Neurovascular compression syndromes (NVCs) are cranial nerve syndromes caused by direct contact or compression of vascular structures on the cranial nerves at the root exit/entry zone. Cases of combined NVCs are extremely rare.
Case
We reported the first case of a 41-year-old woman with combined four NVCs presenting with left hemifacial spasm followed by simultaneous left glossopharyngeal neuralgia, left type-writer tinnitus and vestibular paroxysmia due to the left posterior inferior cerebellar artery compression at the root exit/entry of the left facial, vestibulocochlear and glossopharyngeal nerves. All the symptoms resolved immediately after microvascular decompression without recurrence in a period of follow-up for one year. In addition, we presented a literature review of combined three or more NVCs.
Conclusion
We discussed the hypothesis of combined three or more NVCs development, especially the central hyperactivity of the cranial nerve nuclei mechanism.
Hinweise
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abkürzungen
CN VII
Facial nerve
CN VIII
Vestibulocochlear nerve
CN IX
Glossopharyngeal nerve
GPN
Glossopharyngeal neuralgia
HFS
Hemifacial spasm
IQR
Interquartile range
MRI
Magnetic resonance imaging
NVCs
Neurovascular compression syndromes
PICA
Posterior inferior cerebellar artery
TN
Trigeminal neuralgia
VP
Vestibular paroxysmia
Background
Neurovascular compression syndromes (NVCs) are cranial nerve syndromes caused by direct contact or compression of vascular structures on the cisternal portion of the cranial nerves at the root exit/entry zone. These lead to a variety of paroxysmal neurological hyperactivity dysfunction syndromes of the cranial nerves, such as trigeminal neuralgia (TN), hemifacial spasm (HFS), vestibular paroxysmia (VP), and glossopharyngeal neuralgia (GPN). In contrast to NVCs of a single cranial nerve which has a prevalence ranged from 0.2 to 10 per 100,000 people depending on the affected nerve (0.2–0.7, 0.77, and 5–10 per 100,000 people for GN, HFS, and TN, respectively) [1, 2], the prevalence of combined NVCs is much lower. A study among 1472 Japanese NVCs patients reported that 2.8% had combined NVCs, all with two cranial nerves involvement [3]. A study among 1,450 Chinese NVCs patients also showed a similar proportion of those with combined NVCs (3%), with those with combined three NVCs accounting for 0.1% of all NVCs patients [4]. In the rarity of combined NVCs cases, we described the first case report with combined four NVCs: HFS, VP, type-writer tinnitus, and GPN. In addition, all published cases presenting with combined three or more NVCs were reviewed and the role of hyperactivity of the cranial nerve nuclei in the pathophysiology of combined NVCs was reconsidered.
Case report
A previously healthy 41-year-old Thai female officer presented to a neurology clinic at a provincial hospital due to paroxysmal jerky movement of her left facial muscles for 3 years. Her symptoms initially started from the left lower eyelid before spreading to the upper and lower face. The duration of each jerky movement was approximately 30 s with an interval ranged from 5 to 10 min, which was compatible with typical HFS. A regular botulinum toxin injection at the affected facial muscle was performed. After one year of partial improvement, her HFS symptom began to deteriorate with more severe spasm and longer duration in each episode. In concordance, she simultaneously developed three new spontaneous paroxysmal symptoms: a sharp pain in her left ear canal, which was electrical shock-like and was aggravated by yawning, compatible with GPN; a “tik-tik” sound-like tinnitus or the ‘type-writer tinnitus’, and non-positional related vertiginous symptoms or VP. These three symptoms occurred and resolved simultaneously with HFS. All symptoms had a duration ranged from 1 to 2 min and an interval of approximately 15 min. Carbamazepine 400 mg/day was prescribed with partial improvement, but was discontinued due to drowsiness. After discontinuing carbamazepine, all symptoms reappeared. Botulinum toxin injection was reinitiated with partial improvement in only HFS. Other symptoms remained persistent. She was then referred to King Chulalongkorn Memorial Hospital. Physical examination revealed intermittent muscle contractions at her left lower face. The contraction of the left eyelid muscles was not observed, most likely due to the effect of botulinum toxin injection. Auditory, vestibular, and bulbar functions as well as facial sensation were preserved. Other neurological examinations were unremarkable.
Anzeige
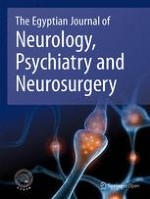
MRI of the brain demonstrated a distortion along the course of the left facial (CN VII), left vestibulocochlear (CN VIII), and left glossopharyngeal nerves (CN IX) due to compressions at the root exit/entry zone by a tortuous left posterior inferior cerebellar artery (PICA) in a perpendicular fashion to all three nerves (Fig. 1). The diagnosis was concurrent left HFS, VP, type-writer tinnitus, and GPN due to neurovascular compressions. Using the standard suboccipital approach, compressions at the root exit/entry zone of the left CN VII, CN VIII, and CN IX by the tortuous left PICA loop were confirmed. No arachnoiditis around the cranial nerves was identified. Microsurgical dissection was performed to separate the affected nerves from the PICA loop before placing Teflon between the nerves and the artery as a shock absorber. There were no postoperative complications. All symptoms resolved immediately after the surgery without recurrence of the symptoms in the follow-up period of one year.
Fig. 1
Axial 3D-FIESTA MRI of the brain. A, B At the level of medulla, left PICA (red line) crossing left CN IX (yellow line) was demonstrated; and C, D at the level of caudal pons, left PICA (red line) attaching the root exit zone of left CN VII (yellow line) and the root entry zone of left CN VIII (green line) was demonstrated
×
Discussion
We presented a patient with combined four NVCs caused by compression of CN VII, VIII, and IX due to a tortuous PICA. Our patient had started with a typical HFS followed by simultaneous GPN, type-writer tinnitus, and VP. Neuroimaging fulfilled the diagnostic criteria for NVCs of all affected cranial nerves [2, 5, 6]. The intraoperative findings demonstrated definite compressions. All symptoms resolved promptly after microvascular decompression and did not recur, verifying the causal relationship between neurovascular compression and the patient’s clinical syndromes.
Combined NVCs have been rarely reported, particularly those with three or more cranial nerves involvement. To our knowledge, our patient is the first case report of combined four NVCs. Searching the MEDLINE database for combined three or more NVCs, a total of 11 published cases were identified (Table 1) [1, 4, 7‐9]. All the cases had combined three NVCs. The majority were female (7/11), were from Asian reports (9/11), with a median (IQR) age at presentation of 65 (56–69) years. The common clinical manifestations included TN, HFS, and GPN caused by the tortuosity or dolichoectasia of arteries in the vertebrobasilar system [1, 4, 8]. Most patients (8/11) had combined NVCs confining to the same side: four were on the right, two were on the left, and two were ipsilateral unknown side. The median interval timing between the first and second syndromes was 3 (2–4) years. Nearly half of the patients (5/11) developed the second and third syndromes simultaneously. Immediate and simultaneous resolution of the combined symptoms after microvascular decompression was detected in nearly half of the patients (5/11).
Table 1
Eleven published cases of combined neurovascular compression syndromes with three or more cranial nerves involvement
The single classical NVCs are usually caused by a close contact or compression of normal vascular structure in the posterior cranial fossa to the cranial nerve which is susceptible to pulsatile impulse. A potential factor contributing to the development of combined NVCs is the tortuosity or dolichoectasia of arteries in the vertebrobasilar system and this is concordance to our case report and our review mentioned above [3, 4]. In addition, a small or crowded posterior fossa, as demonstrated from the MRI volumetric study which was proposed to be another potential factor for the development of single NVCs, such as HFS syndrome [10], may also contribute to the development of combined NVCs.
Anzeige
NVCs are caused by vascular compression at the root exit/entry zone of cranial nerves located near the transitional zone where the myelin sheath changes its origin from oligodendrocyte (central nervous system) to Schwann cell (peripheral nervous system). The accepted pathophysiology of these syndromes is based on the mechanism of spontaneous impulse generation and ephaptic transmission due to the demyelinating cranial nerve as a result of neurovascular compression. In addition, a role of the central hyperactivity of the cranial nerve nuclei resulting in hyperactivity dysfunction syndromes of the cranial nerves was also proposed [11]. Previous neurophysiologic studies included: (1) F wave and blink reflex studies among HFS patients [12, 13]; (2) nociceptive blink reflex and pain-related evoked potential studies among TN patients [14]; and (3) audiovestibular functions among VP patients [15]. All of these studies revealed the presence of hyperactivity of related cranial nerve nuclei in these NVCs. These evidences supported that the brainstem nuclei hyperactivity might also play a role in the pathophysiology of NVCs.
From the perspective view of the natural history of the combined NVCs in our analysis, most patients with combined NVCs started with one initial syndrome for 2- to 4-year period before developing additional cranial nerve syndromes which frequently occurred simultaneously (Table 1). Our hypothesis for simultaneous combined NVCs is as follow: an initial ectopic excitation and ephaptic transmission occurred from neurovascular compression of the firstly affected cranial nerve may initiate a hyperactivity of the first cranial nerve nucleus as well as the nearby cranial nerve nuclei, consequently leading to a simultaneous or sequential central hyperactivity of the cranial nerve nuclei and combined NVCs. Clinical evidences supporting the role of central hyperactivity of the cranial nerve nuclei were also documented from previous case reports. Idriceanu et al. reported painful spasms in facial, masticatory and motor ocular muscles caused by the PICA loop compression at the brainstem which reversed by microvascular decompression [16], and Warren et al. reported a case of simultaneously combined TN and GPN-like syndromes secondary to ipsilateral lateral medullary infarction [17].
Conclusions
Combined NVCs, particularly more than three syndromes, are rare and have never been documented. We reported a first case of combined four NVCs caused by a tortuous PICA loop. The potential factors for combined NVCs are the tortuosity or dolichoectasia of arteries in the vertebrobasilar system and the small area of posterior cranial fossa. The analysis of reported cases in this communication revealed an interesting natural history of combined NVCs which began with one syndrome followed by simultaneous combined syndromes. The simultaneous combined syndromes may underlaid by the role of the cranial nerve nuclei hyperactivity in the development of these syndromes. The established mechanism of NVCs is peripheral spontaneous impulse generation and ephaptic transmission of the compressed and demyelinated cranial nerve. Nevertheless, the possibility of the central hyperactivity of the cranial nerve nuclei should be considered especially in the setting of combined NVCs. Further research including neurophysiologic and clinical studies is needed to confirm this hypothesis.
Acknowledgements
We would like to express our gratitude to the patient for providing clinical information and giving informed consent to publish this report.
Declarations
Ethics approval and consent to participate
Not applicable.
Consent for publication
The patients in this case report gave written informed consent to publish the data contained.
Competing interests
All authors declared no competing interests.
Open AccessThis article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Eine ältere Frau trinkt regelmäßig Sennesblättertee gegen ihre Verstopfung. Der scheint plötzlich gut zu wirken. Auf Durchfall und Erbrechen folgt allerdings eine Hyponatriämie. Nach deren Korrektur kommt es plötzlich zu progredienten Kognitions- und Verhaltensstörungen.
Mit einem Neurotrophin-Rezeptor-Modulator lässt sich möglicherweise eine bestehende Alzheimerdemenz etwas abschwächen: Erste Phase-2-Daten deuten auf einen verbesserten Synapsenschutz.
Ein hohes soziales Niveau ist mit die beste Versicherung gegen eine Demenz. Noch geringer ist das Demenzrisiko für Menschen, die sozial aufsteigen: Sie gewinnen fast zwei demenzfreie Lebensjahre. Umgekehrt steigt die Demenzgefahr beim sozialen Abstieg.
Kommt es zu einer nichttraumatischen Hirnblutung, spielt es keine große Rolle, ob die Betroffenen zuvor direkt wirksame orale Antikoagulanzien oder Marcumar bekommen haben: Die Prognose ist ähnlich schlecht.
Update Neurologie
Bestellen Sie unseren Fach-Newsletterund bleiben Sie gut informiert.