

Abstract
Objective. To assess ovarian reserve markers in patients with Takayasu arteritis (TA).
Methods. Twenty patients with TA and 24 healthy controls were evaluated for ovarian reserve by follicle-stimulating hormone, luteinizing hormone, and estradiol, and antral follicle count (AFC). Anti-Müllerian hormone (AMH) was measured by ELISA using 2 different kits. Demographical data, menstrual abnormalities, disease variables, and treatment were also analyzed.
Results. The median current age was similar in patients with TA and controls (31.2 ± 6.1 vs 30.4 ± 6.9 yrs, p = 0.69). The frequencies of decreased levels of AMH in patients with TA were identical using both kits and higher when compared to controls (50% vs 17%, p = 0.02; 50% vs 19%, p = 0.048). A positive correlation was observed between the 2 kits in patients with TA (r = +0.93, p < 0.0001) and in healthy controls (r = +0.93, p < 0.0001). The apparent lower AFC (11 vs 16, p = 0.13) and the higher frequency of low AFC (41% vs 22%, p = 0.29) in TA compared to controls did not reach statistical significance. Other hormones were similar in both groups (p > 0.05). Further evaluation of patients with TA with low AMH levels (< 1.0 ng/ml) versus normal AMH levels (> 1.0 ng/ml) revealed that the frequency of current disease activity (p = 1.0) and the median of erythrocyte sedimentation rate (p = 0.6), C-reactive protein (p = 0.4), prednisone cumulative dose (p = 0.8), and methotrexate cumulative dose (p = 0.8) were comparable in both groups. Cyclophosphamide use was reported in only 1 patient with reduced ovarian reserve, whereas none of the remaining patients received gonadotoxic drugs.
Conclusion. To the best of our knowledge, our present study was the first to suggest that patients with TA may have diminished ovarian reserve.
Takayasu arteritis (TA) is a rare idiopathic systemic chronic vasculitis that involves large arteries1,2. This disease occurs mainly in women of reproductive age, when ovarian reserve and future fertility are major topics of interest.
Aging, surgery, and hypothalamic-pituitary-gonad axis dysfunction have been found to influence the quantity and quality of primordial follicles in ovaries and ultimately, the ovarian reserve3,4,5.
Other conditions such as autoimmune oophoritis5 and immunosuppressive drugs, particularly intravenous cyclophosphamide (IVCYC), may also result in diminished ovarian reserve6,7,8,9,10,11. Women with TA are susceptible to these factors, but there is no systematic study assessing this ovary abnormality in these patients.
Therefore, we have performed a complete assessment of ovarian reserve, including hormonal profile and ovarian ultrasound in patients with TA and healthy controls. The possible association between reduction of ovarian reserve and disease variables and treatment were also analyzed.
MATERIALS AND METHODS
Patients and controls
We have screened 52 consecutive women with TA, followed at the Vasculitis Outpatient Clinic of the Rheumatology Division of Clinics Hospital, University of São Paulo, São Paulo, Brazil, from July 2011 to December 2012. All patients were between the ages of 18 and 45 years and fulfilled the American College of Rheumatology classification criteria12.
Exclusion criteria were current pregnancy, hypothalamus-pituitary-gonadal axis dysfunction, use of hormonal contraceptive in the last 6 months, gynecological surgery, gynecological cancer, presence of an additional autoimmune disease, did not agree to participate in our study, and incomplete gonadal evaluation. Thirty-two were excluded: use of hormonal contraceptive (n = 15), did not agree to participate (n = 7), incomplete assessment (n = 4), presence of granulomatosis with polyangiitis (n = 2), current pregnancy (n = 2), hyperprolactinemia (n = 1), and current treatment for gynecological cancer (n = 1). Therefore, a cross-sectional study was conducted in 20 patients with TA and 24 healthy controls according to the same exclusion criteria. The Local Ethics Committee of our University Hospital approved our study and an informed consent was obtained from all participants. The Brazilian socio-economic classes were classified according to the Associação Brasileira dos Institutos de Pesquisa de Mercados13.
Age at menarche, and time between menarche and current age, were evaluated. Obstetric data were recorded based on individual’s recollection. Amenorrhea was defined as absence of menstrual period for at least 3 consecutive cycles. Normal cycle was defined as flow duration varying 3–7 days and length 25–35 days7,9. Menstrual disturbances were based on alterations in 1 or more of these variables during evaluation. Patients with amenorrhea (> 1 yr) in whom menstruation did not resume and had follicle-stimulating hormone (FSH) levels > 40 IU/l were defined as premature ovarian failure (POF). Secondary sexual characteristics were classified according to Tanner pubertal changes14.
Ovarian reserve tests
Complete ovarian function was assessed by evaluation of serum hormones levels on the early follicular phase of the menstrual cycle or randomly for those with defined amenorrhea, blinded to the other variables of ovarian function. FSH (reference levels 3.5–12.5 IU/l), luteinizing hormone (LH; 2.4–12.6 IU/l), and estradiol (≤ 166 pg/ml) were measured by radioimmunoassay using a commercial kit (Cobas, Roche). Intraassay and interassay coefficients of variation were recommended by the manufacturer and were limited to 5.7% and 3.6%, respectively. FSH were considered elevated when levels were ≥ 10 IU/l.
Anti-Müllerian hormone (AMH) was measured by ELISA (AMH Gen II ELISA, Beckman Coulter Inc.) in duplicated samples in 20 patients with TA and 24 controls. Intraassay and interassay coefficients of variation were limited to 5.4% and 5.6%, respectively. AMH was also evaluated by ultrasensitive AMH/Müllerian inhibiting substance enzyme linked chemiluminescent immunoassay (US AMH/MIS AnshLabs ELISA) in duplicated samples in 20 patients with TA and 22 controls. Intraassay and interassay coefficients of variation were limited to 3.1% and 2.7%, respectively. AMH level < 1.0 ng/ml was considered as reduced according to manufacturer suggestion15,16.
Transvaginal ultrasound was performed in all sexually active patients with TA and controls by an expert sonographer (LYSY) using a 6.5 MHz endovaginal transducer (HD3, Philips Ultrasound) and blinded to the other variables of gonadal function at study entry. Ovaries were scanned in axial and longitudinal planes, and at least 2 measurements of length (L), width (W), and thickness (T) were obtained and used to calculate the mean ovarian volumes (L × W × T ×π/6)17. Follicles of 2 mm to 10 mm were counted in the antral follicle count (AFC)18. AFC levels were divided into clinically suitable classifications: ≤ 10 (low) and < 5 follicles (very low).
Clinical, laboratory evaluation, and treatment of patients with TA
The following clinical manifestations were assessed: arterial hypertension (HTN), stroke, myocardial infarction, aortic insufficiency, and heart failure. Vascular imaging studies of each patient were evaluated according to the angiographic classification of the International TA Conference in Tokyo 1994 in 6 different types as follows: Type I (the aortic branches are involved), Type IIa (the ascending aorta, arch, and its branches), Type IIb (the ascending aorta, arch with its branches, and thoracic descending aorta), Type III (the thoracic descending aorta, abdominal aorta, and/or renal arteries), Type IV (only the abdominal aorta and/or renal arteries), and Type V (the combined features of Type IIb and IV)19. The patterns of vascular involvement consisted of occlusion (total occlusion of the lumen), stenosis (narrowing of the lumen), and aneurysm.
Current disease activity was defined based on National Institutes of Health criteria or modified Kerr’s criteria20. Erythrocyte sedimentation rate (ESR) was performed according to the Westergren method and C-reactive protein (CRP) according to nephelometry. Data concerning the cumulative and current dosage of all medications were determined.
Statistical analysis
Results were presented as the mean ± SD or median (range) for continuous, and percentage for categorical variables. Data were compared by t test and Mann–Whitney test in TA and controls. Categorical variables were assessed by Fisher’s exact test. Spearman rank correlation coefficient was used for correlations between cumulative dose of immunosuppressive drugs and ovarian reserve variables, and between AMH Gen II ELISA and US AMH/MIS AnshLabs ELISA kits in patients with TA and healthy controls. The level of significance was set at 5% (p < 0.05).
RESULTS
Patients with TA and healthy controls
All of the patients with TA and controls were postpubertal (Tanner stage 5). The mean of current age was similar in TA and controls (31.2 ± 6.1 vs 30.4 ± 6.9 yrs, p = 0.69), as well as the body mass index, and the frequencies of white race and socio-economic class (p > 0.05). The frequency of arterial HTN was significantly higher in patients with TA compared to controls (55% vs 4%, p = 0.0003). No differences were evidenced in menstrual cycle and obstetric data in either group (p > 0.05; Table 1). None of the nulliparous patients with TA and controls tried to get pregnant and failed to conceive. The number of live births and abortions were similar in TA and controls (p = 0.28, p = 0.34; Table 1) and there was no case of stillbirth.
Demographic and clinical features, menstrual cycles, obstetric data, and ovarian reserve in patients with TA and healthy controls. Values are expressed in n (%), mean ± SD, or median (range). Gynecologic age is time between menarche and current age.
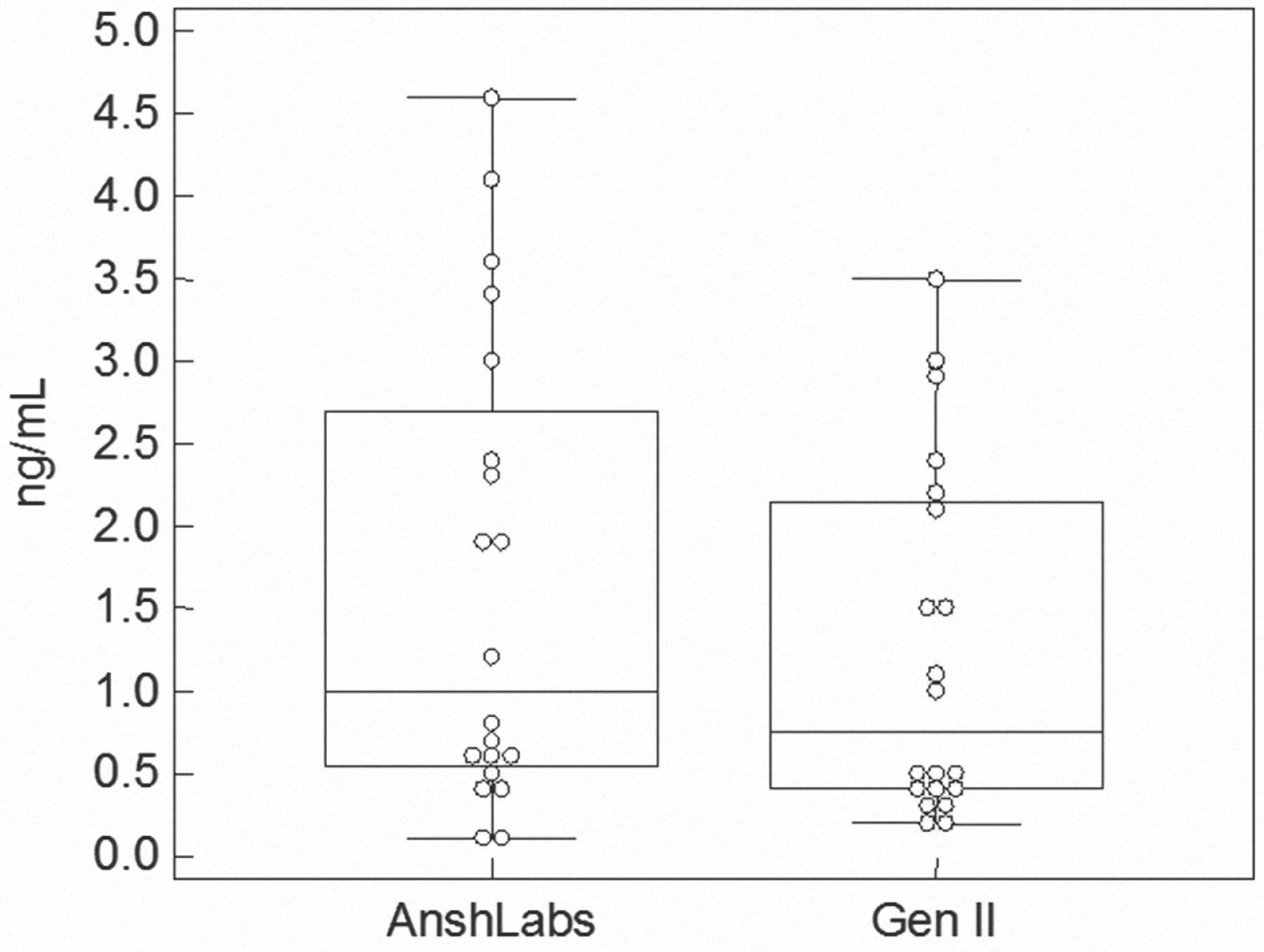
A positive correlation was observed between AMH Gen II ELISA assay and US AMH/MIS AnshLabs ELISA assay in patients with TA (r = +0.93, p < 0.0001) and in healthy controls (r = +0.93, p < 0.0001). The same 10 patients with TA and 4 healthy controls had decreased AMH (< 1.0 ng/ml) in both kits. Frequencies of decreased levels of AMH were significantly increased in TA according to AMH Gen II ELISA kits (50% vs 17%, p = 0.02) and US AMH/MIS AnshLabs ELISA (50% vs 19%, p = 0.048). The median of AMH (Gen II ELISA) was significantly reduced in 20 patients with TA versus 24 controls [0.7 (0.2–3.5) ng/ml vs 2.7 (0.1–6.6) ng/ml, p = 0.008] whereas the lower median of AMH (US AMH/MIS AnshLabs ELISA) in 20 patients with TA compared to 22 controls did not reach statistical significance [1.0 (0.1–4.6) ng/ml vs 2.3 (0–6.6) ng/ml, p = 0.12; Table 1]. Figure 1 includes data plot for AMH using 2 different ELISA assays.
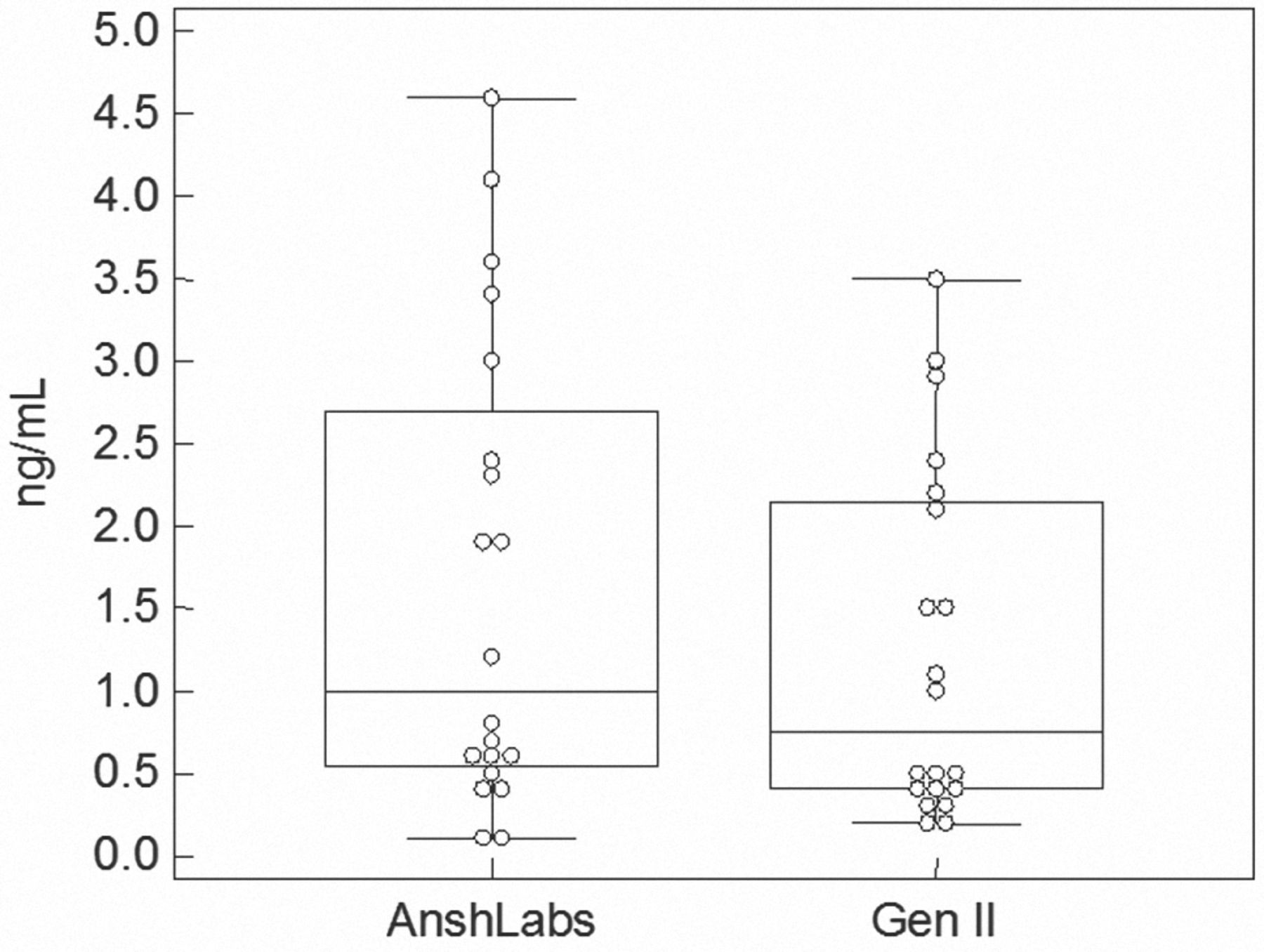
Data plot for anti-Müllerian hormone using 2 different ELISA assays.
The apparent lower AFC [11 (3–40) vs 16 (5–37), p = 0.13] and the higher frequency of low AFC (41% vs 22%, p = 0.29) in TA compared to controls also did not reach statistical significance. Ovarian volume and levels of FSH, LH, and estradiol were alike in both groups (p > 0.05; Table 1).
Ovarian reserve in patients with TA
Further evaluation of patients with TA with low AMH levels versus normal AMH levels revealed no differences in the age at TA diagnosis (24.7 ± 7.4 yrs vs 21.3 ± 6.5 yrs, p = 0.29), time lag between TA diagnosis and AMH assessment (9.7 ± 7.0 yrs vs 6.8 ± 5.0 yrs, p = 0.31), and current disease activity (20% vs 20%, p = 1.0). Only one 38-year-old patient with TA had concomitant low AMH and high FSH levels, whereas all others with low AMH levels had FSH within normal levels.
Arterial HTN was observed in 55% of patients with TA, stroke in 25%, aortic insufficiency in 10%, myocardial infarction in 5%, and none of them had heart failure. Angiographic Type V was evidenced in 11 (55%), Type I in 4 (20%), Type IV in 2 (10%), and Types IIa, IIb, and III in 1 patient with TA each. Occlusion and/or stenosis were observed in 100% of patients with TA and aneurysm in 20% of them.
The median of ESR [16 (7–19) mm/first h vs 18.5 (5–51) mm/first h, p = 0.6], CRP (5.6 ± 3.4 mg/l vs 7.5 ± 6.7 mg/l, p = 0.4), prednisone cumulative dose [4 g (0–41.1) vs 9.2 g (0–27.3), p = 0.8), and methotrexate (MTX) cumulative dose (2.6 ± 2.7 g vs 2.3 ± 1.4 g, p = 0.8) were comparable in patients with low AMH levels versus normal AMH levels. Cyclophosphamide use was reported in only 1 patient with reduced ovarian reserve, whereas none of the remaining patients received gonadotoxic drugs. No correlations were observed between cumulative doses of prednisone and MTX with AMH levels and AFC (p > 0.05). Treatment durations for immunosuppressive drugs in patients with TA were prednisone, 2.5 years (0.6–8.2); MTX, 2.5 years (0.1–6.0); azathioprine, 1.8 years (1.2–4.5); and mycophenolate mofetil, 1.5 years (0.7–6.1).
DISCUSSION
To our knowledge, ours was the first study to identify that patients with TA may have a shortened reproductive lifespan.
The main advantage of our study was a complete ovarian reserve assessment in postpubertal patients with TA and controls at an early follicular phase of menstrual cycle that provided a more accurate estimation of follicle population3,4. The rigorous selection criteria of our patients and controls younger than 45 years21 and without recent gynecologic surgeries, pregnancy, and hypothalamic-ovary and pituitary-ovary axis dysfunction are relevant because these alterations may influence ovarian reserve tests4,10.
In addition, we evaluated hormonal profile without the effect of any exogenous hormone for at least 6 months to avoid possible bias, because another study indicated that AMH levels can be decreased in women using contraceptives22. These restrictive inclusion and exclusion criteria resulted, however, in a small sample size.
Our careful evaluation suggested that patients with TA have lower AMH levels compared to controls. The use of 2 different kits with similar results regarding the frequency of reduced AMH ruled out the possibility of instability in terms of values of AMH Gen II ELISA recently reported23. Moreover, our data showed a very strong correlation between both assay assessments. Of note, AMH levels were more often decreased in patients with TA with a low but not significant AFC. The smaller number of subjects that performed transvaginal ultrasound evaluation is the most likely explanation for this nonsignificant finding. The clinical utility of AFC is limited because it has low sensitivity, in spite of high specificity24.
Ovarian reserve in autoimmune rheumatic diseases may be influenced by age, autoimmunity, and therapy3,4,10. The comparable ages among patients and controls exclude this confounding variable and reinforce the finding of a premature reduced ovarian reserve in patients with TA21.
Diminished follicle ovarian pool was probably not related to TA therapy. Patients with TA were different from women with systemic lupus erythematosus and patients with dermatomyositis3,4,10,11 in whom immunosuppressive agents, particularly IVCYC, and glucocorticoids influenced the menstrual cycles and ovarian reserve. Additionally, disease activity was reported to contribute to alter reproductive function in adult and adolescent SLE8, contrasting to the lack of association observed herein.
The future reproductive health of patients with TA is unknown and family planning must be discussed with all patients, especially young patients with low ovarian reserve. In this regard, a recent study showed that healthy women over age 40 with extremely low levels of AMH still had a chance of pregnancy25.
To the best of our knowledge, our present report was the first to suggest that patients with TA may have diminished ovarian reserve.
Acknowledgment
We thank Elaine P. Leon for technical support and Dr. Ulysses Doria Filho for statistical analysis.
Footnotes
-
Supported by grants from Fundação de Amparo à Pesquisa do Estado de São Paulo (FAPESP# 11/12471-2 to CAS), Conselho Nacional de Desenvolvimento Científico e Tecnológico (CNPQ #300559/2009-7 to RMRP, #301411/2009-3 to EB, and #302724/2011-7 to CAS), Federico Foundation (to RMRP, EB, and CAS), and by Núcleo de Apoio à Pesquisa “Saúde da Criança e do Adolescente” da USP (NAP-CriAd-SP) to CAS.
- Accepted for publication May 29, 2014.








{kind=link}