

Abstract
Objective. To evaluate the effect of rheumatoid arthritis (RA) on impairing women’s sexuality regarding motivation, activity, and satisfaction, and to assess the correlation of disease-related physical impairment within sexual functioning.
Methods. An anonymous survey among women with RA and healthy controls (HC) using standardized questionnaires, predominantly the Changes in Sexual Functioning Questionnaire-short form (CSFQ-14). In addition, disease activity, depression, and disability were evaluated.
Results. There were 319 questionnaires distributed to patients and 306 to HC. Of these, 235 patient questionnaires (73.7%) and 180 HC questionnaires (58.8%) were returned, of which 203 and 169 were completed, respectively. Of the patients with RA, 47.8% had a total CSFQ-14 score of ≤ 41, indicating female sexual dysfunction (FSD), as compared to 14.2% of HC (p < 0.0001). The median CSFQ-14 score was lower in patients with RA [42 points, interquartile range (IQR) 36–48] than in HC (49 points, IQR 44–54; p < 0.0001), resulting in an OR of 5.53 (95% CI 3.19–9.57; p < 0.0001). After adjustment for confounders, given a higher mean age of patients (55.2 ± 11.3 yrs) than HC (47.4 ± 11.8 yrs; p < 0.0001), the OR for FSD in patients with RA was still 3.04 (95% CI 1.61–5.75; p = 0.001). Neither the Health Assessment Questionnaire–Disability Index nor the Clinical Disease Activity Index was associated with FSD after adjustment.
Conclusion. FSD apparently is highly prevalent in female patients with RA, affects all subdomains of sexual function, and is most likely underestimated in daily clinical practice. Of note, FSD could not be linked to disability or RA disease activity.
Inflammatory rheumatic diseases such as rheumatoid arthritis (RA) are characterized by their chronic and progressive features and may lead to premature loss of joint function. RA occurs across all age groups, job categories, and social classes, causing sick leave and occupational disability1. In the last decade, because of a better understanding of the pathogenesis of RA and its progression, highly effective drugs have improved treatment2. Early diagnosis as well as the establishment of an effective therapy within a few months of first symptoms is therefore of paramount importance and an integral part of diagnostic paths and therapeutic guidelines. Apart from conventional synthetic disease-modifying antirheumatic drugs (csDMARD), a steadily increasing group of bDMARD (biologic DMARD) enables stringent disease management3,4,5,6.
Nevertheless, RA constitutes major social, economic, and health burdens and may affect all aspects of life, including patients’ sexuality. Reasons for influencing sexual functioning are multifactorial and comprise disease-related factors as well as therapy7.
RA may influence different areas of partnership such as division of labor within the family and a change in the traditional assignment of roles. The unintentional giving up of joint activities such as sports, combined with a lack of understanding for the disease, can lead to frustration in living together8.
Sexual health is an important part of human well-being and is recognized as an essential part of general health by the World Health Organization. Pain, stiffness, fatigue, and physical limitations of patients with RA could affect sexual functioning. In addition, rheumatic disorders may induce a negative body image and impaired self-esteem9.
As a consequence, people with progressive RA might be affected in all aspects of sexuality, from reduction in sexual desire to impaired arousal and satisfaction, and thus retreat from sexual activity10.
Sexuality is not normally addressed during routine clinical visits for RA and is not an integrated part of most quality-of-life assessment tools11,12. Accordingly, although sexuality is a central part of human existence, very little is known about the burden of sexual dysfunction in women with RA7,9. The number of studies addressing this issue is very small and they differ in patient selection, methods, and conclusions13,14,15.
Therefore, we initiated a comprehensive cross-sectional study. The aim of our study was to investigate the proportion of women with RA, compared to healthy controls (HC), regarding sexual dysfunction, according to the Changes in Sexual Functioning Questionnaire-short form 14 (CSFQ-14)16.
MATERIALS AND METHODS
Study design and ethics
This cross-sectional study is in compliance with the Declaration of Helsinki. All participants gave written informed consent. The study was approved by the relevant local ethics committees (Ethics Committee of Upper Austria: Approval No. L-26-15).
Setting
Patients were recruited from 4 hospital-based outpatient clinics and 3 office-based rheumatologists, between October 2015 and October 2016. Patients with RA aged ≥ 18 years were included as cases. Patients were eligible for the study when they fulfilled the European League Against Rheumatism/American College of Rheumatology 2010 classification criteria17. Women ≥ 18 years of age, without an inflammatory rheumatic condition, many of them attending the practice for a health check, were included as a control group (HC). HC attended to see a general practitioner or a specialist in internal medicine. Patients and HC received detailed information about the study and were instructed on how to fill in the questionnaire. All participants received an addressed return envelope. To ensure absolute anonymity, all study participants were instructed to strictly avoid any personal notes on envelopes and questionnaires. During the patient visit, medical information (concerning disease, disease activity, and medication) was filled in by the treating physician. Then, the form was handed over to the patient, who was asked to fill in all the other information at home. The patient was further asked to use the enclosed envelope to anonymously send the form to the Centre of Excellence in Medicine in Linz, Austria, where all questionnaires were collected. Alternatively, patients could choose to fill in the forms during their visit, in the hospital or office waiting area, and then put the questionnaire into the envelope and the envelope into the locked box provided. This box was then sent to the Centre of Excellence in Medicine, a suborganization of the Austrian Medical Association that has been involved in processing numerous questionnaires in healthcare for over 20 years.
Variables and data sources
The main exposure variable was RA. Physicians were instructed to register age and current medication on the questionnaire. For patients with RA, physicians also recorded date of RA diagnosis, presence of rheumatoid factor and anticitrullinated proteins/peptides, tender joint count in 28 joints, swollen joint count in 28 joints, patient’s global assessment, and physician’s global assessment. The last 4 variables were used to calculate the Clinical Disease Activity Index (CDAI)18. In addition, medication was registered, particularly DMARD and glucocorticoids. The DMARD were grouped: csDMARD (methotrexate, sulfasalazine, leflunomide, hydroxychloroquine) as well as bDMARD (adalimumab, etanercept, infliximab, golimumab, certolizumab pegol, rituximab, abatacept, tocilizumab).
All patients and controls self-reported religion, comorbidities, weight, height, alcohol consumption, and smoking status. In addition, the questionnaire contained questions regarding contraception, menstruation, pregnancies, births, marital status, and employment status. Data were collected concerning “help seeking” for sexual problems, by using some open and closed questions.
The questionnaire contained the validated German version of the CSFQ-1419 and the Beck Depression Inventory–Fast Screen (BDIFS)20,21,22,23,24. In addition, patients with RA also filled in the Health Assessment Questionnaire–Disability Index (HAQ-DI)25.
The CSFQ-14 is a self-reporting questionnaire and covers all stages of sexual functioning16,19,26,27. More detailed information concerning methods is given in Supplementary Data 1 (available with the online version of this article).
Statistical methods
The primary endpoint was the proportion of women with FSD according to the CSFQ-14. All further tests are exploratory, not confirmatory.
For statistical analysis, we used only data from patients and healthy women with complete information on the CSFQ-14 (203 patients with RA and 169 HC). Accordingly, data of 31 patients with RA and 12 women in the control group with incomplete CSFQ-14 had to be excluded. We tested categorical data with the chi-square test and calculated, where appropriate, a test for trend. In addition, we calculated OR and 95% CI. For comparison of continuous data following Gaussian distributions, we used unpaired Student t tests. If continuous data departed from a near-normal distribution, we used the Wilcoxon rank-sum test. We used logistic regression for multivariable analyses with a binary outcome.
A p value < 0.05 was accepted as statistically significant. We performed all analyses with Stata Statistical Software: Release 13 IC (StataCorp LP) or ALMO statistics system (www.almo-statistik.de)28. For more statistical details, see Supplementary Data 1 (available with the online version of this article).
RESULTS
A total of 625 questionnaires were distributed to 319 patients with RA and 306 HC. In total, 415 questionnaires were sent back: 235/319 (73.7%) handed out to patients with RA, and 180/306 (58.8%) given to HC. After eliminating questionnaires with missing data, the CSFQ-14 score could be calculated for 203 of the patients with RA (63.6%) and 169 of the HC (55.2%). Mean RA disease duration was 12.0 ± 10.1 years. Characteristics of RA patients and HC are shown in Table 1.
Characteristics of patients with RA and HC.
The median CSFQ-14 score was lower in patients with RA [42 points, interquartile range (IQR) 36–48] than in HC (49 points, IQR 44–54; p < 0.0001; Figure 1). Using the recommended threshold of ≤ 41 points in the CSFQ-14 score as an indicator of FSD, the percentage of women with FSD was higher in the RA group (97/203, 47.8%) when compared to HC (24/169, 14.2%; p < 0.0001). In each of the subsections of the CSFQ-14, female patients with RA had a lower score than HC (Table 2 and Table 3). Accordingly, in an unadjusted analysis, RA was strongly associated with FSD (OR 5.53, 95% CI 3.19–9.57; p < 0.0001) when compared to HC. Figure 2 shows the situation for RA and healthy individuals in 10-year strata.
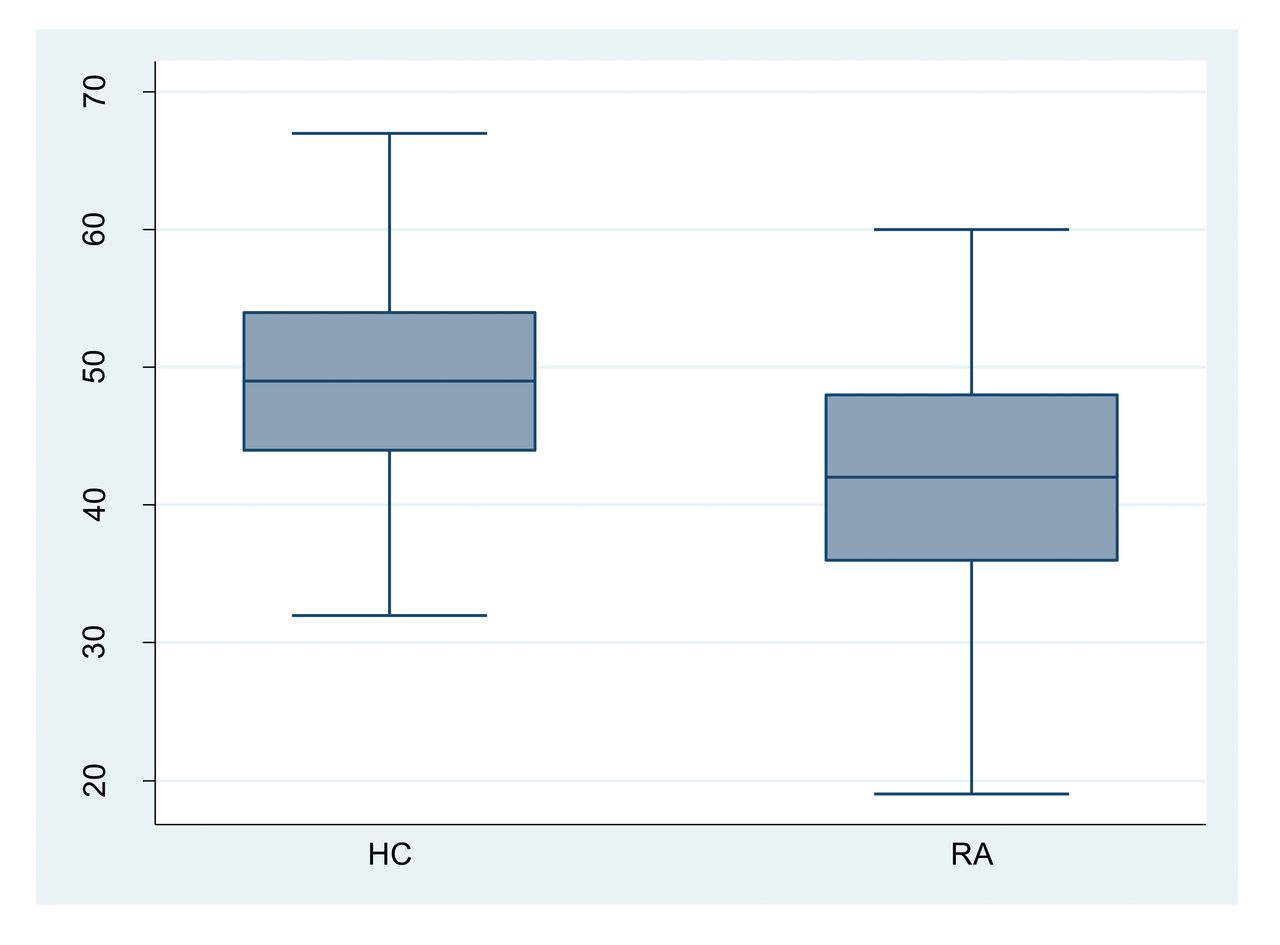
CSFQ score for HC and patients with RA. HC have a higher total CSFQ score compared to patients with RA (p < 0.0001). CSFQ: Changes in Sexual Functioning Questionnaire-short form; RA: rheumatoid arthritis; HC: healthy controls.
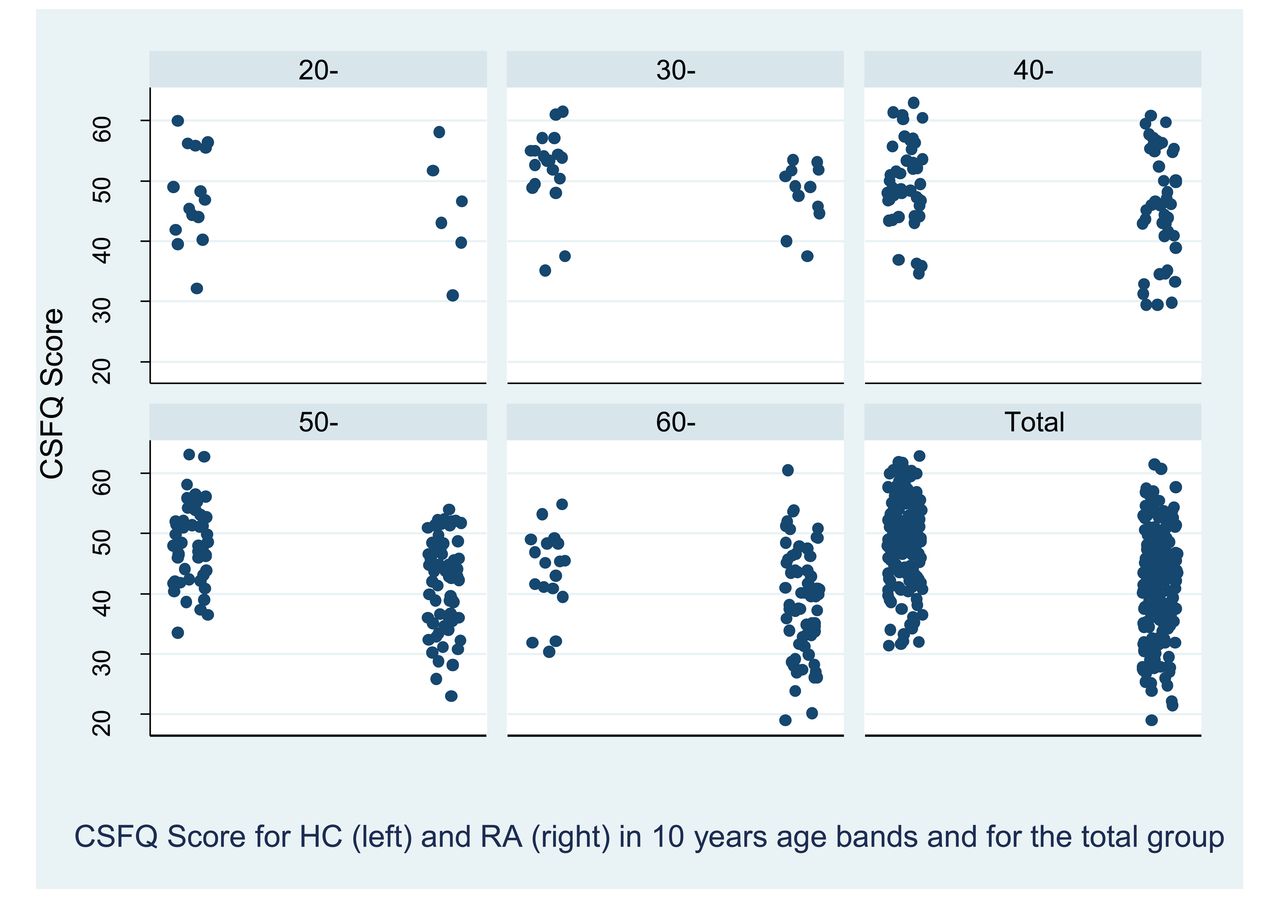
Dot blot shows the situation for RA and HC in 10-year strata. CSFQ: Changes in Sexual Functioning Questionnaire-short form; RA: rheumatoid arthritis; HC: healthy controls.
Comparison of FSD in patients with RA and HC.
Scoring for CSFQ.
Some of the patient characteristics were found to be distributed unequally between the 2 groups analyzed. The mean age of the 203 remaining patients with RA was 55.2 ± 11.3 years, significantly higher than for the 169 HC (47.4 ± 11.8 yrs, p < 0.0001). In addition, as shown in Table 1, patients with RA were less likely to drink alcohol, had lower levels of education, and were less likely to be employed.
RA patients with FSD were older than RA patients without FSD (58.4 ± 10.3 vs 51.0 ± 11.0 yrs; p < 0.0001). In general, there was a strong trend for increasing odds of FSD within a higher age category (OR 1.68 per age category, 95% CI 1.38–2.05; p < 0.0001).
After adjustment for the confounders’ age, education level, employment status, and alcohol consumption, the OR for FSD in patients with RA was still 3.04 (95% CI 1.61–5.75; p = 0.001). Adjustment for the comorbidities, specifically diabetes mellitus, arterial hypertension, coronary heart disease, congestive heart failure, and peripheral arterial occlusive disease, did not significantly alter the association between RA and FSD (OR 2.84, 95% CI 1.42–5.68; p = 0.003; Supplementary Figure 1, available with the online version of this article).
A significant relationship was found between BDI and sexual dysfunction. Patients with RA have a significantly higher risk of depression. In the RA group, 66/223 (29.6%) had a BDI score ≥ 4. In the HC group, 21/169 (12.4%) had a BDI score ≥ 4 (p < 0.0001). However, the association of RA and FSD was also adjusted for BDI-FS in an exploratory way (see Materials and Methods); the OR for reduced sexual function remained statistically significant (2.67, 95% CI 1.39–5.13; p = 0.003; Table 4).
Multivariable analysis of RA as well as confounders and FSD (as defined by a CSFQ score of ≤ 41). This analysis includes BDI-FS.
Use of csDMARD (OR 1.30, 95% CI 0.65–2.63; p = 0.4565) or bDMARD (OR 1.43, 95% CI 0.82–2.51; p = 0.2064) was not associated with FSD. In addition, glucocorticoid use was not associated with FSD (OR 1.22, 95% CI 0.51–2.91; p = 0.6552). In an unadjusted analysis, disability, as measured by HAQ-DI, appeared to be associated with FSD. However, this association was no longer statistically significant after adjustment for age, education level, employment status, and alcohol consumption (see Supplementary Table 1, available with the online version of this article). An additional adjustment for the BDI category did not substantially alter the results (test for trend of odds: p = 0.6225). Likewise, disease activity, as measured by CDAI, was not significantly associated with FSD. In a sensitivity analysis, we combined the CDAI “moderate” and “high” strata to a “moderate/high” stratum and recalculated the association between CDAI category and FSD. Again, we could not find a statistically significant association between CDAI category and FSD (p for trend = 0.4381).
This was true for both an unadjusted and adjusted analysis for age, education level, employment status, and alcohol consumption (see Supplementary Table 1, available with the online version of this article). Again, an additional adjustment for the BDI category did not substantially alter the results (test for trend of odds: p = 0.4895). In addition, CSFQ-14 was also not correlated with patient’s global assessment (ρ = −0.0817; p = 0.25).
For a total of 375 women, we had information on dryness. Fifty-six women (14.93%) reported that they had dryness of the mucous membranes, while 319 women (85.07%) stated that they did not experience dryness. Dryness was significantly associated with RA (OR 3.78, 95% CI 1.90–7.55; p < 0.0001; see also Table 1). In addition, dryness was strongly associated with FSD (OR 5.10, 95% CI 2.64–9.87; p < 0.0001). Adjustment for dryness in the multivariable analysis slightly reduced the association between RA and FSD; however, the association remained statistically significant (OR 2.45, 95% CI 1.23–4.91; p = 0.011).
Sixteen patients (6.8%) and 4 HC (2.2%; p = 0.031) had used professional help because of a sexual problem. Only 5 (6.7%) out of 75 patients (answering this question) thereby contacted their rheumatologist. According to some of the open answers in our questionnaire, patients did not feel there is enough time to discuss a sexual problem during routine clinical visits. They said they felt embarrassed to raise their problem or that the rheumatologist was perhaps the wrong person to whom to disclose this kind of sensitive, personal information.
Seventy-two out of 229 patients (31.4%) said that RA harmed their sexuality. Of these, 66 women specified problems: lack of sexual desire (86%), dryness (25%), and pain during intercourse (14%; multiple answers were possible).
RA had had an adverse effect on their relationship in 18% of the respondents in our survey; 81% of these women discussed this problem with their partner.
DISCUSSION
In our study population of female RA patients with a mean age of 55 years, almost half had an FSD indicative of sexual dysfunction, about 3 times higher than in women without an inflammatory rheumatic disorder. Even after adjustments for confounders, the OR for FSD in patients with RA was impressively high (OR 3.04, 95% CI 1.61–5.75; p = 0.001). It is very likely that this point is substantially underestimated in daily clinical practice. Only a small proportion of patients with RA were seeking professional help or decided to discuss this topic with their rheumatologist. There could be many reasons for sexual dysfunction in women with RA, including aspects related to the disease itself as well as to treatment, a limited performance owing to physical disability, and emotional, social, and cultural factors9.
Of patients with RA, 21.9% reported dryness of the mucous membranes. Being aware of the effect of dryness on well-being and quality of life, it is obligatory to evaluate patients with primary Sjögren syndrome in this regard during their medical visits29. According to our findings, this problem should be addressed in patients with RA more often because it can be 1 reason for FSD that could be tackled quite easily. Patients with inflammatory rheumatic diseases more frequently have comorbidities such as fatigue and depression, which are known to impair sexuality23,24,30,31. The prevalence of depression in patients with RA is between 10% and 45%, depending on various methods of measurement, types of surveillance, and cultural influences31. In contrast, we could not find an association of FSD with disability (HAQ-DI) or disease activity (CDAI). Therefore, according to our data, the assumption that RA patients with more active or debilitating RA are, in particular, those who have FSD may be an oversimplification. Conversely, RA patients with well-controlled disease may still have FSD, a point that could be easily missed in daily clinical practice.
The effect of rheumatic disease on sexual relationships has been mentioned in a limited number of previously published papers. These studies, specifically dealing with FSD in RA, differ from each other in several pivotal points: in the small number of participants, in the inclusion of both men and women, in a low return rate, or in the lack of a control group. It is worth mentioning that some of them were conducted in culturally and religiously different cohorts, which makes a big difference in this issue and is a restricting factor in terms of comparability9,10,11,13,14,15,30.
The 48.5% of RA patients with FSD in our study are well in the range reported in the literature: from 31% to 76%7,9,11. Comparing our patients with HC, we found a statistical difference in almost all domains of the measured sexual functions, such as sexual pleasure, desire, arousal, and completion (Table 3). This is in line with the study by Khnaba, et al9 and a systematic review done by Zhang, et al32. This review included 5 studies, each of them comprising only small numbers of participants (between 32 and 104; 3 studies from Turkey, 1 from Morocco, and 1 from Iran). As listed by Zhang, et al as a limitation, the high statistical heterogeneity might reduce the generalization of the results. Because of limited data, they did not analyze the influence of co-factors such as disease activity, disability, or depression on FSD, which we explicitly did. To our knowledge, our study is the first on this topic, focusing on women in a Western cohort.
Factors that had an independent effect on sexual function in our study were depression, level of education, employment status, alcohol consumption, and age. Compared to a study by Yilmaz, et al33, disease activity had no influence on sexual function in women with RA. It might be that we did not find such an association, as 74.4% of our patients were in remission or in low disease activity. However, our data are in line with Costa, et al, who also found no association between disease activity or functional disability and FSD11. That BDI is associated with FSD is not a surprise, because they are strongly interrelated. On the one hand, depression can lead to FSD; on the other hand, FSD may cause depression23. However, RA itself is also associated with depression and it is speculated that the chronic inflammatory state itself may be 1 causative factor in the development of depression22. Therefore, adjustment for depression may underestimate the association of RA and FSD. In our analysis, we present both calculations. We found that the association of RA and FSD is still strong after adjustment for BDI. Fatigue is a common symptom affecting patients with RA, and fatigue may also be associated with FSD. However, as with depression, fatigue appears to be on the causal pathway between RA and sexual dysfunction. Therefore, fatigue should be seen as an intermediate (i.e., a variable on the causal pathway), and not as a confounder.
Only 6.8% of the patients with RA used professional support to treat a sexual problem. Just 6.7% of patients with RA discussed a sexual problem with their rheumatologist. One may ask: Is this so because questions concerning sexual dysfunction are not asked by rheumatologists? According to some of the open answers in our questionnaire, patients did not feel there is enough time to discuss a sexual problem during routine clinical visits, they felt embarrassed to raise their problem, or they thought the rheumatologist was perhaps the wrong person to whom to disclose this kind of sensitive, personal information. According to our data, strategies to improve the management of (unrecognized) sexual dysfunction in patients with RA are needed. One option might be to train healthcare professionals in relevant departments to broach the subject and then advise the patient on the best course of action. This and other solutions need further discussion11. Of note, in the United Kingdom, a telephone survey was conducted and completed by 1500 individuals, using a structured questionnaire covering sexual behavior, attitudes, and beliefs. Of these, 16.7% of women reporting a sexual problem had discussed it with a doctor; however, 32.5% talked to their partners34.
One of the strengths of our study was the high number of participants. There were 235 questionnaires from patients and 180 from HC that were sent back, yielding a response rate of 73.7% in patients with RA and 58.8% in HC. Given the sensitive topic of the study, this return rate is quite high and reduces the risk of selection bias. A return rate of > 50% is desirable but very rare in questionnaire surveys30. We used a validated questionnaire to assess FSD, which makes comparisons with future studies possible. Our study has some limitations. It is a cross-sectional study, which does not allow the interpretation of a cause-effect relationship. There was a high percentage of patients treated with bDMARD (45%), much higher than the expected average of about 25% in the population35. This may limit generalizability. Maybe the respondents to our study were under close surveillance, and more motivated to participate in the survey. Our efforts to ensure anonymity of study participants not only resulted in a high return rate, but also excluded the possibility to track back any patient information. We were unable to query any missing data (e.g., for the calculation of missing items in the CSFQ-14). This may also explain the unequal distribution of a number of characteristics between the study groups. We accounted for these factors by giving unadjusted as well as adjusted results. Another limitation of our study is that HC were selected in offices. The sensitive topic of this survey was the reason to intentionally choose this way of recruitment, assuming that a trustful relationship between doctor and individual would enhance the response rate for the control group. Indeed, this approach led to a high return rate of 58.8% for controls. Finally, we investigated sexual dysfunction in women, who represent the majority of patients with RA. Therefore, our study cannot give any conclusions concerning sexual dysfunction in men, and further research is necessary in this field.
FSD is highly prevalent in female patients with RA, affects all subdomains of sexual function, and is most likely underestimated in daily clinical practice. Of note, FSD is independent of disability and disease activity. Although FSD affects a large number of female patients with RA, only a minority have decided to discuss this problem with their rheumatologist or are seeking professional help elsewhere. Thus, questions to address these aspects should be asked when evaluating the course of disease. Rheumatologists and healthcare providers have to be aware of the possibility of FSD in patients with RA and ought to provide therapeutic options.
ONLINE SUPPLEMENT
Supplementary material accompanies the online version of this article.
Acknowledgment
We thank Prof. Anita Clayton, University of Virginia, for permission to use the CSFQ-14 for our research without any fee.
Footnotes
This work was supported by an unrestricted industrial grant from Pfizer Austria [grant number WI205954].
- Accepted for publication June 14, 2018.








{kind=link}
{kind=link}