

Abstract
Objective. Studies on mortality associated with patients with systemic sclerosis (SSc) and myopathy have been limited by heterogeneous definitions of muscle involvement. The objective of this study is to determine whether homogeneous-defined SSc/polymyositis overlap (SSc-PM overlap) is associated with a worse survival rate compared with SSc without PM.
Methods. Data from the Nijmegen Systemic Sclerosis cohort were used. Incidence rates were calculated from the observed number of deaths and followup time. Survival analysis using Cox proportional hazard modeling was performed to compare survival among patients with SSc and patients with SSc-PM overlap, including controlling for confounders. All patients with SSc-PM fulfilled the Bohan and Peter criteria for PM.
Results. There were 24 patients with SSc-PM (5.7%) and 396 patients with SSc (94.2%). The 5- and 10-year cumulative survival rates from diagnosis were 82% and 68% for the SSc-PM group and 93% and 87% for the SSc group, respectively. Multivariate survival analysis revealed an adjusted HR of 2.34 (95% CI 1.09–5.02) for SSc-PM compared with SSc, with age at diagnosis, modified Rodnan skin score, diffuse cutaneous subtype, and male sex included as confounders. The most common cause of death among patients with SSc-PM overlap was cardiopulmonary involvement (63%), which was similar to the patients with SSc (51%).
Conclusion. Patients with SSc-PM overlap have a worse survival rate compared with patients with SSc.
Systemic sclerosis (SSc) is an autoimmune disease characterized by vascular lesions and fibrosis of multiple organs, predominantly in the skin, lungs, heart, intestinal tract, joints, and muscles1,2. The prevalence of myopathies reported in patients with SSc varies from 5% to 81%, also because of the use of the different definitions of muscle involvement3,4,5,6,7,8,9,10,11,12. Myositis in patients with SSc resembles clinical and biological features of patients with polymyositis (PM); hence the term “SSc/PM overlap” (SSc-PM) is used.
SSc-PM is not benign; in several studies, it appeared that the prevalence of myocardial involvement and pulmonary fibrosis is increased in patients with SSc-PM overlap compared with patients with SSc7,9,12. A possible explanation for a poor prognosis for patients with SSc-PM overlap is that SSc-PM overlap could reflect a more active disease with increased presence of systemic complications7,9,12. Increased mortality in patients with SSc and myopathy has been suggested in 2 studies13,14. However, both studies used heterogeneous definitions of SSc myopathy ranging from raised serum to creatine kinase (CK) to reported history of myositis. If indeed the survival rate is worse in patients with SSc-PM overlap compared with patients with SSc, knowledge of the causes of death and organ involvement could support treatment decisions to improve survival rates.
Therefore, the objective of our study was to determine whether patients with SSc with an overlap with PM have a worse survival rate compared with patients with SSc without PM.
MATERIALS AND METHODS
Design
The Nijmegen Systemic Sclerosis cohort is an ongoing, prospective inception cohort which was started in 1989 at the Department of Rheumatology at the Radboud University Medical Center. The data collection contains information on symptoms, physical examinations, and laboratory investigations, as well as annually performed pulmonary function tests, and echocardiography and high-resolution computed tomography scans (HRCT) at first visit and during followup when indicated. According to Dutch law and regulations, because this was an observational, noninterventional study, the study was exempted from approval by a medical ethics committee and no informed consent was required.
Participants
All patients with SSc or SSc-PM of the Nijmegen Systemic Sclerosis cohort were included. Patients with SSc were classified according to the preliminary American College of Rheumatology classification criteria for SSc15. The patients with SSc-PM also fulfilled the Bohan and Peter criteria for probable or definite PM16,17.
Serum CK was routinely measured in all patients with SSc. All patients with SSc with an increase in serum CK of at least 2× the upper limit, myalgia, and proximal muscle weakness had been analyzed for presence of PM with electromyography (EMG) and muscle biopsy. One experienced neuropathologist evaluated all muscle biopsies.
Survival and cause of death
Patients contributed person-years of followup for the period since first diagnosis of SSc as confirmed by a rheumatologist. Followup was terminated at the time of death, dropout, or at the first of January 2012, whichever came first. The causes of death were retrieved from medical records or available autopsy reports. Death rate was calculated from the observed number of deaths divided by the number of patient-years for SSc and SSc-PM groups separately.
Disease definitions
Presence of SSc and of SSc-PM was defined above. Diffuse cutaneous SSc (dcSSc) was defined as patients having skin thickening proximal to the elbows and knees during diagnosis. Limited cutaneous SSc (lcSSc) was defined as the presence of skin thickening distal to the elbows and knees, or in the face at least 2 years after the onset of the first non-Raynaud phenomenon (RP). First non-RP consisted of proximal SSc, sclerodactyly, puffy hands (sausage-like finger edema lasting > 6 mos, or lasting a shorter time but followed by sclerodactyly), or pulmonary fibrosis18.
Skin involvement was evaluated during an interval of 6 weeks after diagnosis using the modified Rodnan skin score (mRSS), which assesses the skin hardening/thickness by manual palpation of 17 body areas on a scale of 0 to 319.
Renal crisis was defined by the occurrence of malignant arterial hypertension (HTN; diastolic blood pressure > 120 mmHg) with grade III or IV hypertensive funduscopic changes according to the Keith-Wagener classification or rapidly progressive oliguric renal failure without other discernible causes during the course of SSc20.
Interstitial lung disease (ILD) was defined as the presence of significant pulmonary fibrosis on HRCT scan and forced vital capacity < 70% of predicted normal and/or DLCO < 70% of predicted.
Pulmonary HTN (PH) was suspected if an experienced cardiologist found a tricuspid regurgitation velocity > 3 m/s or 2.5–3 m/s on echocardiography with unexplained dyspnea21. PH was confirmed when the mean pulmonary arterial pressure was ≥ 25 mmHg at rest, assessed with right heart catheterization (RHC)22. Cardiac dysfunction was defined as a moderate to severe left ventricular systolic dysfunction on cardiac ultrasound or a wedge pressure > 15 mmHg as measured with RHC23.
Statistical analysis
We compared clinical characteristics of patients with SSc and SSc-PM overlap at baseline using the Student t test, Mann-Whitney U test, and chi-square or Fisher’s exact test, as appropriate. Kaplan-Meier cumulative survival plots were used to describe time until occurrence of death or censoring for patients with SSc-PM and without SSc-PM. Survival analysis was carried out by a Cox proportional hazard model using the pooled dataset resulting from multiple imputation. Baseline variables (Table 1) were regarded as confounders if the regression coefficient of the main effect (SSc-PM overlap status) in the Cox proportional model changed by at least 10% when adding the variable to the model using a forward selection approach. Serology and internal organ involvement variables were not included in the analysis because they could possibly serve as causal or explanatory variables regarding the risk difference between SSc and SSc-PM. The risk difference between SSc and SSc-PM overlap was given as adjusted HR (adjHR) with 95% CI when multivariate analysis was performed with correction for confounders.
Clinical characteristics of study population. Values are n (%) unless otherwise specified.
The proportional hazard assumption was checked by graphical inspection of the linearity of the hazards over time and log-log plots. Sensitivity analysis was performed with a different value of the followup time: patient-years since last diagnosis was confirmed (i.e., when both SSc and/or PM diagnosis were confirmed and an overlap diagnosis exists).
We performed all analyses with the SPSS package for Windows 20 (IBM Inc.) and defined statistical significance as a p value ≤ 0.05.
Missing data
Multiple imputation was used for missing values regarding confounders (age, sex, type of SSc, and mRSS) used in the Cox-survival model. Multiple imputation was carried out with a linear regression method with a random component, conditionally on data being missing at random24. Confounding variables age, sex, and type of SSc revealed no missing data. Only missing values of the mRSS were imputed using SSc subset (limited/diffuse cutaneous) and mRSS at another timepoint as predictors. The mRSS was missing in 8% within an interval of 6 weeks during diagnosis and calculated based on 5 imputed datasets. Missing value analysis showed no abnormal pattern.
Missing information for ILD was considered equivalent to no ILD, because patients with missing pulmonary function tests or HRCT scans usually lacked documented pulmonary symptoms or physical findings.
RESULTS
Patient characteristics
By January 2012, a total of 420 patients with SSc followed for 4127 patient-years were included for our analysis. There were 396 patients with SSc (94.2%) and 24 patients with SSc-PM (5.7%). The median (P25–P75) followup time was 7.8 years (3.9–14.1) for the patients with SSc and 6.3 years (4.2–12.9) for patients with SSc-PM.
The mean (SD) age of all patients with SSc at diagnosis was 50 years (13.1), and most patients were women (65%) and were classified as having the limited cutaneous subtype (73%; Table 1). Baseline characteristics were similar between patients with SSc-PM and patients with SSc. However, in 21% of the patients with SSc-PM and in 41% of the patients with SSc, digital ulcers were present (Table 1). More than 95% of the patients were white. The prevalence of the SSc-PM overlap in the Nijmegen Systemic Sclerosis cohort was 5.7%.
Serology and organ manifestations
SSc-specific autoantibodies, namely anticentromere and antitopoisomerase I, were present in 11% and 0% in the SSc-PM group and in 19% and 22% of the SSc group, respectively (Table 1).
The presence of ILD was statistically significantly higher (58% vs 36%) in the SSc-PM overlap group compared with the SSc group (Table 1). Diastolic dysfunction on echocardiography was present in 37% of the SSc-PM group and in 42% of the SSc group. PH was diagnosed in none of the patients with SSc-PM overlap and in 57 patients with SSc. Regarding cardiac involvement and the presence of renal crisis, there were no significant differences between the SSc-PM and SSc groups (Table 1).
Myopathology
Analysis of all muscle biopsies (n = 24) revealed that necrotic muscle fibers and inflammation were the most prevalent features, occurring in 96% (n = 23) and 79% (n = 19; Table 2). Further, fibrosis was seen in 26% (n = 5) and the presence of cytochrome oxidase (COX)-negative fibers in 30% (n = 3) of the muscle biopsies. COX-negative fibers were present in patients over the age of 65 years and therefore were considered an effect of ageing.
Myopathological markers of muscle biopsies slides. Values are n (%).
Survival
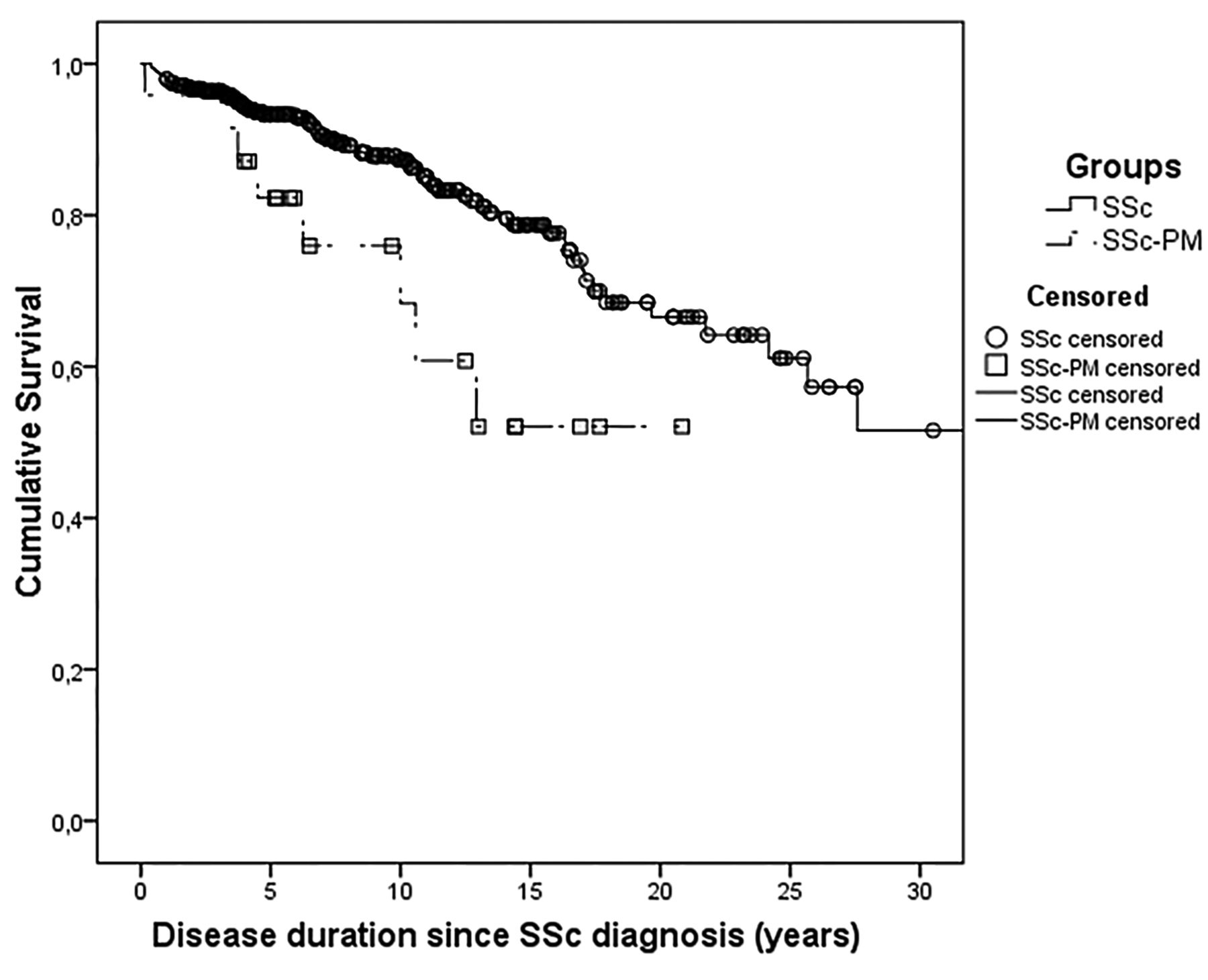
The frequency of death was 73 with 4127 person-years, resulting in a total mortality rate of 1.77 deaths per 100 patient-years. The Kaplan-Meier survival curves of patients with SSc-PM and patients with SSc are shown in Figure 1. For the SSc-PM overlap group, the 5- and 10-year unadjusted cumulative survival rates from diagnosis were 82% and 68%, respectively, compared with 93% and 87% of the SSc group. Unadjusted survival was worse in the patients with SSc-PM as compared with patients with SSc (p = 0.017 log-rank test; Figure 1).

Kaplan-Meier survival curves of patients with SSc-PM and patients with SSc. SSc: systemic sclerosis; SSc-PM: SSc/polymyositis overlap.
Cox-survival model with correction for confounders
The unadjusted and adjusted Cox analysis of the difference in survival between patients with SSc-PM and SSc are shown in Table 3. The model was adjusted for sex, age at diagnosis, mRSS at diagnosis, and SSc subtype (lcSSc/dcSSc).
Results of the Cox proportional hazard survival analysis.
According to both the unadjusted and the adjusted models, survival was significantly worse for patients with SSc-PM in comparison with patients with SSc (Table 3). In the unadjusted model, the HR (95% CI) for patients with SSc-PM overlap (vs patients with SSc) was 2.40 (1.15–5.02). After adjusting for confounders, the adjHR (95% CI) was 2.34 (1.09–5.02), indicating that SSc-PM was associated with a worse survival compared with SSc without PM, after controlling for sex, age at diagnosis, mRSS, and SSc subtype.
On graphical inspection, it appeared that the proportional hazard assumptions were not violated.
Sensitivity analyses
For the primary survival analysis, followup time since the first diagnosis was used. We also performed the analysis with different observation times defined as patient-years since last diagnosis was confirmed (i.e., when both SSc and PM diagnosis were confirmed and an overlap diagnosis existed). Further, we conducted the analysis with observation time since the patients’ first non-RP complaints. There were no differences; the unadjusted and adjusted models remained associated with a worse survival rate for patients with SSc-PM.
Causes of death
The total mortality was 33% in the SSc-PM overlap group, which was significantly higher compared with the patients with SSc, where total mortality was 16% (Table 1). The causes of death in SSc-PM (n = 8) were progressive heart disease (n = 2), myocardial infarction (MI; n = 2), respiratory failure because of ILD (n = 1), sepsis (n = 2), and unknown cause (n = 1). Causes of death in the SSc group (n = 65) were progressive heart failure (n = 7), MI (n = 2), respiratory failure because of ILD (n = 11) or PH (n = 13), malignancies (n = 6), infections (n = 6), and other or unknown causes (n = 20). The most common cause of death among patients with SSc-PM overlap was cardiopulmonary involvement (63%), which was similar to the patients with SSc (51%).
DISCUSSION
In our study, we investigated whether patients with SSc with an overlap syndrome with PM have a worse survival compared with patients with SSc without PM. According to the results of our study, the SSc-PM overlap group showed a 5- and 10-year cumulative survival from diagnosis of 82% and 68% compared with 93% and 87% of the patients with SSc without PM. Univariate and multivariate survival analyses revealed a worse survival for patients with SSc-PM compared with patients with SSc (adjHR 2.34, 95% CI 1.09–5.02). The most common cause of death among patients with SSc-PM overlap was cardiopulmonary involvement (63%).
The prevalence of SSc-PM overlap in our Nijmegen Systemic Sclerosis cohort was low (5.7%) compared with older investigations3,4,5,6,7,9. In more recent studies, prevalences of 7.6% and 7.2%12,25 were observed, which is comparable to our finding. This discrepancy in prevalence compared with more dated studies can be explained by the different criteria used to define SSc myopathy and the different study designs. In our study, we used strict criteria to select only inflammatory myopathies among patients with SSc and not associated myopathies. The use of these strict criteria may have been insensitive to identify all SSc overlap PM cases. However, the criteria we used reflected daily clinical practice in which treating physicians consider invasive diagnostics such as muscle biopsies or EMG, and diagnose by far the most PM overlap cases.
A study by Jung, et al among patients of the Canadian Systemic Sclerosis cohort revealed that being male or having dcSSc, antitopoisomerase I antibody, anti-RNP, and ILD were related to muscle involvement in SSc14. These findings are in line with our results, which also showed the increased presence of men (46%) and ILD (58%) among the SSc-PM overlap group. Further, a Kaplan-Meier analysis in the study by Jung, et al showed a worse survival for patients with SSc with an increased serum CK. In addition, Hashimoto, et al found that overlap with myositis among Japanese patients with SSc was related to a poor prognosis13. The results of Jung, et al and Hashimoto, et al confirm the finding of our study that SSc-PM is related with a worse survival for patients with SSc. Limitations of the study by Jung, et al were that no adjustment for confounders was applied for the survival analysis and an inhomogeneous study population of patients was used ranging from patients with raised serum CK to patients with physician-reported myopathy.
A possible explanation for the poor prognosis for patients with SSc-PM overlap is that SSc-PM overlap could reflect a more active disease with increased presence of systemic complications. Previous studies and our results show an increased presence of pulmonary fibrosis and/or myocardial involvement in patients with SSc and a myopathy7,9,12. Further, the results of our study reveal that cardiopulmonary involvement is the most common cause of death. This should warrant physicians to perform regular screening for this complication and timely initiation therapy. One could argue that patients with SSc-PM overlap could be candidates for stem cell transplantation, because promising results are found in patients with dcSSc26,27.
Limited studies are performed to assess specific immunosuppressive therapy among patients with SSc with a myopathy8,28. Ranque, et al evaluated 35 patients with SSc with a myopathy and found that the presence of histological muscle inflammation was associated with a good muscle prognosis within 3 months of treatment with corticosteroids8. This result should lead treating physicians to consider performing a muscle biopsy to characterize the possible myopathy. Further, the results of Ranque, et al indicate that corticosteroids should be part of the immunosuppressive therapy.
The strengths of our study are the large number of patients, the quality of clinical data, and the length of followup. The Nijmegen Systemic Sclerosis cohort represents the largest sample of patients with SSc in the Netherlands. The data are prospectively collected, with clinical features including information regarding mRSS, laboratory results, pulmonary function tests, echocardiography, HRCT, RHC, and causes of death. Therefore, multivariate survival analysis could be performed with inclusion of major possible confounders. We also performed a sensitivity analysis with different observation time defined as patient-years since last diagnosis was confirmed (i.e., when both SSc and PM diagnosis were confirmed and an overlap diagnosis exist). The outcome was not different, indicating that our results are robust regarding the worse survival for patients with SSc-PM. A sensitive method was used to trace patients with clinical suspicion for PM overlap among our SSc cohort (muscle complaints and a low threshold of 2× upper limit of serum CK). Moreover, muscle biopsy and EMG analysis were then used to diagnose a PM overlap, creating a well-defined homogeneous group of patients with SSc-PM.
A limitation of our study is that all patients were selected from a single tertiary referral center, which potentially could introduce a source of recruitment bias. Given this limitation, a comprehensive, multicenter database with longitudinal patient followup is necessary to fully validate our findings. The small sample size of the SSc-PM overlap cohort makes us concerned about overinterpretation of results. Nonetheless, using strict criteria, we were able to identify a well-defined homogeneous SSc-PM overlap cohort. Underdetection of cardiopulmonary involvement could have occurred, because not all patients underwent HRCT scans or echocardiography. However, we believe underdetection is limited in our study population, because unexplained dyspnea or decline in pulmonary function tests prompted treating physicians to conduct further investigations. Observational studies inevitably face the occurrence of missing values. However, omitting patients with missing values from the analyses would be inefficient and might lead to bias24. Therefore, missing values were imputed by multiple imputation such as the mRSS. Unfortunately, no data concerning SSc-PM overlap-associated antibodies were available, which can be regarded as a limitation to our study.
Patients with SSc-PM overlap have a worse survival compared with patients with SSc. The most common causes of death among patients with SSc-PM overlap were cardiopulmonary, which was similar to the SSc group. These findings underline the need for regular screening for cardiopulmonary involvement in all patients with SSc. Further research should focus on clinical trials to properly evaluate efficacy of different immunosuppressive therapies to improve survival for all patients with SSc and especially patients with SSc-PM overlap.
- Accepted for publication June 29, 2016.








{kind=link}