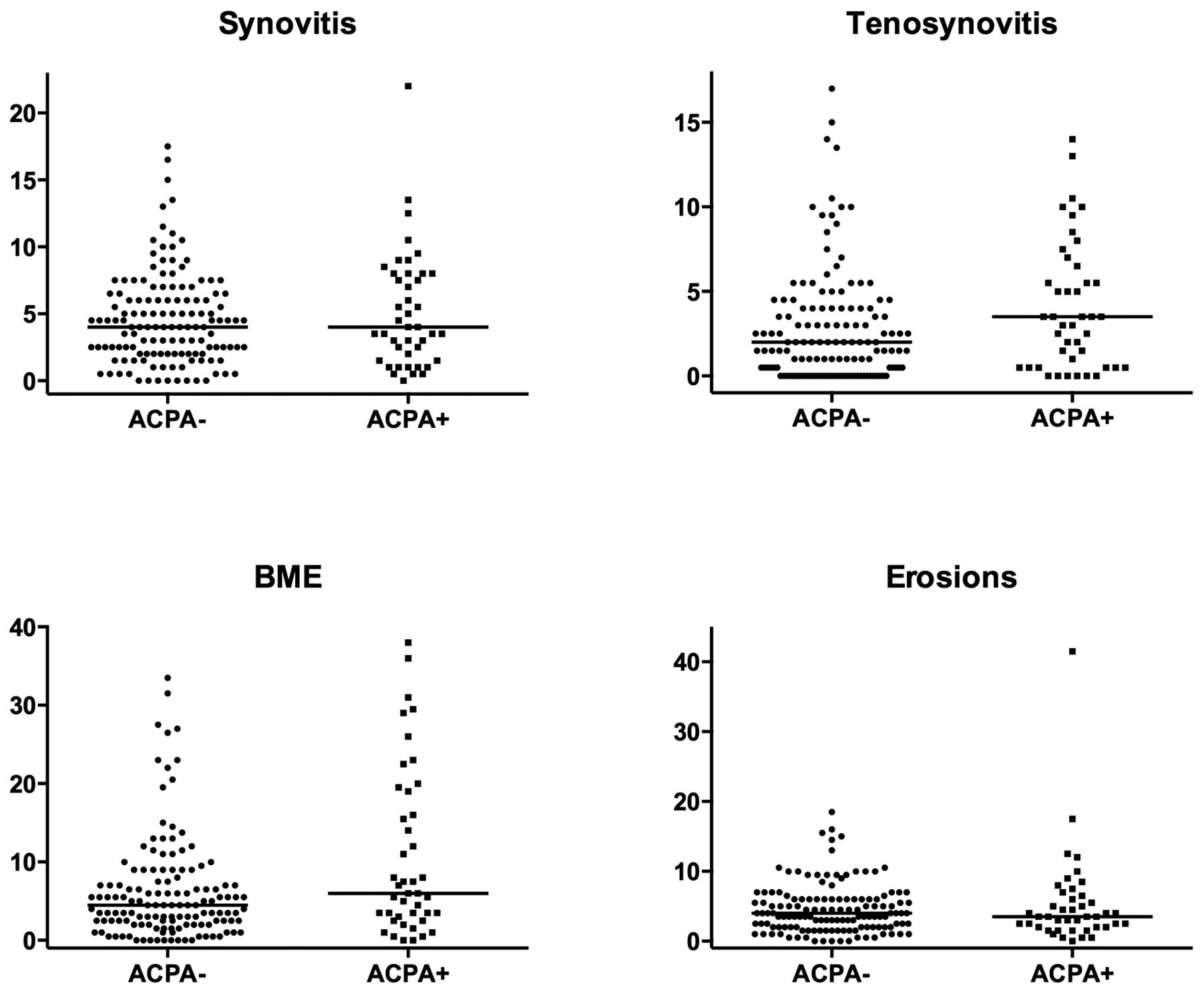
RAMRIS scores for the different MRI features per group of diagnoses for RA and UA patients with and without ACPA (n = 39 and 92, respectively). Horizontal lines represent median values. For tenosynovitis in the ACPA-negative group, many scores are clustered at 0. Synovitis p = 0.57, tenosynovitis p = 0.40, BME p = 0.017, and erosions p = 0.93. RAMRIS: Rheumatoid Arthritis Magnetic Resonance Imaging Scoring; MRI: magnetic resonance imaging; RA: rheumatoid arthritis; UA: undifferentiated arthritis; ACPA: anticitrullinated protein antibodies; BME: bone marrow edema.
Value of hand and foot joints
The RAMRIS is developed for wrists and MCP joints. We also performed MR imaging of the forefoot. When we evaluated the scores of hands and feet separately, it was observed that the scores in the feet were lower (Table 2), but that the distributions of the scores of hands and feet among the different diagnoses were comparable (Appendix 3). When the test characteristics were determined with and without the feet, similar results were obtained (data not shown).
DISCUSSION
Many questions remain to be answered before it can be decided whether 1.5T extremity MRI is valuable for use in clinical practice in the field of RA. One is a basic question: whether the abnormalities seen on MRI are different in patients with RA compared to patients with early arthritis and other diagnoses. Our cross-sectional study set out to explore this, making use of an unselected set of patients with early arthritis. It was observed that among all patients presenting with early arthritis, patients with RA had significantly higher synovitis, BME, and tenosynovitis scores than patients without RA, but also that high synovitis, BME, and tenosynovitis scores were not confined to patients diagnosed with RA. Consequently, the ability of MR imaging to differentiate patients with RA from patients without RA was low.
In our study we did not focus on the subset of patients with UA. The number of patients with UA was relatively low and followup data were not yet available. The definite diagnosis of these patients can be established after 1 or 2 years. Our present study addressed a basic issue by evaluating which differences in MRI features occur between patients with different diagnoses. Although several statistical differences were found, patients with RA did not have striking differences in the severity of MRI inflammatory scores. Further, in the presence of a certain MRI feature, the chance that this patient had RA was low (low positive predictive value). Because the UA group included patients who will go on to develop RA and other diagnoses, results may differ when final diagnoses are used to define groups. Particularly, prospective studies are required to determine whether MRI is valuable for classification of patients whose conditions are clinically undefined. Followup of the studied cohort of patients is currently under way and will be presented in future studies.
Our study has several limitations. The joints scanned are the joint regions that are most commonly involved in RA; also, the RAMRIS method was developed for RA. Patients with other diagnoses may have abnormalities in structures that were not scanned or scored, for instance, inflammation in other joints or capsulitis. When a protocol would be developed for use in practice in patients with RA, the joints as assessed here will likely be included. Adding other small joints, such as interphalangeal joints or other structures, may possibly enhance the discriminative ability. This is a subject for further studies.
One strength of our study was that we scanned metatarsophalangeal (MTP) joints in addition to the more often assessed wrist and MCP joints. This seems relevant because foot involvement is common in early RA and abnormalities may be found even when the hand MR imaging results are normal9,10.
Unfortunately, time constraints prohibited the addition of axial and postcontrast imaging of the foot. However, the contribution of the foot to total scores was generally low. This was not only true for synovitis, for which the lack of gadolinium contrast might have decreased sensitivity, but also for BME and erosions. The MRI features were similarly distributed in hand and foot. Thus findings from this study do not support routine inclusion of MRI of the foot, and hand/wrist MRI is probably adequate; however, studies with a more complete assessment of the MTP joints including postcontrast imaging are necessary for a more definite recommendation.
Although many clinical studies have been performed comparing the 1987 and 2010 criteria for RA, to the best of our knowledge no MRI studies on this subject have been published. We observed no difference in MRI scores between RA when classifying RA according to the 1987 ACR criteria or the 2010 ACR/EULAR criteria. However, a majority of patients overlapped between these 2 groups. When assessing the patients who were positive for both or for 1 of these sets of criteria separately, we did observe that patients with RA fulfilling the 2010 criteria, but not the 1987 criteria, had less synovitis. These baseline MRI data suggest that patients who only fulfill the 2010 criteria have a milder disease; an observation in line with the results of studies comparing the longterm outcome of RA when using the different classification criteria for RA11.
Because it has been suggested that ACPA+ and ACPA– disease are separate entities of RA12, we performed stratified analyses. ACPA-positive patients had significantly more BME than ACPA-negative patients. Because BME is a predictor for progression of joint destruction3, this observation is in line with ACPA-positive RA being a more severe disease. Only 1 earlier study has explored the relation between ACPA and BME, also reporting a significantly higher proportion of patients with BME in the ACPA+ group13. Further, subclinical inflammation including BME has been observed in ACPA-positive patients with arthralgia (although no ACPA-control group was present in that study)14. This observation also relates to the observation that ACPA may be able to directly activate osteoclasts15. Altogether these data support the use of MRI to further increase the understanding of the relation between these 2 risk markers for severe RA, because MRI is the only imaging modality able to show BME.
MRI inflammatory scores were higher in RA than in other diagnoses, and ACPA-positive patients had more BME than ACPA-negative patients. Nonetheless, the severity of MRI inflammation assessed according to RAMRIS does not accurately differentiate patients fitting ACR criteria for RA at 1 timepoint from other patients with early arthritis.
Acknowledgment
We thank Dr. Espen A. Haavardsholm and Dr. Pernille Bøyesen from Diakonhjemmet Hospital in Oslo, Norway, for their help with the OMERACT RAMRIS score.
APPENDIX 1.
RAMRIS scores for the different MRI features for patients with RA according to 1987 and 2010 American College of Rheumatology criteria. Horizontal lines represent median values. RAMRIS: Rheumatoid Arthritis Magnetic Resonance Imaging Scoring; MRI: magnetic resonance imaging; RA: rheumatoid arthritis; BME: bone marrow edema.
APPENDIX 2.

RAMRIS scores for the different MRI features for patients with RA fulfilling both the 1987 and 2010 American College of Rheumatology criteria, and 1 of these 2 sets of criteria. Horizontal lines represent median values. 1987–/2010+ versus 1987+/2010+ patients: synovitis p = 0.029. All other combinations p > 0.05. RAMRIS: Rheumatoid Arthritis Magnetic Resonance Imaging Scoring; MRI: magnetic resonance imaging; RA: rheumatoid arthritis; BME: bone marrow edema.
APPENDIX 3.

RAMRIS scores for the different MRI features per group of diagnoses, separated for hand and foot joints. Box and whisker plots showing median, interquartile, and range of scores separately for the hand (wrist and MCP joints combined, white) and forefoot (grey). Tenosynovitis was only assessed in the hand. MCP: metacarpophalangeal; RAMRIS: Rheumatoid Arthritis Magnetic Resonance Imaging Scoring; MRI: magnetic resonance imaging; BME: bone marrow edema; RA: rheumatoid arthritis; UA: undifferentiated arthritis; OA: osteoarthritis; PsA: psoriatic arthritis.
Footnotes
-
This research was performed within the framework of CTMM, the Center for Translational Molecular Medicine (www.ctmm.nl), and the Dutch Arthritis Foundation, project TRACER (grant 04I-202). The research has also been funded by The European Community Seventh Framework Program FP7 Health-F2-2008-223404 (Masterswitch), as well as by a European grant from the Innovative medicine Initiative: BTCURE. This work of A. van der Helm-van Mil is supported by a Vidi-grant of the Netherlands Organisation for Scientific Research. The work of A. Krabben is supported by a grant of the Dutch Arthritis Foundation.
- Accepted for publication April 3, 2014.








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}