

- Department of Neurosurgery, University Hospitals Leuven, Belgium
- Department of Neurosurgery, International Neuroscience Institute, D-30625 Hannover, Germany
Correspondence Address:
Hamid Reza Niknejad
Department of Neurosurgery, International Neuroscience Institute, D-30625 Hannover, Germany
DOI:10.4103/2152-7806.161416
Copyright: © 2015 Niknejad HR. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.How to cite this article: Niknejad HR, Samii A, Shen S, Samii M. Huge familial colloid cyst of the third ventricle: An extraordinary presentation. Surg Neurol Int 23-Jul-2015;6:
How to cite this URL: Niknejad HR, Samii A, Shen S, Samii M. Huge familial colloid cyst of the third ventricle: An extraordinary presentation. Surg Neurol Int 23-Jul-2015;6:. Available from: http://surgicalneurologyint.com/surgicalint_articles/huge-familial-colloid-cyst-of-the-third-ventricle-an-extraordinary-presentation/
Abstract
Background:Since the use of computed tomography and magnetic resonance imaging, colloid cysts (CCs) are discovered more frequently and subsequently their true incidence exceeds the numbers previously estimated. In 1986, the first familial case was reported in two identical twin brothers. To date, a total of 17 of these cases have been reported, all differing in the pattern of affected family members.
Case Description:Here, we describe a unique presentation of a familial case and review the relevant literature on CCs and their natural history to improve our understanding of these cases.
Conclusion:Familial CC can present in various patterns, sizes, and forms. A genetic factor is likely to be responsible in these cases, and further research is warranted to clarify this phenomenon.
Keywords: Colloid cyst, familial, genetics, tumor
INTRODUCTION
Colloid cysts (CC's) of the third ventricle are benign intra-cranial cysts that account for approximately 1% of all intra-cranial tumors. Considering the intraventricular lesions only, they comprise up to 20% of all tumors, and they are the most common mass found in the third ventricle.[
They mainly present with signs and symptoms related to hydrocephalus such as headache and nausea, which are too unspecific to pinpoint an exact etiology. On the other hand, we have the silent cases diagnosed incidentally by means of magnetic resonance imaging (MRI) or computed tomography (CT).[
To date, a total of 17 familial cases has been reported.[
CASE REPORTS
First case
In 2006, a 43-year-old Saudi man was referred to our institution, the International Neuroscience Institute in Hannover, for the treatment of a cystic intra-cranial lesion. During the week before admission, the primary complaint was sudden onset headaches accompanied by episodes of vomiting. At the time of evaluation, the headaches were described as constant, very severe and diffuse. Sensorimotor evaluation showed mild numbness in the right hand, with a slight weakness of the hand extensors on the right side. A CT-scan performed in the country of origin revealed a cystic lesion that appeared to be a CC of the third ventricle. On T1-weighted gadolinium-enhanced images a 25 mm × 25 mm × 20 mm measuring cystic lesion was seen [
The patient underwent a right fronto-dorsal parasagittal craniotomy for a microsurgical extirpation of the lesion through a transcallosal approach. Total removal of the cyst and its colloidal content, together with its aberrant vascular steel was achieved.
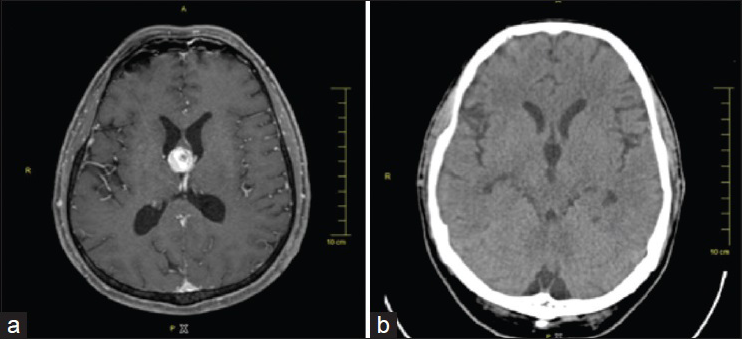
Figure 1
First case. (a) Preoperative gadolinium enhanced T1-weighted axial magnetic resonance imaging, showing an in homogenously enhancing mass in the third ventricle causing mild hydrocephalus. (b) Postoperative axial computed tomography-scan showing complete removal of the lesion and absence of hydrocephalus
Histological examination of the biopsy specimens confirmed the diagnosis of a CC. Surprisingly, the vascular steel consisted of a cluster of markedly abnormal arteries together with tortuous and dilated veins, in accordance with our pathological diagnosis of an arteriovenous malformation (AVM).
Postoperatively the patient recovered quickly and there were no complications. At discharge, the headaches and vomiting were no longer present and the patient was free of any other neurological deficits.
Second case
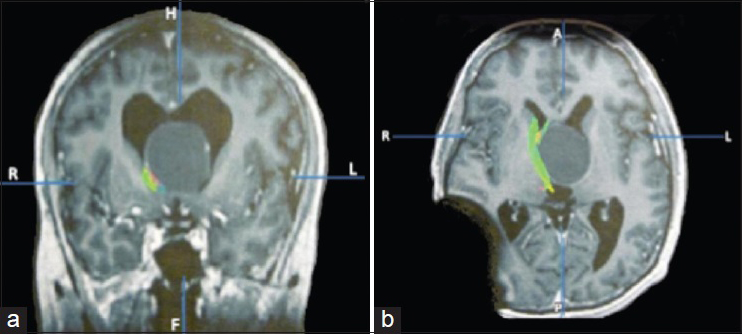
After a 6-year interval, the 39-year-old brother of our first patient was admitted to our clinic with a 1-month history of vertigo together with episodes of nausea and vomiting. One week prior to admission the patient had lost consciousness after having an acute onset headache and was transported to a local hospital. His past medical history and familial history were unremarkable for brain diseases. However, a detailed familial history was not obtained, nor were any other family members examined at our center. A CT-scan was performed showing hydrocephalus and a huge cystic lesion in the third ventricle. In the acute setting, he was treated by means of a ventricular drain. Preoperative gadolinium-enhanced T1-weighted MRI showed a huge, 52 mm × 42 mm × 39 mm measuring, hypointensive cystic lesion in the third ventricle that had progressively expanded upward to the corpus callosum, displacing the septum pellucidum and bulging in the lateral ventricles [
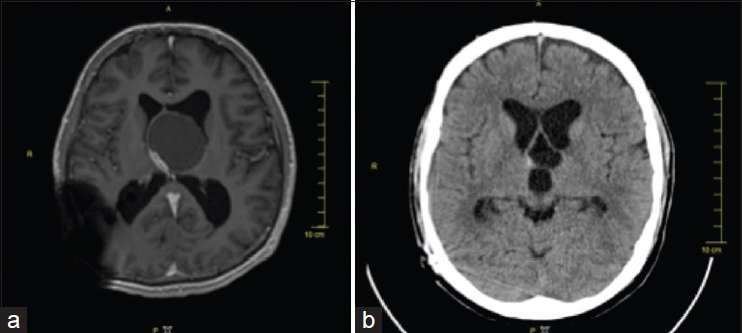
Figure 2
Second case. (a) Preoperative gadolinium enhanced T1-weighted axial magnetic resonance imaging, showing a gigantic cystic lesion in the third ventricle causing hydrocephalus. Note the enhancing vessels on the cyst wall. Artifact is due to the occipital venticuloperitoneal-shunt. (b) Postoperative axial computed tomography-scan showing extirpation of the cyst content and no signs of increased intra-cranial pressure
DISCUSSION
The origin of colloid cysts
Ever since their discovery, CC's have remained a curious clinicopathological entity. More than a century ago Sjovall presumed the cysts originated out of the paraphysis cerebri, an evanescent vestigial embryonic structure.[
Colloid cysts and genetics
Another approach of trying to clarify the mechanisms involved in the development of familial CC's is the search for a genetic abnormality that could lead to an inheritable disease. Interestingly in this respect, insights into the function of “paired”-like homeodomain transcription factor (Prop1) in the development of the Rathke's pouch, the pituitary primordium, have been described in mice. Prop1 seems to have a crucial role in cell proliferation and differentiation and thus in the organogenesis and function of the pituitary gland. A dysregulation in Prop1 expression is correlated with an increased susceptibility for pituitary tumors and Rathke's cleft cysts. The latter were found in 40% of the alpha glycoprotein subunit (αGSU)-Prop1 transgenic mice, which express a high level of Prop1 under the αGSU promoter (gain of function).[
References
1. Aggarwal A, Corbett A, Graham J. Familial colloid cyst of the third ventricle. J Clin Neurosci. 1999. 6: 520-2
2. Ahmed SK, Stanworth PA. Colloid cysts of the third ventricle in identical twins. Br J Neurosurg. 2002. 16: 303-7
3. Akins PT, Roberts R, Coxe WS, Kaufman BA. Familial colloid cyst of the third ventricle: Case report and review of associated conditions. Neurosurgery. 1996. 38: 392-5
4. Antunes JL, Louis KM, Ganti SR. Colloid cysts of the third ventricle. Neurosurgery. 1980. 7: 450-5
5. Bavil MS, Vahedi P. Familial colloid cyst of the third ventricle in non-twin sisters: Case report, review of the literature, controversies, and screening strategies. Clin Neurol Neurosurg. 2007. 109: 597-601
6. Bengtson BP, Hedeman LS, Bauserman SC. Symptomatic neuroepithelial (colloid) cysts of the third ventricle. A unique case report in nontwin brothers. Cancer. 1990. 66: 779-85
7. Benoiton LA, Correia J, Kamat AS, Wickremesekera A. Familial colloid cyst. J Clin Neurosci. 2014. 21: 533-5
8. Britt RH, Silverberg GD, Enzmann DR, Hanbery JW. Third ventricular choroid plexus arteriovenous malformation simulating a colloid cyst. Case report. J Neurosurg. 1980. 52: 246-50
9. Buchsbaum HW, Colton RP. Anterior third ventricular cysts in infancy. Case report. J Neurosurg. 1967. 26: 264-6
10. Camacho A, Abernathey CD, Kelly PJ, Laws ER Jr. Colloid cysts: Experience with the management of 84 cases since the introduction of computed tomography. Neurosurgery. 1989. 24: 693-700
11. Coxe WS, Luse SA. Colloid cyst of third ventricle. an electron microscopic study. J Neuropathol Exp Neurol. 1964. 23: 431-45
12. Cushman LJ, Watkins-Chow DE, Brinkmeier ML, Raetzman LT, Radak AL, Lloyd RV. Persistent Prop1 expression delays gonadotrope differentiation and enhances pituitary tumor susceptibility. Hum Mol Genet. 2001. 10: 1141-53
13. Dandy WE. Diagnosis, localization and removal of tumours of the third ventricle. Bull Johns Hopkins Hosp. 1922. 33: 188-9
14. del Carpio-O’Donovan R, Cardinal E. Agenesis of the corpus callosum and colloid cyst of the third ventricle: Magnetic resonance imaging of an unusual association. Can Assoc Radiol J. 1990. 41: 375-9
15. Fulton JF. Harvey Cushing: A Biography. Spring-field: Charles C Thomas. 1946. p. 713-4
16. Gelabert M, Bollar A, Martinez R, Allut AG. Coincidence of a frontal lobe astrocytoma and colloid cyst of the third ventricle. Neurochirurgia (Stuttg). 1991. 34: 69-70
17. Gemperlein J. Paraphyseal cysts of the third ventricle. Report of two cases in infants. J Neuropathol Exp Neurol. 1960. 19: 133-4
18. Graziani N, Dufour H, Figarella-Branger D, Donnet A, Bouillot P, Grisoli F. Do the suprasellar neurenteric cyst, the Rathke cleft cyst and the colloid cyst constitute a same entity?. Acta Neurochir (Wien). 1995. 133: 174-80
19. Hadfield MG, Ghatak NR, Wanger GP. Xanthogranulomatous colloid cyst of the third ventricle. Acta Neuropathol. 1985. 66: 343-6
20. Hamlat A, Casallo-Quiliano C, Saikali S, Adn M, Brassier G. Huge colloid cyst: Case report and review of unusual forms. Acta Neurochir (Wien). 2004. 146: 397-401
21. Heafner MD, Duncan CC, Kier EL, Ment LR, Scott DT, Kolaski R. Intraventricular hemorrhage in a term neonate secondary to a third ventricular AVM. Case report. J Neurosurg. 1985. 63: 640-3
22. Hernesniemi J, Romani R, Dashti R, Albayrak BS, Savolainen S, Ramsey C. Microsurgical treatment of third ventricular colloid cysts by interhemispheric far lateral transcallosal approach – Experience of 134 patients. Surg Neurol. 2008. 69: 447-53
23. Ho KL, Garcia JH. Colloid cysts of the third ventricle: Ultrastructural features are compatible with endodermal derivation. Acta Neuropathol. 1992. 83: 605-12
24. Ibrahim AW, Farag H, Naguib M, Ibrahim E. Neuroepithelial (colloid) cyst of the third ventricle in identical twins. Case report. J Neurosurg. 1986. 65: 401-3
25. Joshi SM, Gnanalingham KK, Mohaghegh P, Wilson A, Elsmore A. A case of familial third ventricular colloid cyst. Emerg Med J. 2005. 22: 909-10
26. Kappers JA. The development of the paraphysis cerebri in man with comments on its relationship to the intercolumnar tubercle and its significance for the origin of cystic tumors in the third ventricle. J Comp Neurol. 1955. 102: 425-509
27. Kelly R. Colloid cysts of the third ventricle; analysis of twenty-nine cases. Brain. 1951. 74: 23-65
28. Klein MR. Craniopharyngioma and tumor of the III ventricle: Exeresis of both tumors. Rev Neurol. 1994. 76: 21-
29. Little JR, MacCarty CS. Colloid cysts of the third ventricle. J Neurosurg. 1974. 40: 230-5
30. Mathiesen T, Grane P, Lindgren L, Lindquist C. Third ventricle colloid cysts: A consecutive 12-year series. J Neurosurg. 1997. 86: 5-12
31. Matsushima T, Fukui M, Kitamura K, Soejima T, Ohta M, Okano H. Mixed colloid cyst-xanthogranuloma of the third ventricle. A light and electron microscopic study. Surg Neurol. 1985. 24: 457-62
32. Nader-Sepahi A, Hamlyn PJ. Familial colloid cysts of the third ventricle: Case report. Neurosurgery. 2000. 46: 751-3
33. Partington MW, Bookalil AJ. Familial colloid cysts of the third ventricle. Clin Genet. 2004. 66: 473-5
34. Pollock BE, Huston J. Natural history of asymptomatic colloid cysts of the third ventricle. J Neurosurg. 1999. 91: 364-9
35. Romani R, Niemelä M, Korja M, Hernesniemi JA. Dizygotic twins with a colloid cyst of the third ventricle: Case report. Neurosurgery. 2008. 63: E1003-
36. Ryder JW, Kleinschmidt-DeMasters BK, Keller TS. Sudden deterioration and death in patients with benign tumors of the third ventricle area. J Neurosurg. 1986. 64: 216-23
37. Sadeghi S, Sharifi G, Aliasgari A. Familial colloid cyst of the third ventricle: A case report and review of the literature. Med J Islam Repub Iran. 2003. 17: 267-9
38. Salaud C, Hamel O, Buffenoir-Billet K, Nguyen JP. Familial colloid cyst of the third ventricle: Case report and review of the literature. Neurochirurgie. 2013. 59: 81-4
39. Shahhal I, Dayes LA. A case of arteriovenous malformation of the third ventricle: A clinical presentation and special features. Bull Clin Neurosci. 1984. 49: 13-22
40. Shuangshoti S, Netsky MG, Switter DJ. Combined congenital vascular anomalies and neuroepithelial (colloid) cysts. Neurology. 1978. 28: 552-5
41. Shuangshoti S, Roberts MP, Netsky MG. Neuroepithelial (colloid) cysts: Pathogenesis and relation to choroid plexus and ependyma. Arch Pathol. 1965. 80: 214-24
42. Sjovall E. Uber eine Ependymcyste embryonalen characters (paraphyse.) im dritten Hirnventrikel met todlichem Ausgang?. Beitr Pathol Anat. 1910. 47: 248-69
43. Socin HV, Born J, Wallemacq C, Betea D, Legros JJ, Beckers A. Familial colloid cyst of the third ventricle: Neuroendocrinological follow-up and review of the literature. Clin Neurol Neurosurg. 2002. 104: 367-70
44. Stoodley MA, Nguyen TP, Robbins P. Familial fatal and near-fatal third ventricle colloid cysts. Aust N Z J Surg. 1999. 69: 733-6
45. Tsuchida T, Hruban RH, Carson BS, Phillips PC. Colloid cysts of the third ventricle: Immunohistochemical evidence for nonneuroepithelial differentiation. Hum Pathol. 1992. 23: 811-6
46. Vandertop WP, Gosselaar PH, Nesselrooij B. Three sisters with colloid cyst of third ventricle. Lancet. 1995. 346: 643-4
47. Vandertop WP. Familial colloid cyst of the third ventricle: Case report and review of associated conditions. Neurosurgery. 1996. 39: 421-
48. Wallman H. Eine Colloidcyste im dritten Hirnventrikel und ein Lipom in Plexes Choroides. Virchous Arch. 1858. 11: 385-8
49. Wu W, Cogan JD, Pfäffle RW, Dasen JS, Frisch H, O’Connell SM. Mutations in PROP1 cause familial combined pituitary hormone deficiency. Nat Genet. 1998. 18: 147-9
50. Yüceer N, Baskaya M, Gökalp HZ. Huge colloid cyst of the third ventricle associated with calcification in the cyst wall. Neurosurg Rev. 1996. 19: 131-3
51. Zygmunt-Górska A, Starzyk J, Adamek D, Radwanska E, Sucharski P, Herman-Sucharska I. Pituitary enlargement in patients with PROP1 gene inactivating mutation represents cystic hyperplasia of the intermediate pituitary lobe. Histopathology and over 10 years follow-up of two patients. J Pediatr Endocrinol Metab. 2009. 22: 653-60

