

Abstract
Objective. Treat-to-target guidelines promote shared decision making (SDM) in rheumatoid arthritis (RA). Also, because of high cost and potential toxicity of therapies, SDM is central to patient safety. Our objective was to examine patterns of perceived communication around decision making in 2 cohorts of adults with RA.
Methods. Data were derived from patients enrolled in 1 of 2 longitudinal, observational cohorts [University of California, San Francisco (UCSF) RA Cohort and RA Panel Cohort]. Subjects completed a telephone interview in their preferred language that included a measure of patient-provider communication, including items about decision making. Measures of trust in physician, education, and language proficiency were also asked. Logistic regression was performed to identify correlates of suboptimal SDM communication. Analyses were performed on each sample separately.
Results. Of 509 patients across 2 cohorts, 30% and 32% reported suboptimal SDM communication. Low trust in physician was independently associated with suboptimal SDM communication in both cohorts. Older age and limited English proficiency were independently associated with suboptimal SDM in the UCSF RA Cohort, as was limited health literacy in the RA Panel Cohort.
Conclusion. This study of over 500 adults with RA from 2 demographically distinct cohorts found that nearly one-third of subjects report suboptimal SDM communication with their clinicians, regardless of cohort. Lower trust in physician was independently associated with suboptimal SDM communication in both cohorts, as was limited English language proficiency and older age in the UCSF RA Cohort and limited health literacy in the RA Panel Cohort. These findings underscore the need to examine the influence of SDM on health outcomes in RA.
In a truly shared decision, physicians and patients mutually influence each other, each potentially ending up in a place different from where they began, with different understandings than either would have reached alone.
—J.L. Hanson, Archives of Internal Medicine, July 14, 20081
Rheumatoid arthritis (RA) is the most common inflammatory arthritis, affecting up to 1% of the population. Because of the complexity, high cost, and potential toxicity of therapies for RA, clear patient-clinician communication is central to safety and quality of care. Two of the 6 priorities outlined in the US National Quality Strategy, a provision of the Affordable Care Act, are to ensure patient-centered care and promote effective commun ication2. Implicit in this mandate to provide quality, person-centered care, is the need to involve patients in decision making around all aspects of their care. Further, recommendations from an international task force in rheumatology outline 4 overarching principles in the treatment of RA, the first of which states: “The treatment of rheumatoid arthritis must be based on a shared decision between patient and rheumatologist.”3 Health authorities in several European nations have placed great emphasis on patient engagement in decision making4; however, despite wide recognition of the benefits and ethical considerations in incorporating shared decision making (SDM) and the use of decision aids in everyday practice, a number of barriers to its uptake have been identified. Wennberg and colleagues outlined ways in which the US government could improve care and reduce healthcare spending in their 2008 Dartmouth Atlas White Paper and included a focus on requiring informed patient choice and SDM as ways to reduce unwanted or unnecessary procedures and treatments5. While there is no consensus on a single definition or theoretical framework of what constitutes SDM, we define it here as a process whereby both patient and clinician take into account the best available evidence of risks and benefits across all available options as well as patient values and preferences when making medical decisions6. Evidence that greater levels of informed choice and patient involvement in decision making leads to increased knowledge of conditions and treatment, improved satisfaction with decisions, and greater adherence to medication (as seen in asthma) continues to build in other chronic conditions7,8,9.
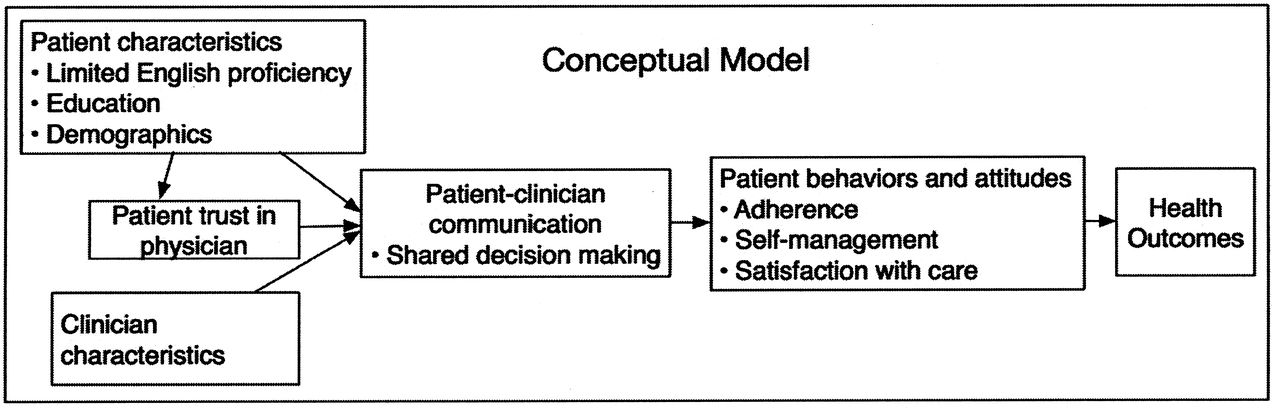
Several factors known to influence patient-provider communication and SDM in other conditions such as diabetes and coronary heart disease include trust in physician, race/ethnicity, education level, employment status, depression, and limited English proficiency (LEP)10,11,12,13,14,15,16. While these factors have been associated with clinician-patient communication in other chronic diseases, they have not been examined in ethnically and linguistically diverse populations with RA, particularly among those patients at highest risk for poor outcomes and with barriers to communication, such as LEP and limited health literacy. Our study model (Figure 1) outlines our vision of the potential relationships between patient-level characteristics, trust in physician, SDM, and how these factors may be related to health outcomes in RA.
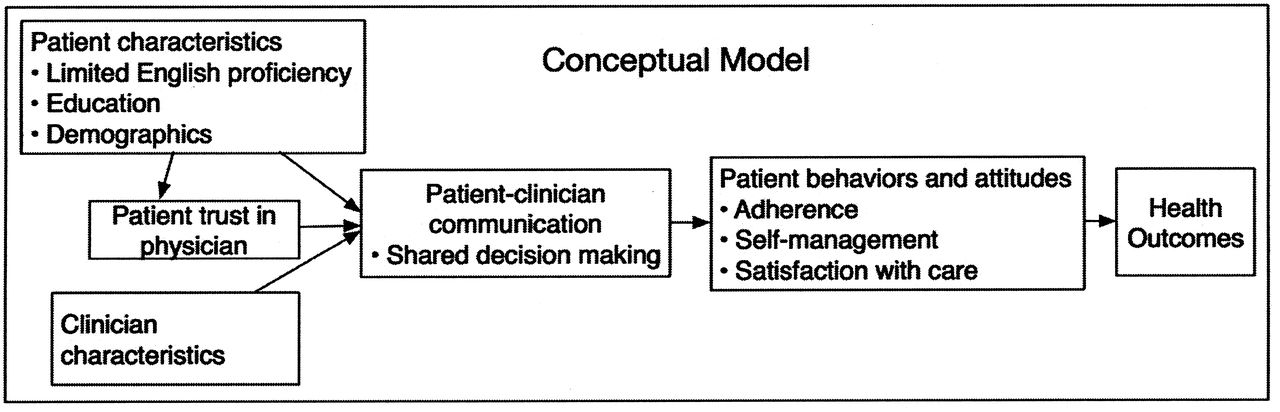
Conceptual model of the relationship among patient-level characteristics, trust, shared decision making, and health outcomes.
We conducted this study to examine patient perception of SDM communication within 2 cohorts of adults with RA. In addition, we sought to better understand the influence of trust, language proficiency, and educational attainment on SDM communication in RA.
MATERIALS AND METHODS
Study design
This is a cross-sectional study of the results from a one-time telephone interview administered to 2 separate cohorts of adults with RA described below.
Data sources
Subjects included in our study were participants in 1 of 2 longitudinal, observational RA cohorts: the RA Panel Study and the University of California, San Francisco (UCSF) RA Cohort. The RA Panel Study was initiated in 1982 by enrolling the universe of persons with RA being treated over a 1-month period by a random sample of Northern California rheumatologists; subsequent enrollment occurred in 1989–1990, 1995–1996, 1999–2000, and 2003–2004, with an average of 85% of listed patients enrolled each time. RA Panel participants are interviewed by telephone annually in English. Followup rates in the RA Panel averaged 92% annually since the last enrollment wave. The data for this study consist of all interviews conducted in 2011, with a total of 275 participants from the RA Panel. The UCSF RA Cohort is a multisite observational cohort whose enrollment began in October 2006. Subjects were consecutively enrolled from 2 outpatient clinics staffed by UCSF faculty and fellows, the Rheumatoid Arthritis Clinic at San Francisco General Hospital and the university-based UCSF Arthritis Center; about 90% of patients agreed to enroll in the cohort. Data for the UCSF RA Cohort were obtained from patients and physicians at the time of each regular clinical visit and integrated with laboratory and radiology test results. The 234 patients from the UCSF RA Cohort included in this study were interviewed by telephone between 2007 and 2009 in their preferred language (English, Spanish, or Cantonese); they represented 85% of all active cohort members at that time. The research protocol for both cohorts was approved by the UCSF Committee on Human Research. All participants gave their informed consent to be part of the study. This study took place in the UCSF Collaborative Research Network.
Primary outcome: quality of SDM communication
To measure the patient perception of communication around SDM, we used a subscale from the Interpersonal Processes of Care (IPC) survey. The IPC is a valid and reliable measure17 designed to quantify specific components of doctor-patient communication in diverse populations18; it was included in the telephone survey for both cohorts. Prior to administration of the IPC, all patients are told: “The next questions are about your experiences talking with your main rheumatology or arthritis doctor over the past twelve months … ” If the patient reports seeing more than 1 physician, they are then prompted to answer about the doctor seen most often. The primary outcome for this study was the 2-item validated decision-making subscale of the IPC that is calculated as the mean score for 2 items, “How often did you and your doctors work out a treatment plan together?” and, “If there were treatment choices, how often did doctors ask if you would like to help decide your treatment?” The 5-item response ranged from 1 (“never”) to 5 (“always”). We created a summary score from the average of the 2 items. Mean scores < 4 (corresponding to never/rarely/sometimes) were categorized as suboptimal communication, as has been done in prior studies15. We also created an alternate measure of communication in decision making, in which anything besides the highest rating on both measures was considered suboptimal, as has been done in other surveys of healthcare experiences (Consumer Assessments of Healthcare Providers and Systems) and considered the “top box” approach19 to scoring, which has also been recommended for the IPC20.
Trust in physician
Among primary independent variables, trust in physician has been shown to be associated with quality of communication14,15 as well as confidence in the decision to take a disease-modifying antirheumatic drug (DMARD) in RA21. We measured trust with the 11-item Trust in Physician scale22, which has been validated in patients with RA23; however, to our knowledge, it has not been validated in Spanish (David Thom, personal correspondence). Each question has a 5-point Likert scale response ranging from 1 (“strongly disagree”) to 5 (“strongly agree”). Examples of questions include “I trust my doctor so much I always try to follow his/her advice,” “I trust my doctor’s judgments about my medical care,” and “I trust my doctor to tell me if a mistake was made about my treatment.” Responses are summed and the value obtained is transformed to a 0–100 scale. A score below the median (90.9) was considered to be suboptimal.
Education and income
Education level was ascertained during the telephone interview and dichotomized as less than high school (< HS) or high school graduate and beyond. Household income was also gathered in the telephone interview and included here as an alternate measure of socioeconomic status (SES), categorized as < $20,000, $20,000–$80,000, and > $80,000 US.
Limited English language proficiency
In UCSF RA Cohort interviews, English language proficiency was assessed using the US Census question “How well do you speak English?” Those who reported “very well” or “well” were considered English proficient (EP) and those who reported “not well” or “not at all” were considered to have LEP13,24,25. English language proficiency was not ascertained in the RA Panel, which was conducted exclusively in English.
Health literacy
Health literacy was measured in the RA Panel using the single-item literacy screener, a self-report question developed by Morris and colleagues26,27 validated among diverse English and Spanish-speaking populations28 and administered over the telephone in multiple prior studies29,30,31. This screener has also been used to measure health literacy in a large study of over 6000 patients with RA in the United States32. The single-item question is “How often do you have someone like a family member, friend, hospital or clinic worker or caregiver help you read health plan materials, such as written information about your health or care you are offered?” Possible answers include “always, often, sometimes, occasionally or never.” A response of “sometimes,” “often,” or “always” was considered to represent limited health literacy27,33.
Other variables
Patient age, sex, race/ethnicity, language, and date of diagnosis were obtained at time of enrollment into the cohorts. Patients provided a global assessment of their disease during the telephone interview, answering the following question, “Considering all the ways that your arthritis affects you, rate how well you are doing on a scale from 0 to 100, where 0 is very well and 100 is very poor”34. The Patient Health Questionnaire-9 (PHQ-9)35,36 was collected in the UCSF RA Cohort, and the Geriatric Depression Scale short form (GDS)37,38 was obtained in the RA Panel to measure depressive symptoms. The RA Panel has used the GDS consistently since 1989; the UCSF RA Cohort has used the PHQ-9 since 2006 because it has been validated in multiple languages36,39,40,41 and used among patients with limited literacy42 and English language proficiency43. We used cutoffs for depressive symptoms in each scale that allowed for comparable thresholds.
Statistical analysis
We conducted all analyses on the 2 cohorts separately, examining the associations between the likelihood of reporting suboptimal communication in SDM and the primary independent variables of education, health literacy, or English language proficiency, and trust in physician. Because the dependent variable is dichotomous, we used binary logistic regression for all statistical modeling. In addition to the primary independent variables, we selected covariates on an a priori basis that are known or hypothesized to be associated with differences in patient-provider communication. These included patient age, sex, race/ethnicity, disease duration, and patient global disease assessment. Because of the relatively low number of RA Panel members who were ethnic minorities, whites were compared to nonwhites in that cohort.
We initially examined the relationship between each independent variable and the likelihood of suboptimal communication in SDM in a series of bivariable logistic regression models. We next assessed the full model for multicollinearity. Finding no covariates with variance inflation factors above 1.5 in either cohort, we determined that all variables could be appropriately included in the same multivariable models; there was like-wise no evidence of excessive influence by any individual observations in the models. The models showed an adequate fit to the data based on both the classification table approach (> 70% correctly classified in each model), and the Hosmer-Lemeshow goodness-of-fit test44. Last, we assessed potential interactions among the primary independent variables: trust, education, and health literacy (in the RA Panel) or English language proficiency (in the UCSF RA Cohort). Finding no significant interactions in either model, we present only the main effects models.
We examined several alternate models to the ones presented here. These included replacing education with household income as an alternate measure of SES, and adding a measure of depressive symptomatology, which has been associated with suboptimal communication in coronary heart disease and diabetes14,15, to the multivariable model for each cohort. We investigated the role of trust in physician as either an effect modifier or a mediator in the relationship of each of the main predictor variables to SDM. As a sensitivity analysis, we used the more inclusive measure of suboptimal communication as the dependent variable in the logistic regression models.
All analyses were performed using STATA Version 12 (STATA Corp.).
RESULTS
A total of 509 subjects were included in our study, 234 from the UCSF RA Cohort and 275 from the RA Panel. Patients from both cohorts were predominantly female (84% in the UCSF Cohort, 86% in the RA Panel); however, they were different in all other demographic characteristics (Table 1). The UCSF RA Cohort has great diversity by race/ethnicity and language, with substantial numbers of ethnic minorities and non-English speakers (64% English, 22% Spanish, and 14% Cantonese or Mandarin). The average age of the RA Panel patients was nearly 10 years older; 83% were white, and 95% had graduated high school. Limited health literacy was identified in 39 subjects (14%) in the RA Panel. RA Panel participants rated their disease as less active overall, with a mean rating of 24.2 versus 41.9 for the UCSF RA Cohort patients, on a 0–100 scale. The 2 cohorts assessed depressive symptoms using 2 different measures and had differing degrees of depressive symptoms as well. In the UCSF RA Cohort, 25% of subjects had a PHQ-9 score ≥ 10, which has been shown to correspond to moderate depressive symptoms or greater. In the RA Panel, only 13% had a comparably high score in the GDS. Patients in both cohorts expressed a high degree of trust in their physicians, with half giving a score of over 90 on a 0–100 scale.
Characteristics of participants from 2 rheumatoid arthritis (RA) cohorts. Values are n (%) or mean ± SD.
Primary outcome
Despite the demographic differences, patients were nearly equally likely to report suboptimal SDM communication (30% for the Cohort and 32% for the Panel, Table 2).
Proportion of study participants in 2 cohorts reporting suboptimal communication in shared decision making (SDM).
UCSF RA cohort
In bivariate analyses, sex, age, and disease duration were not associated with suboptimal communication. Latino and Asian/Pacific Islander race/ethnicity, LEP, less than high school education, and low trust in physician were all associated with greater risk of reporting suboptimal SDM communication (Table 3). In the multivariate analyses, lower trust in physician remained strongly associated with suboptimal SDM communication with an adjusted OR (AOR) of 2.11 (95% CI 1.10–4.07). In addition, an increase in age was a significant independent correlate of suboptimal SDM (AOR 1.28 per 10 years, 95% CI 1.01–1.62), as was LEP (AOR 5.11, 95% CI 1.56–16.7). Race/ethnicity and education were no longer significant in the multivariable model.
OR for suboptimal communication in shared decision making among 234 UCSF RA Cohort participants, from unadjusted and adjusted logistic regression models.
RA panel
In bivariate analyses, the Panel showed similar results with respect to low trust in physician (OR 5.22, 95% CI 2.93–9.31), but lower education, race/ethnicity, age, sex, and disease duration were not associated with suboptimal SDM communication. However, worse patient global rating of disease was associated with suboptimal SDM communication (Table 4). In multivariate analysis, low trust in physician remained significant (AOR 5.57, 95% CI 3.05–10.15) as did limited health literacy (AOR 2.80, 95% CI 1.25–6.28).
OR for suboptimal communication in shared decision making among 275 RA Panel participants, from unadjusted and adjusted logistic regression models.
We conducted several sensitivity analyses as part of the study. Given the use of a “top box” method of scoring healthcare experience surveys as discussed above, we created a more stringent definition of optimal communication, only including participants who responded “always” to both decision-making items. Under this definition, more than 50% of either cohort report suboptimal communication around decision making. Nevertheless, the results for the main analysis are essentially unchanged, with strong associations with LEP and suboptimal trust in physician in the UCSF RA Cohort and with health literacy and suboptimal trust in the RA Panel. When we estimated the models using annual household income as an alternate measure of SES, the findings were similarly unchanged. Depressive symptoms have been shown to be associated with suboptimal patient-clinician communication in other chronic diseases such as diabetes and coronary heart disease. Measures of depressive symptoms were available on a subset of patients in both cohorts. We recalculated the multivariate models for both cohorts separately and included the measures of depressive symptoms. Depressive symptoms were not associated with suboptimal communication in either multivariate model, nor did the inclusion of depressive symptoms change the main results. Because we anticipated that trust in physician could modify the association of the primary independent variables with SDM communication, we added interaction terms to the models for both cohorts, but found no significant effect modification. Similarly, trust could play a mediating role in the pathway between these variables and SDM. However, there was no evidence of mediation in either cohort.
DISCUSSION
This study of 2 demographically distinct cohorts including a total of over 500 adults with RA found that nearly one-third of subjects reported suboptimal SDM communication with their clinicians, regardless of the study sample. To our knowledge, this is the first study of perceptions of SDM communication in RA that has included a diverse, multi-lingual population.
Strikingly, low trust in physician was independently associated with suboptimal SDM communication in both cohorts. In addition, LEP was associated with greater likelihood of reporting suboptimal communication, after controlling for age, sex, race/ethnicity, disease duration, and trust in physician in the more diverse UCSF RA Cohort for language and race/ethnicity. Limited health literacy was also an independent correlate of suboptimal communication in the largely white, more educated, older subjects in the RA Panel. While older age and suboptimal trust in physician have been associated with poorer communication in prior studies of patients with RA21,45, LEP and limited health literacy have not been studied as a correlate of SDM in RA.
The emphasis on SDM as an integral part of delivering high-quality, patient-centered care is reflected in national and international directives such as the Institute of Medicine’s Crossing the Quality Chasm, which concerns all medical conditions, and the 2010 Treat to Target guidelines for RA, which concerns this one. Despite the goal of an informed, engaged patient truly sharing a decision with the clinician, multiple barriers to this ideal exist4. Specific barriers include health beliefs, and educational, cultural, or literacy backgrounds that pose challenges to understanding or applying existing evidence to certain decisions, such as whether to begin a biologic or triple therapy with synthetic DMARD when faced with moderate to high disease activity. Such barriers can then result in disenfranchisement, or may further alienate patients from fully engaging in healthcare decisions46.
As evidenced by our current study, patients with limited health literacy and LEP had much greater risk of suboptimal SDM communication. It is these very populations who are also at increased risk of poorer health outcomes in RA, even if they have access to the most current, state-of-the-art treatments47. In a cross-sectional study of over 1000 commun -ity-based patients with RA (6.5% non-white and 8.8% with limited health literacy), Martin and colleagues found that health literacy was independently associated with risk perception and willingness to take a DMARD but that depression was not48. This study also found that risk perception mediates the effect of health literacy on willingness to take a DMARD. This finding underscores the importance of creating interventions to ensure that more vulnerable groups are truly informed of risks and benefits of treatments and are engaged in making treatment decisions with their clinicians. In other chronic diseases, suboptimal patient-clinician communication has been associated with lower medication adherence to cardiometabolic medications in heart disease, and to hypoglycemic medications in diabetes12, which suggests a possible role for communication in addressing health disparities in general49. While associations with poorer adherence or health outcomes have not yet been demonstrated in RA, it is a reasonable next step in acquiring a better understanding of whether a link exists between patient-provider communication and health disparities.
Prior studies have reported on decision making in RA, but have largely examined the concept in majority populations with higher levels of education. Kjeken, et al studied over 1000 Norwegian patients with RA and found that younger age, high levels of formal education, high levels of satisfaction with care, and received information were all associated with greater patient involvement in medical decisions45. In a study of 628 US adults with RA who were 90% white and over half of whom had some college education or more, Martin, et al identified trust as an independent correlate of confidence in a medical decision21. While our study confirms the findings of prior work, it adds substantially to the current literature in that it included populations most vulnerable to poor outcomes and suboptimal communication. While it is perhaps not surprising that those with limited health literacy and LEP reported suboptimal communication around SDM, the size of the effect of these barriers was notable, at minimum in the case of health literacy, tripling the odds of reporting suboptimal communication. These findings emphasize and underscore the need to identify these characteristics of our patients, and promote and support patient-centered care in these groups.
Our study has several limitations. The cross-sectional design does not allow inferences regarding causation, particularly with regard to the relationship between trust and SDM, even though our theoretical model proposes a causal pathway. Patient reports of communication may be subject to recall bias12, and such bias may be greater among those with low trust or poor understanding of the healthcare encounter. The measure of decision-making communication used was one of self-report and not one of direct observation, however the IPC subscale of decision making has been developed and validated in diverse populations and administered to similar patient populations to those in our study15,17,18,50. Our measure of health literacy in the RA Panel is self-reported and does not capture all domains of this complex concept, nor does it measure numeracy; use of the single item screener that focuses on reading ability may lead to measurement bias when compared to a longer instrument of health literacy. We did not have a measure of health literacy in the UCSF RA Cohort, which one might assume would have an even greater number of subjects with limited literacy. We combined race/ethnicity into a single category for matters of simplicity and power; however, we acknowledge that an analysis examining the association of ethnicity (Latino vs non-Latino) with communication around decision making may be of interest in future studies to evaluate whether English-speaking Hispanics’ experiences differ from English-speaking non-Hispanics.
What can be done to improve the quality of communication and to promote SDM in rheumatology care? It has been reported that physicians engage less in SDM than they perceive51. Clinicians often report they do not have time for engaging in SDM and believe that patients want to be told what to do or have their doctors decide what is best1. However, despite reservations on the part of clinicians, there is evidence to support the practice of patient-centered care and SDM as well as the use of decision aids to improve communication and enhance health outcomes. A 2011 Cochrane review of 86 decision aids reported that these tools appear to have a positive effect on patient-clinician communication, increase patient involvement, and improve knowledge and realistic perception of outcomes52. The effects on adherence, cost effectiveness, and use with lower literacy populations were deemed to require further evaluation. To date, several investigators have published studies on the development and testing of decision support tools designed for patients with RA53,54,55, but only 1 addressed the needs of patients with low literacy54, and none addressed the barriers of LEP. Given the findings of our study and what is known about disparities in RA, we could begin by enhancing the provision of literacy-appropriate educational resources that describe the condition, therapies, risks/benefits, and potential harms to all patients with RA; training clinicians who care for patients with RA in communication skills and techniques of delivering patient-centered care56; increasing awareness of SDM and the use of decision support tools; and promoting the development and implementation of low literacy decision aids to facilitate SDM around complex therapies. In addition to targeting clinician and patient-level enhancements in communication, Brach and colleagues in a 2012 article published by the Institute of Medicine outline 10 attributes of a “health literate organization.” The authors underscore that the provision of truly health literate care to patients is “a necessary prerequisite to assuring patient safety, promoting adherence, enhancing self-efficacy, and improving patient outcomes”57.
Future research must investigate patient-clinician communication as a potential contributor to health disparities, particularly in the rheumatic diseases. If we as a subspecialty are to have any influence on the persistent health disparities documented among our patients, we need to closely examine all facets of care. If patients lack trust or feel their doctors do not respect them or involve them in making decisions about their health, patients may in turn be less likely to adhere to therapy and be at higher risk of poorer outcomes. A disenfranchised patient then enters a vicious cycle of disempowerment and disenchantment with medical care. It is the responsibility of the medical community to confront deficiencies and variation in care resulting from the healthcare system, even those occurring in the interaction in the examination room.
Implications
Our study highlights that nearly one-third of adults with RA report suboptimal SDM communication with their clinician. Patients with limited health literacy, LEP, and lower trust in physician had significantly greater odds of suboptimal SDM communication. These findings underscore the need for more research into the association of SDM and health outcomes, and potentially, the development of more literacy- and language-appropriate interventions.
Footnotes
-
Drs. Barton, Imboden, Katz, and Yelin’s work was supported by funding from the Rosalind Russell Medical Research Center for Arthritis, University of California, San Francisco. Drs. Barton, Imboden, and Yelin received funding from the Agency for Healthcare Research and Quality (R18 HS19209). Drs. Barton, Yelin, and Katz, and Ms. Trupin’s work was also supported by US National Institute of Arthritis and Musculoskeletal and Skin Diseases (grant P60 AR053308, Multidisciplinary Clinical Research Center). Dr. Schillinger’s work was supported by the US National Institutes of Health (NIH)/National Center for Research Resources UCSF–Clinical and Translational Science Institute Grant Number UL1 RR024131. This publication’s contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH.
- Accepted for publication March 26, 2014.








{kind=link}