
Topical Pirfenidone-Loaded Liposomes Ophthalmic Formulation Reduces Haze Development after Corneal Alkali Burn in Mice


 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Preparation of PFD-Loaded Liposomes Formulation
2.2. Characterization of PFD-Loaded Liposomes Formulation
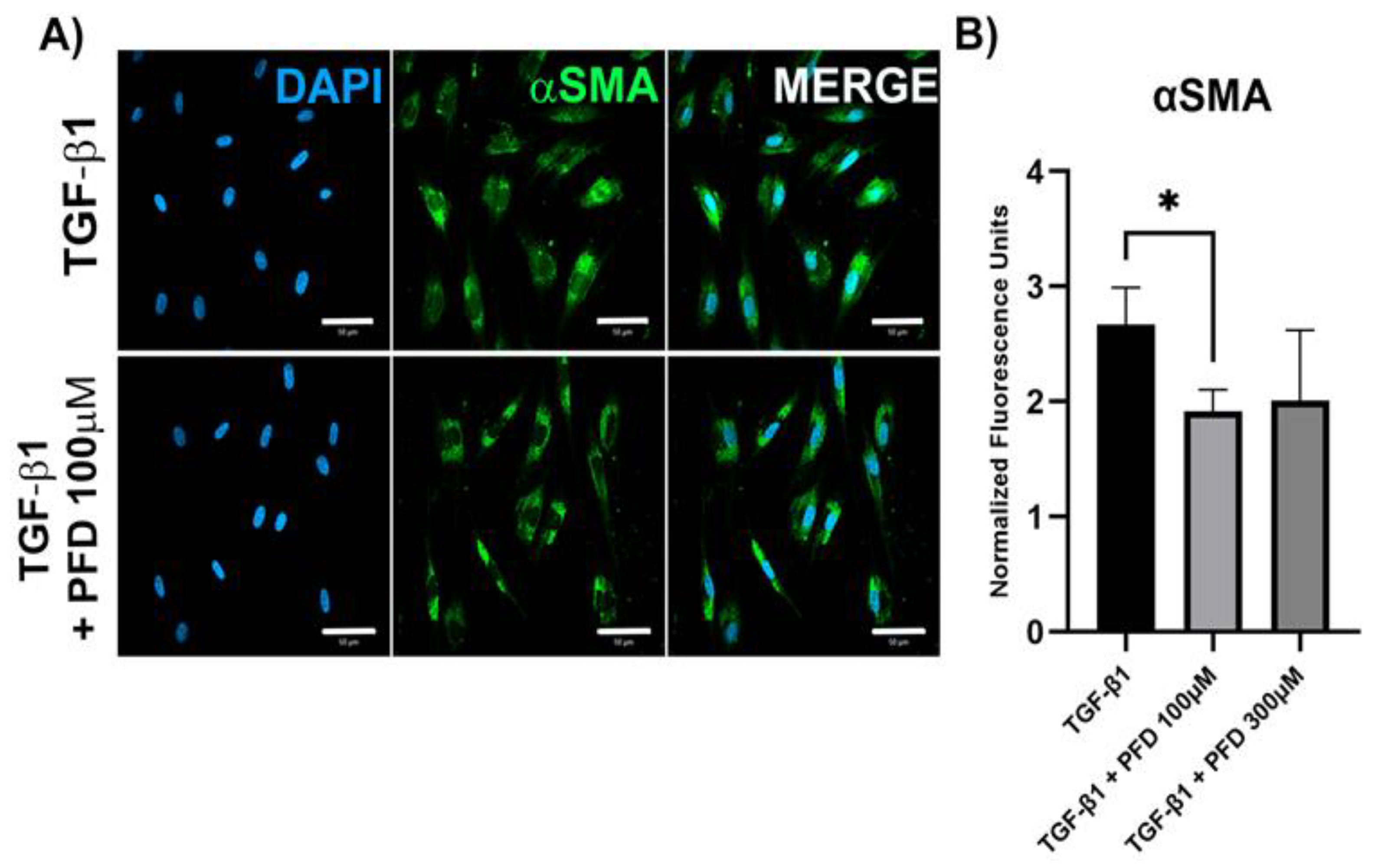
2.3. Evaluation of the Antifibrotic Activity of PFD in Human Corneal Fibroblasts (HCFs)
2.4. Evaluation of the Therapeutic Activity of PFD in a Mice Mode of Corneal Alkali Burn
2.5. Statistical Analysis
2.6. Ethical Considerations
3. Results
3.1. PFD Is Efficiently Loaded in Liposomes and It Is Suitable for Topical Ophthalmic Use
3.2. PFD Reduces Expression of Pro-Fibrogenic Genes in HCF Primary Cell Culture
3.3. PFD Reduces Corneal Haze, Inflammation and Edema after Alkali Burn
3.4. PFD and PFD-Loaded Liposomes Suppress αSMA Expression in Corneal Tissue
3.5. PFD and PFD-Loaded Liposomes Suppress TGF-β Expression in Corneal Tissue and Restores Normal IL-1β Expression
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Barrientez, B.; Nicholas, S.E.; Whelchel, A.; Sharif, R.; Hjortdal, J.; Karamichos, D. Corneal Injury: Clinical and Molecular Aspects. Exp. Eye Res. 2019, 186, 107709. [Google Scholar] [CrossRef]
- Sharma, N.; Kaur, M.; Agarwal, T.; Sangwan, V.S.; Vajpayee, R.B. Treatment of acute ocular chemical burns. Surv. Ophthalmol. 2018, 63, 214–235. [Google Scholar] [CrossRef]
- Bizrah, M.; Yusuf, A.; Ahmad, S. An update on chemical eye burns. Eye 2019, 33, 1362. [Google Scholar] [CrossRef]
- Torricelli, A.A.M.; Santhanam, A.; Wu, J.; Singh, V.; Wilson, S.E. The corneal fibrosis response to epithelial-stromal injury. Exp. Eye Res. 2016, 142, 110. [Google Scholar] [CrossRef] [Green Version]
- Eslani, M.; Baradaran-Rafii, A.; Movahedan, A.; Djalilian, A.R. The Ocular Surface Chemical Burns. J. Ophthalmol. 2014, 2014, 196827. [Google Scholar] [CrossRef] [Green Version]
- Hamill, C.E.; Bozorg, S.; Peggy Chang, H.Y.; Lee, H.; Sayegh, R.R.; Shukla, A.N.; Chodosh, J. Corneal alkali burns: A review of the literature and proposed protocol for evaluation and treatment. Int. Ophthalmol. Clin. 2013, 53, 185–194. [Google Scholar] [CrossRef]
- Zahir-Jouzdani, F.; Soleimani, M.; Mahbod, M.; Mottaghitalab, F.; Vakhshite, F.; Arefian, E.; Shahhoseini, S.; Dinarvand, R.; Atyabi, F. Corneal chemical burn treatment through a delivery system consisting of TGF-β1 siRNA: In vitro and in vivo. Drug Deliv. Transl. Res. 2018, 8, 1127–1138. [Google Scholar] [CrossRef]
- Kaji, Y.; Soya, K.; Amano, S.; Oshika, T.; Yamashita, H. Relation between corneal haze and transforming growth factor-β1 after photorefractive keratectomy and laser in situ keratomileusis. J. Cataract Refract. Surg. 2001, 27, 1840–1846. [Google Scholar] [CrossRef]
- Ljubimov, A.V.; Saghizadeh, M. Progress in corneal wound healing. Prog. Retin. Eye Res. 2015, 49, 17. [Google Scholar] [CrossRef] [Green Version]
- Roy, K.; Cheung, C.H.A.; Kanwar, R.K.; Sandhir, R.; Kanwar, J.R. Topical ophthalmic formulation of trichostatin A and SurR9-C84A for quick recovery post-alkali burn of corneal haze. Front. Pharmacol. 2017, 8, 223. [Google Scholar] [CrossRef]
- Joung, C.; Noh, H.; Jung, J.; Song, H.Y.; Bae, H.; Pahk, K.; Kim, W.K. A Novel CD147 Inhibitor, SP-8356, Attenuates Pathological Fibrosis in Alkali-Burned Rat Cornea. Int. J. Mol. Sci. 2020, 21, 2990. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zahir-Jouzdani, F.; Khonsari, F.; Soleimani, M.; Mahbod, M.; Arefian, E.; Heydari, M.; Shahhosseini, S.; Dinarvand, R.; Atyabi, F. Nanostructured lipid carriers containing rapamycin for prevention of corneal fibroblasts proliferation and haze propagation after burn injuries: In vitro and in vivo. J. Cell. Physiol. 2019, 234, 4702–4712. [Google Scholar] [CrossRef]
- Jiang, N.; Ma, M.; Li, Y.; Su, T.; Zhou, X.Z.; Ye, L.; Yuan, Q.; Zhu, P.; Min, Y.; Shi, W.; et al. The role of pirfenidone in alkali burn rat cornea. Int. Immunopharmacol. 2018, 64, 78–85. [Google Scholar] [CrossRef]
- Shimizu, T.; Kuroda, T.; Hata, S.; Fukagawa, M.; Margolin, S.B.; Kurokawa, K. Pirfenidone improves renal function and fibrosis in the post-obstructed kidney. Kidney Int. 1998, 54, 99–109. [Google Scholar] [CrossRef] [Green Version]
- García, L.; Hernández, I.; Sandoval, A.; Salazar, A.; Garcia, J.; Vera, J.; Grijalva, G.; Muriel, P.; Margolin, S.; Armendariz-Borunda, J. Pirfenidone effectively reverses experimental liver fibrosis. J. Hepatol. 2002, 37, 797–805. [Google Scholar] [CrossRef]
- Hirano, A.; Kanehiro, A.; Ono, K.; Ito, W.; Yoshida, A.; Okada, C.; Nakashima, H.; Tanimoto, Y.; Kataoka, M.; Gelfand, E.W.; et al. Pirfenidone Modulates Airway Responsiveness, Inflammation, and Remodeling after Repeated Challenge. Am. J. Respir. Cell Mol. Biol. 2006, 35, 366. [Google Scholar] [CrossRef]
- Lopez-de la Mora, D.A.; Sanchez-Roque, C.; Montoya-Buelna, M.; Sanchez-Enriquez, S.; Lucano-Landeros, S.; Macias-Barragan, J.; Armendariz-Borunda, J. Role and New Insights of Pirfenidone in Fibrotic Diseases. Int. J. Med. Sci. 2015, 12, 840. [Google Scholar] [CrossRef] [Green Version]
- Sun, G.; Lin, X.; Zhong, H.; Yang, Y.; Qiu, X.; Ye, C.; Wu, K.; Yu, M. Pharmacokinetics of pirfenidone after topical administration in rabbit eye. Mol. Vis. 2011, 17, 2191–2196. [Google Scholar]
- Yang, M.; Yang, Y.F.; Lei, M.; Ye, C.T.; Zhao, C.S.; Xu, J.G.; Wu, K.L.; Yu, M. Bin Preparation and evaluation of HPMC-based pirfenidone solution in vivo. Drug Dev. Ind. Pharm. 2016, 43, 171–176. [Google Scholar] [CrossRef]
- Chowdhury, S.; Guha, R.; Trivedi, R.; Kompella, U.B.; Konar, A.; Hazra, S. Pirfenidone Nanoparticles Improve Corneal Wound Healing and Prevent Scarring Following Alkali Burn. PLoS ONE 2013, 8, e70528. [Google Scholar] [CrossRef] [Green Version]
- López-Cano, J.J.; González-Cela-Casamayor, M.A.; Andrés-Guerrero, V.; Herrero-Vanrell, R.; Molina-Martínez, I.T. Liposomes as vehicles for topical ophthalmic drug delivery and ocular surface protection. Expert Opin. Drug Deliv. 2021, 18, 819–847. [Google Scholar] [CrossRef] [PubMed]
- Navarro-partida, J.; Castro-castaneda, C.R.; Cruz-pavlovich, F.J.S.; Aceves-franco, L.A.; Guy, T.O.; Santos, A. Lipid-Based Nanocarriers as Topical Drug Delivery Systems for Intraocular Diseases. Pharmaceutics 2021, 13, 678. [Google Scholar] [CrossRef] [PubMed]
- Altamirano-Vallejo, J.C.; Navarro-Partida, J.; Gonzalez-De La Rosa, A.; Hsiao, J.H.; Olguín-Gutierrez, J.S.; Gonzalez-Villegas, A.C.; Keller, B.C.; Bouzo-Lopez, L.; Santos, A. Characterization and pharmacokinetics of triamcinolone acetonide-loaded liposomes topical formulations for vitreoretinal drug delivery. J. Ocul. Pharmacol. Ther. 2018, 34, 416–425. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Partida, J.; Altamirano-Vallejo, J.C.; Lopez-Naranjo, E.J.; Gonzalez-De La Rosa, A.; Manzano-Ramírez, A.; Apatiga-Castro, L.M.; Armendáriz-Borunda, J.; Santos, A. Topical Triamcinolone Acetonide-Loaded Liposomes as Primary Therapy for Macular Edema Secondary to Branch Retinal Vein Occlusion: A Pilot Study. J. Ocul. Pharmacol. Ther. 2020, 36, 393–403. [Google Scholar] [CrossRef]
- Purslow, C.; Wolffsohn, J.S. Ocular surface temperature: A review. Eye Contact Lens 2005, 31, 117–123. [Google Scholar] [CrossRef]
- Guo, X.; Hutcheon, A.E.K.; Melotti, S.A.; Zieske, J.D.; Trinkaus-Randall, V.; Ruberti, J.W. Morphologic Characterization of Organized Extracellular Matrix Deposition by Ascorbic Acid–Stimulated Human Corneal Fibroblasts. Investig. Ophthalmol. Vis. Sci. 2007, 48, 4050–4060. [Google Scholar] [CrossRef]
- Livak, K.J.; Schmittgen, T.D. Analysis of relative gene expression data using real-time quantitative PCR and the 2− ΔΔCT method. Methods 2001, 25, 402–408. [Google Scholar] [CrossRef]
- Yuan, J.S.; Reed, A.; Chen, F.; Stewart, C.N. Statistical analysis of real-time PCR data. BMC Bioinform. 2006, 7, 85. [Google Scholar] [CrossRef] [Green Version]
- Rabinovich-Guilatt, L.; Couvreur, P.; Lambert, G.; Dubernet, C. Cationic Vectors in Ocular Drug Delivery. J. Drug Target. 2008, 12, 623–633. [Google Scholar] [CrossRef]
- Awwad, S.; Mohamed Ahmed, A.H.A.; Sharma, G.; Heng, J.S.; Khaw, P.T.; Brocchini, S.; Lockwood, A. Principles of pharmacology in the eye. Br. J. Pharmacol. 2017, 174, 4205. [Google Scholar] [CrossRef]
- Baranowski, P.; Karolewicz, B.; Gajda, M.; Pluta, J. Ophthalmic drug dosage forms: Characterisation and research methods. Sci. World J. 2014, 2014, 861904. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soleimani, M.; Naderan, M. Management Strategies of Ocular Chemical Burns: Current Perspectives. Clin. Ophthalmol. 2020, 14, 2687. [Google Scholar] [CrossRef] [PubMed]
- Hassell, J.R.; Birk, D.E. The Molecular Basis of Corneal Transparency. Exp. Eye Res. 2010, 91, 326. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hinz, B. Myofibroblasts. Exp. Eye Res. 2015, 142, 56–70. [Google Scholar] [CrossRef]
- McKay, T.B.; Hutcheon, A.E.K.; Zieske, J.D. Biology of corneal fibrosis: Soluble mediators, integrins, and extracellular vesicles. Eye 2020, 34, 271. [Google Scholar] [CrossRef]
- Wilson, S.E. Corneal myofibroblasts and fibrosis. Exp. Eye Res. 2020, 201, 108272. [Google Scholar] [CrossRef]
- Zhong, H.; Sun, G.; Lin, X.; Wu, K.; Yu, M. Evaluation of Pirfenidone as a New Postoperative Antiscarring Agent in Experimental Glaucoma Surgery. Investig. Ophthalmol. Vis. Sci. 2011, 52, 3136–3142. [Google Scholar] [CrossRef] [Green Version]
- Jung, K.I.; Park, C.K. Pirfenidone inhibits fibrosis in foreign body reaction after glaucoma drainage device implantation. Drug Des. Devel. Ther. 2016, 10, 1477–1488. [Google Scholar]
- Westermeyer, H.D.; Salmon, B.; Baynes, R.; Yeatts, J.; Khattab, A.; Oh, A.; Mowat, F. Safety and efficacy of topically applied 0.5% and 1% pirfenidone in a canine model of subconjunctival fibrosis. Vet. Ophthalmol. 2019, 22, 502–509. [Google Scholar] [CrossRef]
- Bao, Y.; Huang, L.; Huang, X.; Gao, C.; Chen, Y.; Wu, L.; Zhu, S.; Song, Y. Pirfenidone ameliorates the formation of choroidal neovascularization in mice. Mol. Med. Rep. 2020, 21, 2162–2170. [Google Scholar] [CrossRef] [Green Version]
- Wilson, S.E.; Mohan, R.R.; Mohan, R.R.; Ambro, R.; Hong, J.; Lee, J. The Corneal Wound Healing Response: Cytokine-mediated Interaction of the Epithelium, Stroma, and Inflammatory Cells. Prog. Retin. Eye Res. 2001, 20, 625–637. [Google Scholar] [CrossRef]
- Wilson, S.E.; Esposito, A. Interleukin-1: A master regulator of the corneal response to injury. Exp. Eye Res. 2009, 89, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mishra, G.P.; Bagui, M.; Tamboli, V.; Mitra, A.K. Recent Applications of Liposomes in Ophthalmic Drug Delivery. J. Drug Deliv. 2011, 2011, 863734. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reagent | Volume |
|---|---|
| Pirfenidone | 1 or 0.2 mg |
| Kolliphor HS 15 | 50 mg |
| Polyethylene Glycol (PEG)-12 glyceryl dimyristate | 100 mg |
| Ethyl alcohol | 14 µL |
| Citric acid anhydrous | 0.8 mg |
| Sodium citrate dihydrate | 4.675 mg |
| Benzalkonium chloride | 0.1 mg |
| Grade 2 purified water | Q.S.1.0 mL |
| Formulation | pH | Viscosity (mPa·s) | Osmolarity (mmol/kg) | Diluted PL (1/200 v/v) | Size (d.nm) | PdI | ζ (mV) |
|---|---|---|---|---|---|---|---|
| PL 0.1% | 5.72 | 32.9 | 103.38 ± 10.15 | PL 0.1% (PBS) | 263 ± 10 | 0.37 ± 0.04 | −20.4 ± 0.2 |
| PL 0.02% | 6.06 | 42.2 | 101.47 ± 9.16 | PL 0.02% (PBS) | 214 ± 2.8 | 0.29 ± 0.03 | −20.9 ± 0.7 |
| PL 0.1 (ddH2O) | 256 ± 2.6 | 0.28 ± 0.01 | −26.6 ± 0.7 | ||||
| PL 0.02% (ddH2O) | 253 ± 5.0 | 0.35 ± 0.01 | −19.4 ± 0.9 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaz-Palomera, C.D.; Vidal-Paredes, I.A.; Navarro-Partida, J.; Cid-Hernandez, M.; Rosales-Rivera, L.C.; De la Rosa-Bibiano, R.; Monroy-Ramirez, H.C.; Santos, A.; Armendariz-Borunda, J. Topical Pirfenidone-Loaded Liposomes Ophthalmic Formulation Reduces Haze Development after Corneal Alkali Burn in Mice. Pharmaceutics 2022, 14, 316. https://doi.org/10.3390/pharmaceutics14020316
Diaz-Palomera CD, Vidal-Paredes IA, Navarro-Partida J, Cid-Hernandez M, Rosales-Rivera LC, De la Rosa-Bibiano R, Monroy-Ramirez HC, Santos A, Armendariz-Borunda J. Topical Pirfenidone-Loaded Liposomes Ophthalmic Formulation Reduces Haze Development after Corneal Alkali Burn in Mice. Pharmaceutics. 2022; 14(2):316. https://doi.org/10.3390/pharmaceutics14020316
Chicago/Turabian StyleDiaz-Palomera, Carlos Daniel, Isaac Alejandro Vidal-Paredes, Jose Navarro-Partida, Margarita Cid-Hernandez, Luis Carlos Rosales-Rivera, Ricardo De la Rosa-Bibiano, Hugo Christian Monroy-Ramirez, Arturo Santos, and Juan Armendariz-Borunda. 2022. "Topical Pirfenidone-Loaded Liposomes Ophthalmic Formulation Reduces Haze Development after Corneal Alkali Burn in Mice" Pharmaceutics 14, no. 2: 316. https://doi.org/10.3390/pharmaceutics14020316