Despite being the cause of morbidity and mortality in many patients, little is known about the pathophysiology of cerebral small vessel disease (CSVD). Identifying new biomarkers is mandatory for early diagnosis and proper management. The aim of this study is to investigate the role of micro-RNA as a biomarker for incidental cerebral small vessel disease (iCSVD) and its clinic-radiological correlates in a sample of Egyptian patients.
Results
The median age of patients, gender and risk factors did not differ from controls. However, patients were more significantly impaired than controls on cognitive, gait and sphincteric scales. MiRNA-451a was upregulated in cases with a median fold change of 3.4, while miRNA-409-3p, 486-5p, 502-3p, were significantly downregulated in comparison to healthy controls.
Conclusion
Dysregulation of the studied microRNA may play a role in pathogenesis of incidental cerebral small vessel disease and warrants further studies.
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Abkürzungen
BBS
Berg Balance Scale Score
BDI
Beck Depression Inventory
BMET
Brief Memory and Executive Test
CMBs
Cerebral microbleeds
CNS
Central nervous system
CSVD
Cerebral small vessel disease
iCSVD
Incidental cerebral small vessel disease
EDTA
Ethylenediaminetetraacetic acid
EPVS
Enlarged perivascular spaces
ICIQ-SF
The Arabic International Consultation on Incontinence Questionnaire-Short Form Scale
MoCA
Montreal Cognitive Assessment Test
10MWT
10-Meter walk test
MRI
Magnetic resonance imaging
RNA
Ribonucleic acid
SVD
Small vessel disease
VaD
Vascular dementia
WMH
White matter hyperintensities
Introduction
Over the past few years, the prevalence, mortality, and morbidity of different neurological disorders have increased, despite the implementation of intervention programs aiming to reduce their health care burden [1]. This has incited the scientific community to explore reliable and affordable biomarkers for early detection of these disorders [2].
Incidental cerebral small vessel disease (iCSVD) is among the neurological diseases known to reduce the quality of life in elderly. It has a strong role in age-related disabilities as cognitive impairment, gait apraxia, urinary incontinence, and depression as well as being a leading cause of vascular dementia (VaD) [3‐5].
Anzeige
Diagnosis of iCSVD is based on brain imaging biomarkers, in the form of recent small subcortical infarcts, white matter hyperintensities (WMH), lacunes, cerebral microbleeds (CMBs), enlarged perivascular spaces (EPVS) and cerebral atrophy [6].
Recently there is an increasing body of evidence that miRNA plays a critical role in the control of key biological processes including development, differentiation, growth, and metabolism as well as pathophysiology of neurodegenerative and cardiovascular diseases [7]. Living neurons and other central nervous system (CNS) cells secrete miRNA and other small non-coding RNA into the extracellular space packaged in exosomes, micro-vesicles, or lipoprotein complexes [8].
In an interesting study, Prabhakar and colleagues in India, reported that four miRNAs (miR-409-3p, miR-502-3p, miR-486- 5p and miR-451a) could be used to differentiate iCSVD patients from healthy controls and might serve as diagnostic biomarkers for this disease [9]. However, to the best of our knowledge, no other studies have further investigated the role of these four miRNAs in patients with iCSVD among other populations or ethnic groups.
In a previous study, we reported that 63.7% of Egyptian patients with acute stroke are due to large artery disease, in addition to radiological evidence of CSVD [10]. Accordingly, we conducted this research to explore if any of the previously studied miRNAs could act as biomarkers for iCSVD in a sample of Egyptian patients. In addition to investigating if they have any clinical–radiological correlates.
Anzeige
Methods
This is an observational cross-sectional case-controlled study. It aims to compare the data of 30 patients with iCSVD to 30 age and sex matched healthy controls with regard to the prevalence of a set of miRNAs and their correlates with clinical and radiological data.
The study was approved by the ethical committee of the university and a written informed consent was obtained from patients or the first of kin to participate in the study. Patients were enrolled from outpatient clinics of the University Hospitals if their age was above 45 years, presenting with insidious onset of cognitive impairment, gait abnormalities or urinary incontinence and Magnetic Resonance Imaging (MRI) brain showing evidence of small vessel disease. Patients were excluded if they presented with or gave a history of acute stroke or showed carotid stenosis more than 50% on imaging. Cases were excluded also if they suffered from any other metabolic or neurological disease affecting white matter as sarcoidosis and multiple sclerosis. Healthy controls were included according to having no history of neurological, or any chronic metabolic disorders with a normal general and neurological examination. Vascular risk factors were not among the exclusion criteria for healthy controls.
All participants were subjected to comprehensive neurological assessment including history taking (past medical history, vascular risk factors, detailed history of current illness and drug history) and neurological examination. Cognitive assessment was done using Arabic version of Montreal Cognitive Assessment Test (MoCA) in which a maximum score of 30 denotes no cognitive affection while scoring ≤ 26 denotes more cognitive affection [11]. Gait assessment scores were compared between cases and controls and included: 10-m walk test (10MWT), self-selected velocity and fast velocity [12] and Berg Balance Scale (BBS) with highest possible score of 56 [13]. Arabic version of Beck Depression Inventory (BDI) [14] was used to assess depressive symptoms where a higher score indicates severer depression, with a maximum score of 63. Urinary problems were assessed using The Arabic International Consultation on Incontinence Questionnaire-Short Form (ICIQ-SF) Scale [15] with range 0–21 with higher grade denoting incontinence. MRI brain was performed using a 1.5T MR scanner (Achieva and Ingenia, Philips medical system, Eindhoven, Netherlands) for visual analysis of lesion burden of CSVD using Fazekas scale [16]. In addition, small vessel disease score (SVD) [17] was calculated by counting the presence of 4 MRI markers (white matter hyperintensities, lacunes, cerebral microbleeds, and perivascular spaces; ranging from 0–4). Also, brain atrophy was assessed using global cortical atrophy scale [18] which has a range 0–39 with higher grade signifying severe atrophy.
For miRNA analysis, venous blood samples collected using EDTA tubes were kept at − 80 degrees Celsius for later use. miRNA extraction was carried out on the stored plasma samples using simple miRNA extraction kit (Qiagen, Germany), according to the manufacturer's instructions. MiScript SYBR Green PCR kit (Qiagen, Germany) was used to perform quantitative PCR (qPCR) amplification of the extracted miRNAs in triplicates using the universal primer and miRNA-specific primers. The extracted miRNAs were reverse transcribed using the miScript II RT Kit (Eurofins, Belgium).
As a normalizer, a spike-in internal control (C. elegans miR-39 miRNA mimic, Qiagen, Germany) was employed, and each run's negative controls included using no template and negative RT reactions. In order to determine the specificity of the reactions, the initial denaturation stage of the reactions was conducted for 10 min at 92 °C, followed by 45 cycles of 95 °C for 15 s, 55 °C for 30 s, and 70 °C for 30 s followed by a high-resolution melt (HRM) analysis. The DTlite 4L thermal cycler (Russia) was used for temperature cycling.
Changes in the circulating levels of miRNAs were calculated by Livak analysis (2-ΔΔCt) method with fold change values more than 1.5 interpreted as up regulation and values less than or equal to 0.5 (2-fold reduction) were interpreted as downregulation. Patients’ fold change (RQ values) was calculated by normalizing the control (calibrators) data and calculating patients’ data accordingly [19].
Statistical analysis
Sample size was calculated using PASS 11, showing that sample of 60 subjects (30 patients and 30 control) would achieve 99% power analysis. Data analysis was done using IBM SPSS software package version 25.0 (Armonk, NY: IBM Corp). The normality test was done using Kolmogorov–Smirnov test. The Mann–Whitney U test was used with median, range and inter-quartile range (IQR), while qualitative data were described in frequency and percentage and was tested via Chi-square test. Point biserial correlation was used to evaluate the correlation between miRNA and different variables. The significance of the obtained results was judged at P < 0.05.
Results
This study involved 30 patients with iCSVD and 30 healthy controls. Both groups of cases and controls were age and sex matched with median age 61 years for cases and 61.5 years for controls. The male prevalence was 19 (63.3%) in cases and 18 (60%) in controls.
Anzeige
There was no significant difference among the 2 groups regarding the educational level with almost half of the subjects achieving 12–14 years of education. Additionally, there was no statistical difference between cases and controls regarding vascular risk factors.
The median (IQR) of the age of onset of symptoms in cases group was 65 (11) years old while the duration of illness was 2 (1) years.
Patients with iCSVD showed significant impairment of mood (p = 0.003), cognition, gait, and sphincteric control as compared to controls (p < 0.001) (Table 1).
Table 1
Comparative analysis between case and control regarding basic data, vascular risk factors and clinical scales
Group
Mann–Whitney U test/
Chi test^
Control
Case
Frequency/ median
%/IQR
Frequency/ median
%/IQR
z/ x^
P
Age
61
7
61.50
4
− 0.423
0.672
Gender (male)
18
60.0%
19
63.3%
0.071^
0.791
Education years
14
6
11
7
− 1.499
0.134
Education level
Read and write
6
20.0%
5
16.7%
5.550^
0.235
Primary
0
0.0%
4
13.3%
Preparatory
7
23.3%
9
30.0%
Secondary
9
30.0%
5
16.7%
University
8
26.7%
7
23.3%
Smoker
9
30.0%
6
20.0%
0.800^
0.371
DM
6
20.0%
10
33.3%
1.364^
0.243
Hypertension
15
50.0%
19
63.3%
1.086^
0.297
Dyslipidemia
7
23.3%
10
33.3%
0.739^
0.390
ISHD
3
10%
4
13.3%
0.162^
0.688
No. of vascular risk factor
0
9
30.0%
5
16.7%
4.218^
0.377
1
7
23.3%
9
30.0%
2
8
26.7%
5
16.7%
3
5
16.7%
7
23.3%
4
1
3.3%
4
13.3%
MoCA
28
1.25
18
6.50
− 6.694
< 0.001*
BDI (total score)
1.50
5
6
16
− 2.924
0.003*
BDI grades
No
30
100.0%
18
60.0%
15^
0.002*
Mild
0
0.0%
4
13.3%
Moderate
0
0.0%
7
23.3%
Severe
0
0.0%
1
3.3%
Berg Balance Score
56
0
35
19
− 6.881
< 0.001*
10MWT self-selected velocity
0.75
0.17
0.44
0.20
− 6.430
< 0.001*
10MWT fast velocity
0.85
0.20
0.55
0.28
− 6.198
< 0.001*
ICIQ-SF
0
0
2.50
7
− 4.377
< 0.001*
Bold values indicate significant values
DM diabetes mellitus, ISHD ischemic heart disease, MoCA Montreal Cognitive Assessment, BDI Beck Depression Inventory, 10MWT 10-meter walk test, ICIQ-SF The Arabic International Consultation on Incontinence Questionnaire-Short Form Scale, IQR inter-quartile range
^ Chi test was used
*p value is significant if < 0.05
The commonest presenting symptom was cognitive impairment representing 17 (56.7%) of cases followed by gait abnormality in 11 (36.7%), with only 2 patients were accidentally diagnosed due to vertigo or headache.
Anzeige
Regarding MRI brain, 93.3% had Fazekas scale grades 2 and 3. Also, the majority laid in SVD score 2 (50%) and 3 (33.3%). Global cortical atrophy scale had a range from 4–32 with a median (IQR) of 17 (9) and atherosclerosis was observed in all patients (Additional file 1: Table S1).
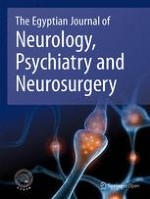
Regarding miRNA expression, cases with significant up- or down-regulation are shown in Fig. 1. It was noticed that 3 miRNAs (409-3p, 486-5p, 502-3p) were significantly downregulated with 90% of cases showing less than 0.5 (twofold reduction) regarding miRNA 409-3p and 486-5p and 80% of cases in miRNA 502-3p as compared to controls, while only one miRNA (451a) showed upregulation as 70% of cases had more than 1.5-fold change compared to controls.
Fig. 1
Box plot of study group’s miRNA fold change
×
There was significant correlation between dysregulated miRNA-486-5p with age and age of onset and negative correlation with duration of illness while dysregulated miRNA-451a showed negative correlation with SVD score as shown in Table 2.
Table 2
miRNA correlation with clinical and radiological characteristics
miRNA-451a
miRNA-486-5p
miRNA-502-3p
Age
Point biserial
− 0.0313
0.42*
0.152
Sig.
0.92
0.01
0.421
Age of onset
Point biserial
− 0.31
0.43*
0.134
Sig.
0.09
0.01
0.479
Duration of illness
Point biserial
0.16
− 0.39*
− 0.138
Sig.
0.41
0.03
0.466
MoCA
Point biserial
0.224
0.093
− 0.191
Sig.
0.233
0.62
0.310
BDI (total score)
Point biserial
0.006
− 0.159
0.053
Sig.
0.97
0.40
0.779
Berg Balance Score
Point biserial
− 0.089
0.012
− 0.193
Sig.
0.64
0.95
0.306
10MWT self-selected velocity
Point biserial
− 0.010
− 0.017
− 0.23
Sig.
0.96
0.93
0.212
ICIQ-SF
Point biserial
− 0.43
− 0.227
0.045
Sig.
0.86
0.226
0.811
SVD score
Point biserial
− 0.43
0.114
0.203
Sig.
0.012
0.55
0.279
Bold values indicate significant values
miRNA micro ribonucleic acid, MoCA Montreal Cognitive Assessment, BDI Beck Depression Inventory, 10MWT 10-meter walk test, ICIQ-SF The Arabic International Consultation on Incontinence Questionnaire-Short Form Scale, SVD small vessel disease
*p value is significant if < 0.05
Correlation with miRNA-409-3p could not be done due to statistical limitation
Discussion
The incidence of iCSVD was found to reach up to 6–10 times that of stroke [20], in addition it is the commonest underlying cause of vascular dementia [21]. The mainstay of management is to control vascular risk factors [22], and this warrants early diagnosis prior to development of permanent disability.
Anzeige
In this case-controlled study, 30 patients with iCSVD were recruited and assessed using clinical scales, MRI brain and blood sampling to detect the expression of four miRNAs as disease biomarkers.
In concordance with a previous study [23], we found no sex difference in iCSVD prevalence. Unexpectedly, there was no significant difference between both cases and control groups with regard to vascular risk factors, while in a recent systematic review and meta-analysis conducted in 2021, it was found that hypertension, diabetes, hyperlipidemia and smoking were significantly related to CSVD [24]. The possible differences between populations, as well as the variability of pathogenesis and presentation of iCSVD [25], are all considerable causes for this disparity of results, and this could point to the importance of further research among different populations with larger sample sizes.
Regarding the clinical scales, patients with iCSVD showed worse scores for depression and cognition, with slower gait speed and impaired sphincteric control than healthy controls. These findings were confirmed by other studies [26, 27].
The key finding of this study was the significant difference in expression of the studied miRNAs between cases and controls, with upregulation of miR-451a and downregulation of the rest (miR-409-3p, miR-486-5p and miR-502-3p). This indicates the potential role of dysregulated miRNA in the pathogenesis of iCSVD or the reciprocal effect of this disease on the homeostasis of certain miRNAs. This, however, still remains unclear and requires further studies in different populations.
These findings are partially in concordance with the previous study conducted in India yet (miR486-5p and miR-502-3p), which were upregulated unlike the results in the Egyptian sample [9]. This could be related to different genotypes of the disease or racial differences.
MicroRNAs usually regulate gene expression at a post-transcriptional level through multiple messenger RNAs (mRNAs) and functional proteins [28] and can therefore, modulate diverse biological processes, including cell differentiation, cell cycle, proliferation, apoptosis and cellular response to stress [29, 30].
MicroRNA was investigated in different CNS diseases as migraine [31] and amyotrophic lateral sclerosis [32], post-stroke cognitive impairment [33]. Moreover, it was employed to differentiate vascular from Alzheimer’s dementia [34]. And in 2017, Prabhakar and colleagues, reported 44 miRNAs that were differentially expressed in VaD patients compared to controls [9].
The neuroprotective role of miRNA in different neurological disorders was investigated thoroughly in a previously published review [35]. Cerebral ischemia in animal models was among the studied disorders where miRNA was reported to be dysregulated and to change following ischemic preconditioning. This suggests the important role of miRNA and its target proteins in cerebral ischemia and reperfusion [36, 37].
The finding that dysregulated miRNA had either positive or negative correlations with some clinical variables as age, age of onset and duration of illness; in addition to radiological biomarker represented by SVD score implies the sensitivity of miRNA to disease progression as well as the possible high yield for early diagnosis. This may be later confirmed by studying the same miRNA in patients at high risk of developing iCSVD and following up this group both clinically and radiologically to confirm such hypothesis [37].
These findings in addition to the few studies investigating the role of miRNA as a biomarker for iCSVD warrant further research on a larger scale with comparison of different races and populations, since this might offer an early diagnostic tool for iCSVD and consequently initiation of primary prevention before disability is established.
Conclusion
Incidental cerebral small vessel disease has no apparent age or sex predilection with huge impact upon quality of life by affecting cognition and gait. The possibility of early detection through the studied miRNAs before clinical manifestation would greatly help in preventive treatment either with the current available medications or by developing new ones that may alter the genetic pathway itself. However, more studies are needed in different populations.
Acknowledgements
Science and Technology Development Fund.
Declarations
Ethics approval and consent to participate
All procedures performed in the study were in accordance with the ethical standards of the faculty of medicine, Ain Shams university research and ethical committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. We obtained approval from research ethics committee FWA 000017585 in 2020. Written informed consent was obtained from participants for participation. We obtained approval from research ethics committee no. FWA 000017585 in 2020.
Consent for publication
Not applicable.
Competing interests
None of the authors has any conflict of interest.
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Eine ältere Frau trinkt regelmäßig Sennesblättertee gegen ihre Verstopfung. Der scheint plötzlich gut zu wirken. Auf Durchfall und Erbrechen folgt allerdings eine Hyponatriämie. Nach deren Korrektur kommt es plötzlich zu progredienten Kognitions- und Verhaltensstörungen.
Mit einem Neurotrophin-Rezeptor-Modulator lässt sich möglicherweise eine bestehende Alzheimerdemenz etwas abschwächen: Erste Phase-2-Daten deuten auf einen verbesserten Synapsenschutz.
Ein hohes soziales Niveau ist mit die beste Versicherung gegen eine Demenz. Noch geringer ist das Demenzrisiko für Menschen, die sozial aufsteigen: Sie gewinnen fast zwei demenzfreie Lebensjahre. Umgekehrt steigt die Demenzgefahr beim sozialen Abstieg.
Kommt es zu einer nichttraumatischen Hirnblutung, spielt es keine große Rolle, ob die Betroffenen zuvor direkt wirksame orale Antikoagulanzien oder Marcumar bekommen haben: Die Prognose ist ähnlich schlecht.
Update Neurologie
Bestellen Sie unseren Fach-Newsletterund bleiben Sie gut informiert.