










Anzeige
Erschienen in:
19.07.2016 | Editorial
Network meta-analyses should be the highest level of evidence in treatment guidelines
Erschienen in: European Archives of Psychiatry and Clinical Neuroscience | Ausgabe 6/2016
Einloggen, um Zugang zu erhaltenExcerpt
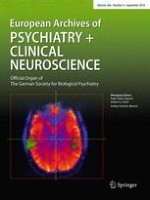
After initial hesitancy due to fears that this procedure might lead to “cookbook medicine” and others, evidence-based medicine (EBM) is now an accepted principle in all fields of medicine including psychiatry. The essence of the evidence is used by many treatment guidelines to inform clinicians in their daily practice. One not entirely resolved issue is, however, which study or evidence synthesis design should be considered as the highest level of evidence. Early statements from McMaster University in Canada [5] (together with the Cochrane Collaboration, the “cradle” of EBM) suggested systematic reviews with meta-analysis can provide the most robust and reliable evidence, but not all guideline producers are in agreement. This is a timely debate, fuelled by the increasing publication of network meta-analyses, a novel approach which takes the assumptions of meta-analysis one step further [3]. Conventional meta-analyses only average the randomised trials comparing two treatments directly (so-called direct evidence). The major criticism has been that meta-analysis compares “apples and oranges”; are trials sufficiently similar so that they can be summarised or are they “heterogeneous”? Network meta-analysis (also called multiple-treatments meta-analysis) additionally uses “indirect evidence”. For example, if in schizophrenia there were trials that compared olanzapine with quetiapine and trials that compared olanzapine with aripiprazole, but no trials comparing quetiapine with aripiprazole directly, we can estimate quetiapine versus aripiprazole indirectly from the other two direct comparisons (see Fig. 1). There are several strengths and added values of this approach: (a) the indirect evidence can fill in the gaps in the evidence matrix, which allows to come up with hierarchies of which drug is probably the best, second best, third best and so on. This information is urgently needed by guidelines, but cannot really be provided by conventional meta-analysis (now sometimes also called “pairwise meta-analysis”). (b) Network meta-analysis can use all kinds of comparisons simultaneously—single antipsychotics versus placebo [11], head-to-head comparisons of new versus old antipsychotics [13], head-to-head comparisons of new drugs [15] —these separate types of comparisons could heretofore be only summarised in separate meta-analyses and viewed “impressionistically” together afterwards [14]. When the network is well connected and provides both direct (e.g. quetiapine vs. aripiprazole directly head-to-head) and indirect (e.g. quetiapine vs. aripiprazole via olanzapine) comparisons, they can be pooled together in the so-called mixed evidence, thus increasing statistical power and the precision of the estimates [3]. This use of the entire information also allows for more timely recommendations compared to conventional pairwise meta-analyses [16]. The underlying assumption of NMA is whether the indirect evidence validly estimates the differences between treatments. This issue is examined in several ways including statistical tests that compare the direct and indirect evidence for all comparisons where both are available [17].
Fig. 1
Principle of the use of indirect evidence in network meta-analysis
× ![]()
…