

Abstract
Objective. To investigate the characteristics of patients with primary Sjögren syndrome (pSS) who have autoimmune cytopenia.
Methods. We analyzed 113 participants from the Korean Initiative of Primary Sjögren Syndrome, a prospective pSS cohort. Autoimmune cytopenia was defined as autoimmune origin neutropenia, anemia, and/or thrombocytopenia without vitamin or iron deficiency, or drug-induced cytopenia. To identify the association between autoimmune cytopenia and the clinical characteristics of pSS, extraglandular manifestations were analyzed according to the European League Against Rheumatism Sjögren’s syndrome disease activity index (ESSDAI) definition. Xerophthalmia was assessed with the Ocular Surface Disease Index, Schirmer I test, ocular stain score (OSS), and tear film breakup time.
Results. The median total ESSDAI score was 2 (interquartile range 1–6). About a quarter of patients had no systemic activity. Autoimmune cytopenia was observed in 23.9% of patients (n = 27). Moderate biological features were more frequently observed in patients with autoimmune cytopenia than in patients without [10 (37%) and 11 (12.8%), respectively, p = 0.016]. Articular involvement was exhibited in 1 patient with autoimmune cytopenia, but in 23 patients (27.4%) without autoimmune cytopenia (p = 0.013). Higher OSS (p = 0.002) and lower mean Schirmer I test (p = 0.029) were observed in patients with autoimmune cytopenia than in those without. Neutrophils and lymphocytes negatively correlated with OSS (ρ = −0.204, p = 0.041 and ρ = −0.230, p = 0.020, respectively).
Conclusion. Autoimmune cytopenia is closely associated with severe ocular surface damage in pSS. Therefore, assessment of xerophthalmia by ophthalmologists may be mandatory, particularly in patients with pSS with cytopenia, even if patients do not complain of eye dryness.
Primary Sjögren syndrome (pSS) is a systemic autoimmune disease that mainly affects the exocrine gland1. The primary features of pSS are keratoconjunctivitis sicca (KCS) and salivary gland dysfunction, which are thought to occur because of lymphocytic infiltration of the exocrine glands2. In addition, extraglandular manifestations (EGM), including arthritis, neuropathy, interstitial lung disease, and renal disease, are observed2,3. The prevalence of EGM varies from 40–50%4 to 86%5. Autoantibodies, such as antinuclear antibodies (ANA), Sjögren syndrome A (SSA)/Ro antibody, Sjögren syndrome B (SSB)/La antibody, and rheumatoid factor (RF), are frequently observed and used as components of classification criteria6,7. Severe EGM generally occur late in the disease course of pSS, and these are associated with serological factors8. Thus, pSS is considered a systemic autoimmune disease.
Autoimmune cytopenia is 1 of the common EGM of pSS. The Sjögren’s International Collaborative Clinical Alliance (SICCA) registry has demonstrated that leukopenia (< 4000/mm3) is observed in 22% of patients with pSS, and anemia (hemoglobin level < 12 g/dl) is observed in 20%9. A Spanish cohort showed that a similar proportion of patients have leukopenia (19.9%) and anemia (17.1%)10, and an Italian cohort8 showed severe neutropenia (< 1500/mm3) or lymphopenia (< 1000/mm3) in 14% of patients. However, only a few studies have been conducted on hematologic abnormalities and their significance in pSS11, and cytopenia is often disregarded in daily practice with patients with pSS because the degree of cytopenia is usually mild and asymptomatic.
In our study, we investigated the prevalence of EGM among participants in the Korean Initiative of primary Sjögren’s syndrome (KISS) cohort, according to domains of the European League Against Rheumatism (EULAR) Sjögren’s syndrome disease activity index (ESSDAI). The EULAR taskforce on Sjögren syndrome developed the ESSDAI that includes all possible EGM and their definitions3. In addition, we investigated cytopenia and other common manifestations of pSS, and their correlation with various phenotypic features of pSS.
MATERIALS AND METHODS
Study population
All patients with pSS in our study were KISS participants. KISS was formed in 2013 with the aim of establishing a nationwide prospective cohort that contained overall clinical data and samples of patients with pSS and to develop diagnostic and treatment tools for pSS. Informed consent was obtained from all patients according to the principles of the Declaration of Helsinki. Our study was approved by the Institutional Review Board of Seoul St. Mary’s Hospital (KC13ONMI0646). All data were collected and managed using the Clinical Research and Trial Management System (iCReaT; Korea National Institutes of Health and Korea Centers for Disease Control and Prevention).
Recruitment began in Seoul St. Mary’s Hospital, a tertiary care university hospital and referral center in Seoul, Korea, in October 2013. By November 2014, the database included 137 patients with pSS from Seoul St. Mary’s who fulfilled the 2002 American-European Consensus group classification criteria7 and/or the 2012 American College of Rheumatology criteria6. Exclusion criteria were radiation history of the head and neck area, chronic hepatitis C or human immunodeficiency virus infections, previous lymphoproliferative disease, sarcoidosis, graft-versus-host disease, amyloidosis, and IgG4-related disease and associated systemic autoimmune diseases such as systemic lupus erythematosus, rheumatoid arthritis, mixed connective tissue disease, primary biliary cirrhosis, vasculitis, autoimmune hepatitis, and systemic sclerosis. Twenty-four patients were excluded from the analysis because they had not completed the case report form.
Assessment of clinical features of pSS
Systemic involvement was defined according to the ESSDAI3 that included 12 domains of EGM. ESSDAI score was assessed by 2 rheumatologists (LJ and KJH) at enrollment. The EULAR Sjögren Syndrome Patient Reported Index (ESSPRI)12 was used for patient-reported dryness, fatigue, and pain. Patient’s global assessment (PtGA) was measured on the same day as the ESSPRI. For evaluating longterm disease consequences, we used the Sjögren’s Syndrome Disease Damage Index (SSDDI)13. Dry mouth was objectively assessed using unstimulated salivary flow rate, and symptoms were assessed using the Xerostomia Inventory (XI; range 11–55)14. A validated questionnaire, the Ocular Surface Disease Index (OSDI; range 0–100)15, was used to assess ocular symptoms and vision-related functions. Schirmer I test, meibomian gland dysfunction16, ocular stain score (OSS)17 using the SICCA method, and tear film break-up time (TBUT) were evaluated by ophthalmologists. These measurements were carried out in both eyes and the worse values obtained were included in analysis. The EQ-5D was used as a generic health-related quality-of-life instrument, and the time tradeoff (TTO) values were derived from South Korean reference data18. Laboratory data were collected from each participant at enrollment for characterization of autoantibodies and quantification of immunoglobulin and complement levels. The ANA titer was determined by an indirect immunofluorescence assay on HEp2 cells, and 1:320 was considered positive. RF was determined by immunoturbidimetric assay. Anti-Ro/SSA antibodies and anti-La/SSB antibodies were tested using commercial ELISA.
Cytopenia was defined as autoimmune cytopenia, such as neutropenia (neutrophil < 1500/mm3), anemia (hemoglobin level ≤ 12 g/dl), and/or thrombocytopenia (platelet count < 150,000/mm3), according to the hematological domain of the ESSDAI3. Cytopenia attributable to vitamin or iron deficiency, drugs, and/or anemia of chronic disease (ACD) was excluded.
Statistical analysis
All data were analyzed using SAS software (Version 9.3). The Shapiro-Wilk test was used to test for departures from normality of distributions for continuous outcome variables. Because patient characteristics were not normally distributed, continuous variables are expressed as median (interquartile range), while categorical data are expressed in absolute and percentage values. When comparing groups, a Mann-Whitney U test was applied to 2 groups of continuous variables (such as white blood cells, hemoglobin, platelet, ESSDAI, ESSPRI, and SSDDI), and the chi-square test was performed for categorical variables. Nonparametric Spearman correlations were used to make comparisons for autoimmune cytopenia and clinical indices. Statistical significance was determined at p < 0.05.
RESULTS
Baseline characteristics
The cohort consisted of 112 women and 1 man, with a median age of 55 years (45–60). The median duration of pSS was 1.6 years (0.4–4.3). Ocular and oral symptoms were assessed according to the 2002 classification criteria. Almost all participants presented oral (98.2%, n = 111) and ocular (99.1%, n = 112) symptoms when they were diagnosed with pSS. Ocular signs, such as ≤ 5 mm in 5 min in the Schirmer I test or ≥ 3 OSS were present in 104 patients (92%). Salivary gland involvement, examined by unstimulated whole salivary flow rate (< 1.5 ml in 15 min) or salivary scintigraphy showing delayed uptake, was observed in 105 patients (92.9%). Minor salivary gland biopsy was performed in 29 patients, and 17 patients (58.6%) had focal lymphocytic sialadenitis with a focus score of ≥ 1 focus/4 mm2. The autoimmune antibody profiles showed ANA ≥ 1:320 in 70.3% of participants, anti-Ro/SSA in 90.8%, anti-La/SSB in 53.2%, and RF in 68.1% (Table 1). The median ESSPRI score was 5.0 (4.2–6.0) and the median PtGA was 63.0 (48.0–78.5). The median SSDDI score was 3 (2–3), and glandular manifestations such as salivary flow impairment (98 cases, 86.7%) and tear flow impairment (89 cases, 78.8%) largely contributed to the SSDDI scores. The median EQ-5D TTO value was 0.84 (0.79–0.89), and the median EQ-5D VAS score was 68.0 (50.0–77.5).
Demographic characteristics of 113 participants with pSS enrolled in the KISS as of November 29, 2014. Values are n (%) or median (IQR) unless otherwise specified.
EGM at baseline
The median total ESSDAI score was 2 (1–6) at enrollment. About a quarter of patients (23.9%, n = 27) had no activity (ESSDAI = 0). The most common positive domain was biological, with 12.4% of patients (n = 14) showing hypocomplementemia and 54% of patients (n = 61) showing hypergammaglobulinemia of more than 16 g/l.
The hematological domain, including autoimmune neutropenia, lymphopenia, thrombocytopenia, and anemia, was observed in 23.9% of patients (n = 27). Anemia was the most frequent hematologic finding (n = 23), but about half of anemia cases (n = 11) were considered to have iron deficiency anemia and ACD. None showed hemolytic anemia at enrollment. Neutropenia was the second most frequent cytopenia (n = 22), and 27.3% of neutropenia (n = 6) was considered induced by drugs or vitamin deficiency. Bicytopenia was observed in 37% of patients with pSS with cytopenia (n = 10), and pancytopenia was observed in 1 case. The prevalence of specific EGM according to the ESSDAI domain is summarized in Table 2. Following the hematological and biological domains, articular involvement was the third most common EGM (n = 24, 21.2%). Pulmonary involvement was observed in 15.0% of patients (n = 17), and only 2 patients showed abnormal lung function test results. Nine participants (8.3%) demonstrated cutaneous lesions, and 2 of these had purpura on the lower extremities. Only 1 patient had nephrocalcinosis with overt hematuria.
Extraglandular manifestations according to the domain of ESSDAI and cytopenia at enrollment. Values are n (%) or median (IQR) unless otherwise specified.
Comparison between patients with pSS with and without autoimmune cytopenia
The age and disease duration of pSS at assessment were similar between patients with and without cytopenia. The proportions of positive anti-SSA/Ro and anti-SSB/La antibody, RF, and ANA ≥ 1:320 were also similar between groups (Table 1). ESSPRI, PtGA, and EQ-5D did not differ according to presence of cytopenia in patients with pSS. SSDDI scores also did not differ between groups.
To determine whether certain EGM were associated with pSS-related autoimmune cytopenia, we compared the prevalence of EGM among the 108 patients with pSS based on presence of autoimmune cytopenia. Arthralgia in small joints accompanied by morning stiffness for more than 30 min was observed in only 1 patient with cytopenia, whereas articular involvement was observed in 27.4% of patients without cytopenia (n = 23, p = 0.013). Among them, 7 (8.4% of patients without cytopenia) had synovitis on 1–5 joints. Hypergammaglobulinemia was observed more frequently in patients with cytopenia than in those without (p = 0.012). In particular, the proportion of those with moderate hypergammaglobulinemia, such as immunoglobulin G level > 2000 mg/dl, was greater for patients with cytopenia (n = 10, 37%) than in those without cytopenia (n = 11, 12.8%, p = 0.016). Hypocomplementemia was observed in 14 patients, and the prevalence did not differ between patients with and without cytopenia. There were no patients with cryoglobulinemia at enrollment. Other manifestations, such as constitutional symptoms, lymphadenopathy, glandular enlargement, cutaneous, and pulmonary and peripheral nervous system involvement did not differ between the 2 groups. In our cohort, no patients showed active muscular and central nervous system (CNS) involvement at enrollment (Table 2).
Associations between autoimmune cytopenia and glandular manifestations of pSS
OSDI scores did not differ between groups (Figure 1A). The median value of the Schirmer I test in patients with cytopenia was 3 mm (0.5–4.8) and 5 mm (2.0–9.0) in those without cytopenia (p = 0.029; Figure 1B). The median OSS according to the SICCA method was significantly higher in patients with cytopenia than in patients without cytopenia [6.0 (4.0–8.0) in patients with cytopenia and 3.5 (2.0–5.0) in patients without cytopenia, p = 0.002; Figure 1C]. In addition, TBUT did not differ between groups [3.0 s (2.0–5.0) in patients without cytopenia and 2.5 s (2.0–3.8) in patients with cytopenia, p = 0.317; Figure 1D]. TBUT was measured in 95 patients, and 94 patients (98.9%) presented tear film instability (< 10 s). Relatively high TBUT (≥ 5 s, 75th percentile of total population) was observed in 20 patients without cytopenia (28.2%) than in those with cytopenia (n = 2, 8.3%, p = 0.050). The proportion of meibomian gland dysfunction grades were similar between the groups (data not shown).
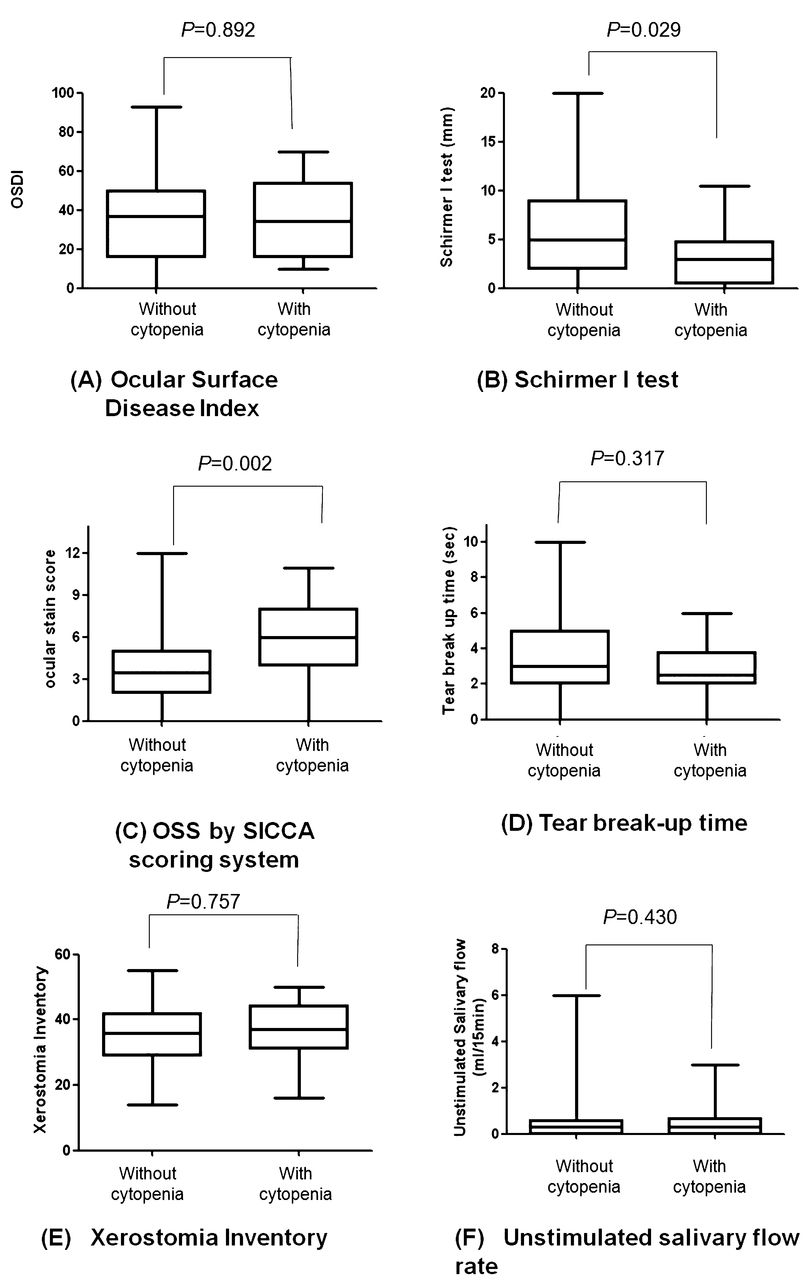
Comparison of (A) OSDI, (B) the mean Schirmer I test, (C) OSS using the SICCA method, (D) TBUT, (E) XI, and (F) unstimulated salivary flow rate in patients with pSS according to the presence of autoimmune cytopenia. OSDI: Ocular Surface Disease Index; OSS: ocular stain score; SICCA: Sjögren’s International Collaborative Clinical Alliance; TBUT: tear film breakup time; XI: xerostomia inventory; pSS: primary Sjögren syndrome.
We investigated dry mouth by XI and measured unstimulated salivary flow rate for 15 min. Those findings did not differ according to presence of autoimmune cytopenia (Figures 1E and 1F).
Correlations between presence of autoimmune cytopenia and clinical index of pSS
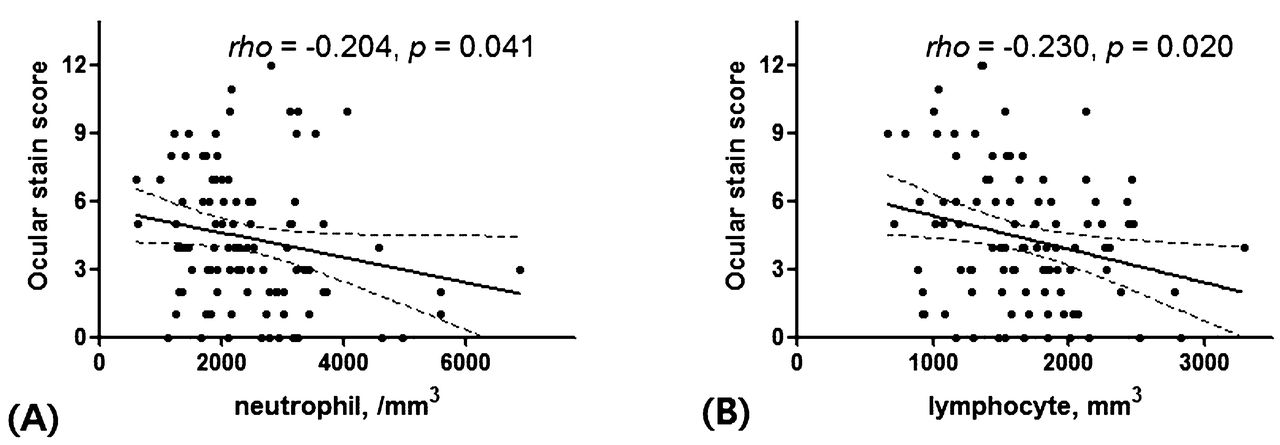
Neutrophil and lymphocytes count at enrollment correlated with OSS according to the SICCA method (ρ = −0.204, p = 0.041 and ρ = −0.230, p = 0.020, respectively; Figure 2). However, OSDI, Schirmer I test, and TBUT did not correlate with autoimmune cytopenia. No significant correlation was found for XI and unstimulated salivary flow rate with autoimmune cytopenia (Table 3).
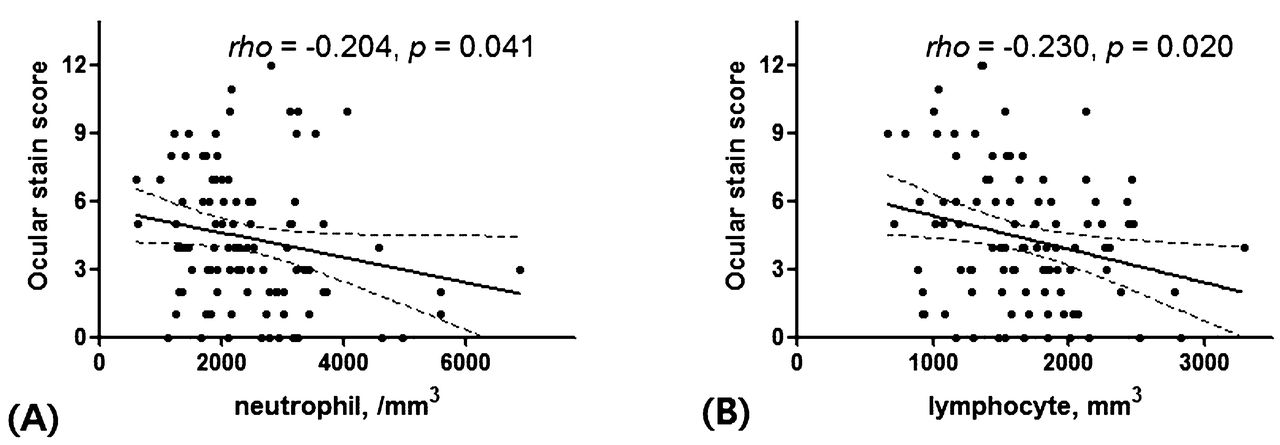
Correlation between neutrophils and lymphocytes counts and OSS. (A) Linear negative correlation was observed between neutrophil counts and OSS. (B) Lymphocytes count was also correlated with ocular stain score.
Simple linear correlations between neutrophils, lymphocytes, and hemoglobin level platelet counts and clinical index of patients with pSS.
DISCUSSION
Our present study reports the clinical and immunological characteristics of patients with pSS at enrollment in a prospective cohort and demonstrates the association between ocular manifestation and autoimmune cytopenia. To our knowledge, ours is the first study to demonstrate the association between autoimmune cytopenia and objective ocular surface damage in patients with pSS.
The prevalence of EGM — for example, renal, muscular, and CNS disease — is low among the KISS participants. The present findings correspond well with those of earlier studies reporting that hypergammaglobulinemia was the most common EGM9,19,20. It is thought to have a strong correlation with circulating autoantibodies, and it implies polyclonal B cell activation. Thus, hypergammaglobulinemia has been studied with regard to its correlation with the development of lymphoma, the most serious complication in pSS20. Although cytopenia is the second most common EGM in pSS, the clinical significance of cytopenia has been relatively underestimated. It has been frequently observed in patients with pSS and usually accompanied hypergammaglobulinemia. In previous studies, hematologic abnormalities have been associated with EGM of pSS9,10,20. However, the definition of hematologic abnormality depended on the counts of each hemocyte, and the range of hematologic abnormality included hypergammaglobulinemia, cryoglobulinemia, and hypocomplementemia. Thus, cytopenias associated with iron or vitamin supply and caused by cessation of offending drugs might be misclassified as an EGM of pSS in those studies. Accordingly, we carefully considered the definition of cytopenia and attempted to include autoimmune cytopenia as a suspected-case EGM of pSS. We also considered hypergammaglobulinemia and hypocomplementemia as biological domains of EGM.
Interestingly, articular involvement may be less common in patients with autoimmune cytopenia. In previous studies, patients with pSS with widespread pain or fibromyalgia were less frequently presented with EGM and anti-La antibody21,22, suggesting that pSS presenting with widespread pain seemed to be of a benign expression. In our cohort, only 1 patient with cytopenia had morning stiffness lasting more than 30 min, whereas 27.4% of patients without cytopenia had arthralgia/arthritis.
In keeping with previous studies, ACD and hypergammaglobulinemia are common at diagnosis and during the course of pSS in the KISS cohort. Neutropenia and cryoglobulinemia at diagnosis are significantly associated with an increased risk of lymphoma development20. Because our present study is based on the first-year data of the KISS cohort, we could not assess the development of serious complications of pSS, such as malignant lymphoma.
Patients with autoimmune cytopenia have more severe KCS than do those without it. Dry eye in pSS can damage the ocular surface, and the range and severity of KCS is assessed using ocular stain score systems. In addition, tear stability has been traditionally measured using TBUT23. Tear film is destabilized when tear secretion is decreased, clearance is delayed, and tear composition is altered24. Dry eye leads to cell apoptosis in the conjunctiva and cornea, and triggers inflammation that contributes to the loss of mucin-producing goblet cells that exacerbates tear film instability25. Tear film instability may be the initiating event of dry eye and acts as a predisposing factor in dry eye complications in response to ocular surface stress24. Thus, lower TBUT and higher OSS in patients with autoimmune cytopenia index decreased tear production and alterations in ocular surface in comparison to patients without autoimmune cytopenia. Autoimmune cytopenia did not affect patient-reported outcomes such as ESSPRI, PtGA, and EQ-5D. Similarly, OSDI was not associated with autoimmune cytopenia. Thus, patients showed early ocular surface damage without symptoms.
There are very weak correlations between the degree of OSDI and the Schirmer I test results and lissamine green or rose Bengal stain scores26. The negative linear correlation between neutrophil, lymphocytes, and OSS may suggest that the active disease state of pSS is associated with severe KCS, although the correlation coefficient was not high. Thus, autoimmune cytopenia as EGM may associate with KCS as the glandular manifestation. A second explanation for our finding is that patients with autoimmune cytopenia could be at a more advanced stage of pSS and could present more severe KCS, although disease duration was not different in patients with and without cytopenia.
A limitation of our current study is that we did not have longterm prognosis data of autoimmune cytopenia because this is the first-year study of our cohort. No patients developed malignant lymphoma in our cohort. However, we considered only autoimmune cytopenia as the EGM of pSS in our study and attempted to exclude other causes of cytopenia.
However, our study has some strengths. We performed various detailed ocular tests, such as OSS using the SICCA method, meibomian gland dysfunction grade, and TBUT. To our best knowledge, ours is the first study to demonstrate the relationship between autoimmune cytopenia and ocular manifestations of pSS. Because our cohort participants followup annually, we will investigate whether ocular surface damage is aggravated more in patients with autoimmune cytopenia, in addition to its consistency, during the followup period.
In three-quarters of patients, pSS is accompanied by systemic manifestations, but it is a generally benign systemic disorder. Autoimmune cytopenia is one of the common manifestations, and is associated with ocular surface damage and decreased tear production. Therefore, in clinical practice, patients with pSS presenting autoimmune cytopenia should be more closely assessed for the severity and range of dry eye.
Acknowledgment
We thank So Young Kim, the research nurse for the Korean Initiative of Primary Sjögren Syndrome cohort, for collecting clinical data. We also thank Jun Pyo Myung of the Department of Occupational and Environmental Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University, for advice on statistical analysis.
Footnotes
Supported by a grant from the Korean Health Technology R&D Project, Ministry of Health and Welfare, Republic of Korea (HI13C0016).
- Accepted for publication June 25, 2015.








{kind=link}
{kind=link}