


Abstract
Background: It is estimated that one-quarter to half of all hospital waste is produced in the operating room. Recycling of surgical waste in the perioperative setting is uncommon, even though there are many recyclable materials. The objective of this study was to determine the amount of waste produced in the preoperative and operative periods for several orthopedic subspecialties and to assess how much of this waste was recycled.
Methods: Surgical cases at 1 adult and 1 pediatric tertiary care hospital in Calgary, Alberta, were prospectively chosen from 6 orthopedic subspecialties over a 1-month period. Waste was collected, weighed and divided into recyclable and nonrecyclable categories in the preoperative period and into recyclable, nonrecyclable, linen and biological categories in the intraoperative period. Waste bags were weighed using a portable hand-held scale. The primary outcome was the amount of recyclable waste produced per case. Secondary outcomes included the amount of nonrecyclable, biological and total waste produced. An analysis of variance was performed to test for statistically significant differences among subspecialties.
Results: This study included 55 procedures. A total of 341.0 kg of waste was collected, with a mean mass of 6.2 kg per case. Arthroplasty produced a greater amount of recyclable waste per case in the preoperative (2017.1 g) and intraoperative (938.6 g) periods as well as total recyclable waste per case, resulting in a greater ratio of waste recycling per case then nearly all other subspecialties in the preoperative (86%) and intraoperative (14%) periods. Arthroplasty similarly produced a greater amount of nonrecyclable waste per case (5823.6 g) than the other subspecialties, most of which was produced during the intraoperative period (5512.9 g). Overall an average of 27% of waste was recycled per case.
Conclusion: Among orthopedic subspecialties, arthroplasty is one of the largest waste producers and it has the highest potential for recycling of materials. Effective recycling programs in the operating room can reduce our ecological footprint by diverting waste from landfills, as our study revealed that nearly three-quarters of this waste is recyclable.
Hospitals produce substantial waste, which is damaging to the environment. In the United States alone, they generate an estimated 3 million tons of solid waste per year.1 Hospital operating facilities are a major source of waste production because of the high-output nature of resource-intensive procedures. It is estimated that one-quarter to half of all hospital waste is produced in the operating room (OR),1,2 a substantial portion of which is produced in the preoperative period, as instruments and tools are often individually wrapped in sterile packaging.3
Opportunities to recycle surgical waste in the perioperative setting are commonly missed, despite the fact that it is possible to safely and easily recycle many of the materials being discarded.4 Several barriers to widespread adoption of recycling programs in the OR include costly initiation and processing fees, concerns about safety related to increased waste handling, and perceptions about decreased OR efficiency. As a result, variability exists globally, from minimal recycling in the United Kingdom to widespread recycling in Australia.4
Total hip and knee arthroplasty procedures in particular are thought to be a substantial source of waste production; however, other orthopedic procedures are not immune to this phenomenon.2 As patient-specific and modular implants become increasingly popular, the amount of waste produced will probably increase. Given the growing concerns about waste production and its effects on the environment, recycling programs have become increasingly common in tertiary care hospitals in the Calgary health region. These programs divide surgical waste into several streams, including recyclables, nonrecyclables and biological waste.
The primary objective of this study was to assess the effect of the recently introduced ecofriendly policies by determining the amount of waste and recycling material produced in the preoperative and operative time periods for several orthopedic subspecialties. We hypothesized that arthroplasty surgery produces the greatest amount of waste. Additionally, we believed that a substantial proportion of the preoperative waste generated by all orthopedic subspecialties has the potential to be recycled.
Methods
Surgical cases were prospectively chosen and assigned to an orthopedic subspecialty category: trauma, arthroplasty, sports, foot and ankle, upper extremity and pediatrics. We aimed to choose 5–10 cases for each category that were thought to be representative of that subspecialty. Data were collected over a 1-month period from to November 2017 from an adult tertiary care hospital (South Health Campus) and a pediatric tertiary care hospital (Alberta Children’s Hospital) with established recycling programs in place. In these centres, OR staff manually separated waste into different waste streams by depositing each article into the appropriate receptacle. Data could not be collected for polytrauma or oncology cases, as these patients were treated at a level 1 trauma centre that did not have an OR recycling program.
The preoperative phase began with the opening of the surgical case carts and concluded with the end of skin preparation. The intraoperative period began after skin preparation was complete and concluded after the OR was cleaned. At the end of the preoperative period all surgical waste was weighed and divided into recyclable and nonrecyclable waste streams. Following the intraoperative period, surgical waste was divided into recyclable, nonrecyclable, linen and biological waste streams. Recyclables included noncontaminated plastics, cardboards and various wrapping materials. Nonrecyclables included contaminated and soiled waste products, including surgical gloves and noncloth gowns. Biological waste, which included human remains such as soft tissue and boney resections, was collected separately in our institution and, as such, for the purposes of data collection it was considered a separate waste stream. All waste bags were weighed in a standardized fashion using a portable Samsonite hand-held scale accurate to 10 g (model 613381041). All waste streams were then disposed of in an appropriate manner as per the regional health protocol. Sharps were excluded from measurement.
The primary outcome was the amount of recyclable waste produced per case for each orthopedic subspecialty in the preoperative, intraoperative and postoperative periods. Secondary outcomes were the amount of non-recyclable, biological and total waste produced during the same time periods. Data for each waste stream were collected on a predeveloped spreadsheet. Statistical analysis was completed with SPSS using descriptive statistics where appropriate and using 1-way analysis of variance with Tukey post hoc testing to detect differences among subspecialties. Significance was defined as p less than 0.05. This study was deemed exempt from the need for ethics review as it did not involve any human or animal subjects and was classified as a quality-improvement project.
Results
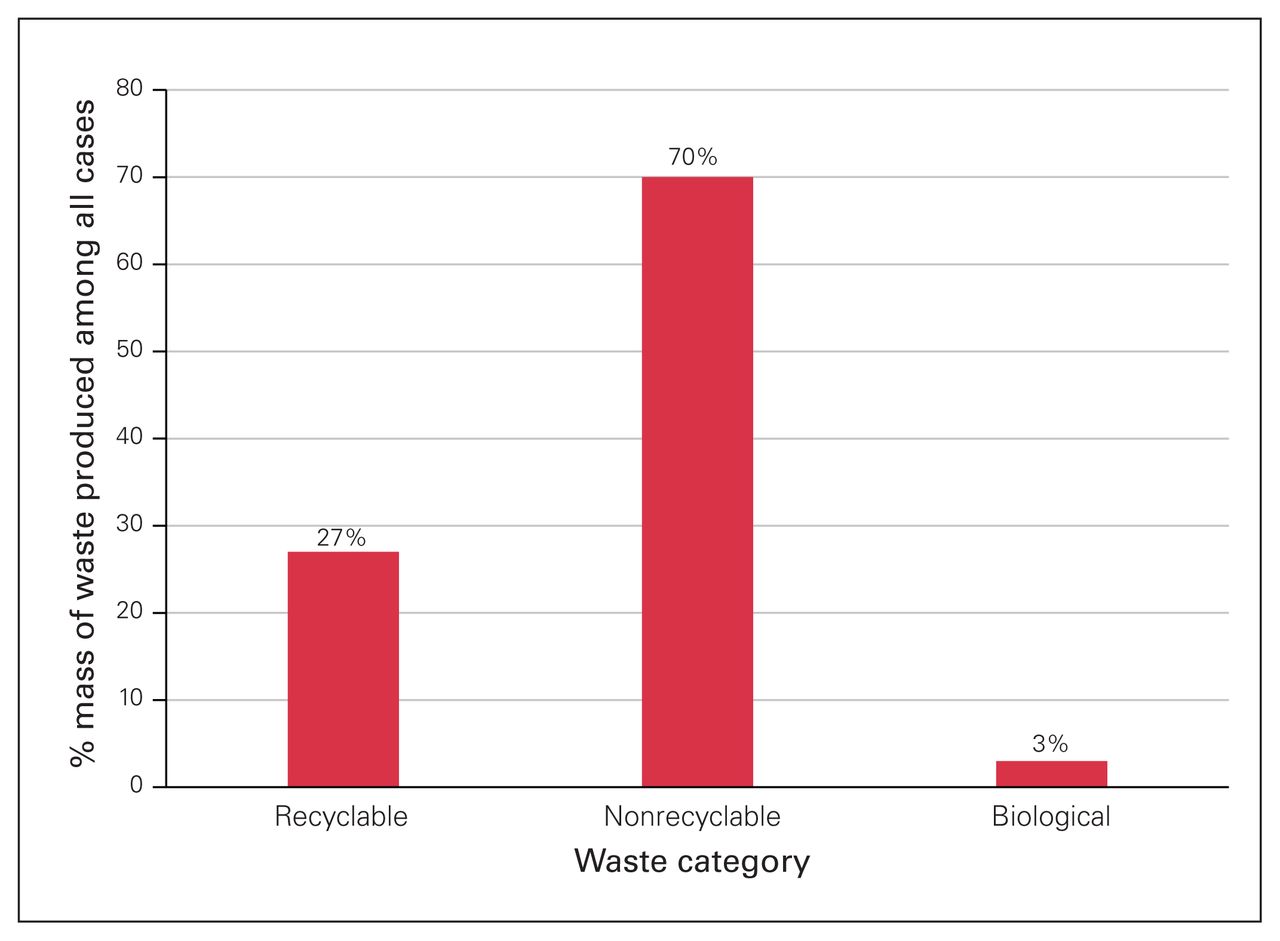
This study included 55 procedures over the 1-month study period. A total of 341.0 kg of waste was collected, with a mean mass of 6.2 kg per case. A total of 93.4 kg of waste was recyclable (1.70 kg per case), 239.1 kg was nonrecyclable (4.35 kg per case) and biological waste amounted to 8.5 kg (0.2 kg per case) (Fig. 1). Substantially more surgical waste was produced in the intraoperative period than in the preoperative period (236.8 kg v. 95.7 kg, respectively). In the preoperative period an average of 74% of waste was recyclable, compared with 8% of waste produced during the intraoperative period (Fig. 2). In total, the average percentage of waste that was recycled per case was 27%.

Percent mass of waste produced among all cases in the recyclable, nonrecyclable and biological waste categories.

Percent mass of recyclable and nonrecyclable waste produced among all cases in the preoperative and intraoperative periods.
In terms of the primary outcome, arthroplasty surgery produced substantially more recyclable waste per case in the preoperative (2017.1 g) and intraoperative (938.6 g) periods than the other subspecialties (Fig. 3). It also produced the greatest percentage of total recyclable waste per case, resulting in a substantially greater ratio of waste recycling per case than nearly all other subspecialties in the preoperative (86%) and intraoperative (14%) periods (Fig. 4).

Mean mass of recyclable waste per case in the preoperative and intraoperative periods, by subspecialty. *p < 0.05.

Percent mass of recyclable waste per case in the preoperative and intraoperative periods, by subspecialty. *p < 0.05.
In terms of the secondary outcomes, arthroplasty surgery similarly produced substantially more nonrecyclable waste per case than all other subspecialties (5823.6 g), most of which was produced during the intraoperative period (5512.9 g) (Fig. 5). Arthroplasty surgery also produced substantially more biological waste per case than all other subspecialties (409.3 g) (Table 1).

Mean mass of nonrecyclable waste in the preoperative and intraoperative periods, by subspecialty. *p < 0.05.
Mean mass of waste per case
Discussion
The primary objective of this study was to assess the amount of waste and recycling produced in the preoperative and intraoperative time periods for several orthopedic subspecialties. Our hypothesis was confirmed, as arthroplasty surgery produced more surgical waste per case than all other subspecialties. However, arthroplasty also produced the most recyclable, nonrecyclable and biological waste per case. Additionally, arthroplasty also recycled a proportionally larger percentage of waste per case (33.5%) than all other subspecialties except pediatrics (42.6%). There was a disproportionally large percentage of recyclable waste produced in the preoperative period. In the preoperative period an average of 74% of waste was recyclable, compared with 8% of waste produced during the intraoperative period. This trend was consistent among all subspecialties.
This study demonstrates that there is great potential for reducing our environmental impact in the preoperative period by promoting ecologically sound practices and waste management protocols. Currently, preoperative waste is primarily handled by nurses and OR staff. With a simple education program, OR staff can easily be trained to correctly identify and dispose of recyclable waste streams. This was demonstrated by Lui and colleagues in 2014 in an otolaryngology waste study: they showed that a single education session, in conjunction with informative wall posters, was effective in promoting preoperative waste recycling. In that study, 89.7% of all preoperative waste was recycled.3 This waste stream is free from contamination, which makes it viable for recycling and safe for handling by untrained staff members, without affecting patient care.
Arthroplasty surgery is a substantial contributor to waste production. The reasons for this are probably multifactorial and related to the large number of equipment sets needed and their associated wrapping waste. Additionally, at our institution, personal protective equipment for arthroplasty surgeries included additional equipment such as sterile arthroplasty helmets, the wearing of which is not standard practice in other orthopedic subspecialties. Finally, these procedures often require 2 assists, and as many as 6 procedures may be completed by a single surgeon during an OR day. Stall and colleagues demonstrated many of these concepts through the use of a surgical audit for total knee arthroplasty.5 They similarly found that arthroplasty surgery resulted in a substantial amount of waste production. Most of the waste was solid waste, biological waste and blue sterile wrap. Only 2.2% of their surgical waste was recyclable. The discrepancy in results between our studies can probably be attributed to differences in recycling practices, as all plastic wrappers and sterile blue wrap at our institution were recycled, and surgical gowns were often reusable Gore-Tex materials. Nonetheless, it is clear that arthroplasty surgery has a greater ecological footprint than the other orthopedic subspecialties. Fortunately, our study also shows that there is the potential for substantial landfill diversion when recycling initiatives are established in arthroplasty. An estimated 7 000 000 orthopedic procedures are completed each year in the United States, 700 000 of which are total hip or knee replacement surgeries.6,7 If we extrapolate our data to these results, similar recycling programs could potentially divert more than 11 564 000 kg of waste from landfills each year, with more than 2 000 000 kg of waste from arthroplasty alone.
Strengths of this study include the fact that, to our knowledge, this is the first study to compare the waste production of different orthopedic subspecialties and the first orthopedic study to break down waste production in the preoperative and intraoperative periods. We hope these data can guide the development of recycling programs and ecologically sustainable OR practices in the future, especially for resource-intensive surgeries and subspecialties.
Limitations
Some weaknesses of our study include the small number of procedures in several subspecialties, particularly in pediatrics, as well as our inability to capture oncologic and polytrauma cases. In our study, pediatric surgery was second only to arthroplasty in waste production, and it recycled a greater percentage of its waste than any other subspecialty in our study. These results are contrary to those of Lui and colleagues, as their study demonstrated that pediatric ear, nose and throat procedures produced proportionally less recyclable material than the other subspecialties. 3 Upon review of our pediatric cases, we discovered there was a disproportionally large number of pediatric spinal deformity cases. These complex cases typically have longer set-up times and thus produce a greater amount of waste, which could potentially explain this discrepancy. Unfortunately, we were not able to include data on polytrauma and oncology cases because there was not an established recycling program at the level 1 trauma centre in which these surgeries took place. Given our current data, both of these subspecialties would probably produce equivalent or greater amounts of waste and have greater potential for recycling than all the orthopedic subspecialties included in our study. Additionally, waste collection was not supervised, and as such, it is possible that cross-contamination took place.
Conclusion
From this study, we can confirm that orthopedic surgery is a substantial source of waste production in our hospital system. Among orthopedic subspecialties, arthroplasty is one of the largest waste producers, but it also has the highest potential for recycling of materials. Effective OR recycling programs can substantially reduce our ecological footprint by diverting waste from landfills. In particular, the preoperative period has substantial potential for landfill diversion as our study showed that nearly three-quarters of all waste in this period can be effectively recycled. We hope to capitalize on these results by expanding recycling opportunities in the OR throughout our health region.
Acknowledgement
The authors of this study were supported by a COREF research grant from the University of Calgary’s McCaig Institute for Bone and Joint Health.
Footnotes
Competing interests: None declared.
Contributors: S. Kooner, J. Lui and M. Clark designed the study. S. Kooner, C. Hewison and S. Sridharan acquired the data, which S. Kooner, J. Lui, G. Matthewson, H. Johal and M. Clark analyzed. S. Kooner, G. Matthewson and H. Johal wrote the article, which all authors critically reviewed. All authors provided final approval of the article to be published.
- Accepted October 10, 2019.
In this issue

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Article tools






Related Articles
Cited By...
- No citing articles found.