Gayet–Wernicke's encephalopathy (GWE) is a life-threatening neurological emergency caused by vitamin B1 deficiency. This is a rare complication, which may be reversible if managed promptly. However, any diagnostic or therapeutic delay exposes to the risk of serious sequelae. Although this pathology frequently occurs in chronic alcohol users, it can also occur in any situation of severe undernutrition. In this context, we report a case of GWE occurring after severe undernutrition complicating prolonged catatonia in a patient suffering from schizophrenia.
Case presentation
He was a 47-year-old patient, suffering from esophageal stenosis, and followed in psychiatry for schizophrenia, who was hospitalized for a catatonic relapse. He was put on benzodiazepine with parenteral rehydration. Faced with the persistence of food refusal, and the appearance of signs of undernutrition, a parenteral diet was introduced. The evolution was marked by the deterioration of his general and neurological condition, with the appearance of mental confusion. The examination showed a central vestibular syndrome, and brain magnetic resonance imaging showed a hyperintense signaling in the periaqueductal area, in mammillary bodies, and in medial thalamic nuclei on T2-FLAIR sequences. GWE was suspected and parental vitamin B1 therapy was initiated. Laboratory testing confirmed the diagnosis, showing a low thiamine blood level of 32 nmol/l [normal range: 78 to 185 nmol/l]. Regression of neurological symptoms was observed within 2 weeks of treatment.
Conclusion
Through this illustration, we draw the attention of the psychiatrist, who must think about preventing this complication, by supplementing any patient at risk of developing GWE with vitamin B1.
Hinweise
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abkürzungen
GWE
Gayet–Wernicke's encephalopathy
MRI
Magnetic resonance imaging
Background
Gayet–Wernicke encephalopathy (GWE) is a life-threatening neurological emergency caused by vitamin B1 (thiamine) deficiency, which affects the peripheral and central nervous systems. It is a rare complication, which can be reversible if it is quickly managed [1]. However, diagnostic or therapeutic delay is associated with serious consequences in terms of mortality (20% of cases) and morbidity, with the risk of serious and disabling neurological sequelae such as Korsakoff's syndrome [1, 2].
Although this pathology mostly affects chronic alcohol users, it can also occur in several other situations causing severe undernutrition (chronic vomiting, prolonged fasting, prolonged parenteral nutrition, liver diseases, exclusive artificial feeding…) [1].
Anzeige
Psychiatric disorders, a class of complex disorders characterized by brain dysfunction with varying degrees of impairment in cognition, emotion, consciousness and behavior [3], are known to be frequently associated with undernutrition. Schizophrenia is one of these chronic devastating neurodevelopmental disorders, in which patients abnormally interpret reality and suffer from and extremely disordered thinking and behavior [4, 5]. Positive symptoms, including hallucinations and delusions, are common in these patients, as are negative symptoms such as apathy, emotionlessness and lack of social functioning [6]. Cognitive impairments are also frequently reported, including deficits in attention, executive functions such as response inhibition and working memory, verbal learning and memory, and social memory [4, 6‐9].
Literature suggests that a person’s risk of developing the illness is increased by a mix of physical, genetic, psychological, and environmental variables (a bio-psycho-social model) [6]. In particular, gene–environment interactions played an important role in its pathogenesis [3].
Several studies highlighted the incrimination of neurobiological factors in the pathogenesis of schizophrenia, just like a wide range of other psychiatric and neurodegenerative disorders [5, 10]. For example, mitochondrial functions are observed to be compromised and to become less resilient under continuous stress [10]. Meanwhile, stress and inflammation have been linked to the activation of the tryptophan (Trp)–kynurenine (KYN) metabolic pathway, which observably contributes to the development of pathological conditions including cancer, immune diseases, neurodegenerative diseases and psychiatric disorders [4, 10]. Previous studies showed that the KYN system is activated in schizophrenia and elevated KYN levels are considered to contribute to the cognitive impairments of schizophrenia [4, 5].
Furthermore, recent studies showed a linkage between schizophrenia-associated chromosomal loci and inflammatory markers such as pro-inflammatory cytokine gene polymorphisms, major histocompatibility complex and Toll-like receptors [5].
Anzeige
Also, neurocognitive dysfunction in patients with schizophrenia has been associated to vitamin D deficiency which may directly affect processing speed [7].
Functional neuroimaging data showed several abnormalities in brain areas, such disruption in prefrontal cortex [9], and corpus callosum (CC) white matter tracts deficits which are associated with cognitive impairments [3, 11].
Schizophrenia is associated to a wide range of somatic comorbidities, such as cardiovascular disease, diabetes, as well as smoking and alcoholism-related diseases. Besides, patients with mental disorders, like schizophrenia, are known to have increased risk of malnutrition, yet physical examinations and nutritional assessments are not routinely performed and followed up mental health professionals [12].
In this context, we report a case of GWE following severe undernutrition, complicating prolonged catatonia in a patient with schizophrenia.
He was a 47-year-old patient, followed in psychiatry since the age of 28 for schizophrenia, with several catatonic relapses. Before his admission, he was taking olanzapine (10 mg/day) and chlorpromazine (100 mg/day) with a poor treatment compliance. He had stopped his treatment 4 months before his admission. The patient also suffered from an esophageal stenosis complicating caustic ingestion occurring 8 months ago. There was no neurological history.
Symptoms and complaints of the current episode
Two months before his hospitalization, the patient became isolated, no longer communicating with his relatives and refused to eat and to take his treatment. Thus, he was hospitalized in a psychiatric department.
Medical and psychiatric examination during the hospitalization
When he was admitted, his eye contact was absent, and he was sub-mute. He was motionless, with maintenance of body position and waxy flexibility. He was opponent, refusing the examiner outstretched hand and the execution of simple orders. In addition, he refused to eat and to take the oral treatment. The medical examination showed a low blood pressure (10/06 mmHg) and a sinus tachycardia (103 b/min). He was breathing at 19 breaths/min, and had a normal oxygen saturation (96%). The neurological examination was normal.
The initial biological explorations were normal.
Anzeige
In light of this catatonic syndrome, the patient was initiated on benzodiazepine (lorazepam) with parenteral rehydration. Faced with the persistence of food refusal 1 week after admission, and the appearance of undernutrition symptoms, a parenteral nutrition was administrated.
The evolution was marked by the deterioration of his general and neurological condition.
Apart from the weight loss (4 kg in 3 weeks), his skin became dry, his bones protruded, and he became cachectic.
A mental confusion appeared, with a temporo-spatial disorientation, anxious perplexity and terrifying visual hallucinations.
Anzeige
Neurological examination showed central vestibular syndrome (ataxia and bilateral multidirectional nystagmus).
Data of the neuroimaging
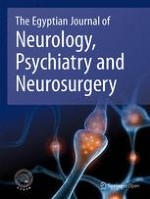
Brain magnetic resonance imaging (MRI) showed a hyperintense signaling in the periaqueductal area, in mammillary bodies, and in medial thalamic nuclei on T2-FLAIR sequences (Fig. 1).
Fig. 1
Brain magnetic resonance imaging (T2-FLAIR sequences). Axial sections on T2-FLAIR sequences showing hyperintense signaling in the periaqueductal area (A, B), in mammillary bodies (B) and in medial thalamic nuclei (C)
×
Therapeutic intervention
GWE was suspected and parenteral vitamin B1 supplementation (500 mg*3/day) was urgently started. Laboratory testing confirmed the diagnosis, showing a low thiamine blood level of 32 nmol/l [normal range: 78 to 185 nmol/l].
Improvement of neurological symptoms was observed within 2 weeks of treatment. An atypical antipsychotic (olanzapine 5 mg/day) was then administrated. Partial remission of psychiatric symptoms was noted within 3 weeks.
Anzeige
Comments
GWE is an acute neurological emergency caused by vitamin B1 deficiency. It is often underdiagnosed, especially in cases with a non-alcohol related etiologies [2], as was the case of our patient. However, its occurrence in these patients is far from exceptional [2]. Mostly reported in patients with a long-standing history of alcohol abuse, this condition can occur in any situation of severe undernutrition (prolonged fasting; diseases of the gastrointestinal tract, anorexia nervosa, prolonged parenteral diet without vitamin supplementation …) [1, 2].
For our patient with schizophrenia, the catatonia caused prolonged dietary restriction, even before his hospitalization. Afterwards, thiamine depletion was aggravated by prolonged parenteral feeding without vitamin supplementation.
While GWE is a well-characterized syndrome in alcoholism and malnutrition, there are limited numbers of reports about this neurological disorder occurring with psychiatric illnesses [13, 14].
Psychiatric disorders can be accompanied by substantial dietary restrictions, because of the fear of gaining weight in anorexia nervosa, losing interest in food in depression, and food-related delusions or hallucinations in schizophrenia [14, 15]. These poor dietary habits, malnutrition, as well as high prevalence of alcoholism, predispose them to thiamine deficiency so that they can develop a GWE [13, 14]. Unfortunately, Wernicke’s symptoms may be overlooked or obscured by the psychiatric illness.
The commonest recognized psychiatric cause of GWE is anorexia nervosa, an eating disorder characterized by a restriction of dietary intake leading to significantly low weight, intense fear of gaining weight, and disturbance in the way one’s own body is experienced [16].
Further, a number of studies have shown an inverse association between thiamine levels and depressive symptoms. Poor intake of food, a common symptom in depression, can lead to thiamine deficiency and exposes to the risk of GWE [17].
Patients with schizophrenia seem to be also at a greater risk for GWE. According to a recent systematic review [18], GWE following schizophrenia has seldom been reported in the literature. This neurological condition is known to be under-recognized, and the vast majority of cases are missed during life. It is unknown the burden of GWE in patients with schizophrenia, but a review of the neuropathology literature suggests that some of these patients demonstrate periventricular gliosis postmortem, thought due to Wernicke’s disease [13].
Several hypotheses have been described to explain the co-occurrence of GWE and schizophrenia.
First, the predisposition of patients with schizophrenia to develop GWE seems to be explained by neurobiological mechanisms. Prior studies pointed out that patients with schizophrenia have an altered glucose metabolism with an abnormal accumulation of lactic acid, possibly increasing the chance to develop a GWE [19]. Similarly, in isotopic dilution studies, a defect in the metabolism of carbohydrates in schizophrenia has been found [18, 20]
The second explanation would be the high frequency of alcohol use in these patients; GWE thus complicates chronic alcoholism among them [13, 21].
Another hypothesis is related to nutritional problems in patients with schizophrenia. These problems are common, due to homelessness, poor self-care, inability to prepare foods, poor dietary habits and an unhealthy lifestyle [13, 18, 22]. In this population, 40.3% of patients have been estimated to be at risk for malnourishment. [13, 21, 23]. These disturbances are partly related to the negative symptoms of schizophrenia, associated with a behavior of isolation, social withdrawal and poor diet leading to nutritional deficiency [24].
Dietary restriction can also be secondary to an active food refusal which may be seen in several situations. For example, this behavior may be underpinned by delusions of poisoning or bewitchment, or a hallucinatory behavior (food-related command hallucinations) [18, 21]. In addition, food refusal can be a depressive symptom (post-psychotic depression, depressive symptoms of a schizoaffective disorder…) or a catatonic behavior [25], as was the case of our patient.
According to a recent systematic review published in 2021 [18], and focusing on case reports of patients with schizophrenia having developed GWE, 15 cases have been already published [13, 21, 24, 26‐37]. This complication occurred in a delusional context in 8 cases [27‐30, 32, 35‐37]; in a hallucinatory context for a case [21] and after vomiting in 2 cases [31, 34]. Besides, two other cases have been recently reported [14, 16]. The first one illustrated a case of GWE caused by food refusal in a woman with schizophrenia [14]. The second one reported a case of GWE caused by mental anorexia in a man with schizophrenia [16]. In the previous literature review [18], only one case [27] suffered from schizophrenia with catatonia, although the occurrence of GWE was attributed to a delusional behavior. Thus, to the best of our knowledge, this is the first case reporting GWE directly linked to a catatonic state.
GWE is typically characterized by a classic clinical triad of confusion, oculomotor disorders (nystagmus, ophthalmoplegia …) and ataxia, which was the case of our patient [1, 38]. However, this triad is noted in only 16 to 38% of patients, and the diagnosis should be suspected in the presence of any unexplained neurological symptom in an undernourished patient [1, 38].
As the clinical triad is non-specific and often incomplete, the use of additional examinations is necessary to confirm the diagnosis. Biological explorations (measurement of erythrocyte transketolase activity or the concentration of serum thiamine pyrophosphate) are not routinely done [1]. Neuroimaging may be particularly important for confirming the diagnosis. Brain MRI remains the investigation of choice because of its high specificity [39]. It shows hyperintensities on T2, FLAIR, and diffusion sequences, in the periaqueductal area, around the third ventricle, in the postero-medial thalamic nuclei and in mammillary bodies [1].
GWE is a therapeutic emergency [1]. Early identification and immediate intervention are crucial to improving patient outcomes. Even if diagnosis is not yet confirmed, it is advised that clinicians initiate interventions in suspected cases. The most consensus guideline is that of the National Institute of Health and Clinical Excellence (NICE) [40], which recommends the administration of intravenous thiamine (500 mg every 8 h), for 5 days, combined with multivitamins and hydro-electrolyte disorders correction. If symptoms improve, this treatment is continued (250 mg/day) for 3 to 5 days (or until full remission) [2].
The early therapeutic response reflects the improvement of biochemical events rather than structural lesions [41]. The recovery begins with the oculomotor disorders improvement within a few hours or days. On the other hand, ataxia and cognitive impairment can persist for a long time or even for life [1]. MRI abnormalities will subside with clinical improvement [41].
Conclusion
Through this illustration, we have shed light on one of the most feared somatic complications in patients with mental disorders, following prolonged undernutrition. GWE is a diagnostic and therapeutic emergency, which is life-threatening unless immediate intervention. Owing to the high rate of mortality and morbidity, it should be considered in the evaluation of any patient with unexplained confusion or other neurological symptoms, especially if there is a context of malnutrition. This is particularly important in psychiatric patients where the clinical history and syndrome may be obscured, and treatment delayed. For patients with schizophrenia, and considering that they are at considerable risk of malnutrition, it is recommended to inquire about eating habits regularly during check-ups. If nutritional deficiency is suspected, the threshold to suspect GWE in these patients should be lowered and in doubt, prophylactic thiamine supplementation may prevent the precipitation or exacerbation of a GWE. Therefore, it is recommended that psychiatrists remain vigilant about such an association with mental health disorders, especially schizophrenia or eating disorders. They should regularly screen for high-risk patients, and think to prevent GWE by a routine vitamin B1 supplementation.
Acknowledgements
Not applicable.
Machines used in the study
* Magnetic resonance imaging: SIMENS MAGNETOM Essenza 1.5T, made in Germany.
* Thiamine level determination in whole blood was performed at Cerba laboratory (France), using High Performance Liquid Chromatography (HPLC) (EDTA tube).
Declarations
Ethics approval and consent to participate
Expedited ethics approval was obtained from the Committee for the Protection of Persons of the University of Sfax, Tunisia (reference “CPP SUD N°0468/2022”, January 5, 2023).
Consent for publication
Informed written consent was obtained from the participant for publication of this case and accompanying images.
Competing interests
The authors declare that they have no competing interests.
Open AccessThis article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Eine ältere Frau trinkt regelmäßig Sennesblättertee gegen ihre Verstopfung. Der scheint plötzlich gut zu wirken. Auf Durchfall und Erbrechen folgt allerdings eine Hyponatriämie. Nach deren Korrektur kommt es plötzlich zu progredienten Kognitions- und Verhaltensstörungen.
Mit einem Neurotrophin-Rezeptor-Modulator lässt sich möglicherweise eine bestehende Alzheimerdemenz etwas abschwächen: Erste Phase-2-Daten deuten auf einen verbesserten Synapsenschutz.
Ein hohes soziales Niveau ist mit die beste Versicherung gegen eine Demenz. Noch geringer ist das Demenzrisiko für Menschen, die sozial aufsteigen: Sie gewinnen fast zwei demenzfreie Lebensjahre. Umgekehrt steigt die Demenzgefahr beim sozialen Abstieg.
Kommt es zu einer nichttraumatischen Hirnblutung, spielt es keine große Rolle, ob die Betroffenen zuvor direkt wirksame orale Antikoagulanzien oder Marcumar bekommen haben: Die Prognose ist ähnlich schlecht.
Update Neurologie
Bestellen Sie unseren Fach-Newsletterund bleiben Sie gut informiert.