

Abstract
The time-integrated absorbed dose to the thyroid gland in the years after a fallout event can indicate the potential excess number of thyroid cancers among young individuals after a radionuclide release. Typical mean values of the absorbed dose to the thyroid have been calculated previously using reported data on radioiodine obtained from air sampling and dairy milk surveys in Sweden after the Chernobyl fallout, not including the contribution from 134Cs and 137Cs. We have developed a model for Swedish conditions taking these additional dose contributions into account. Our estimate of the average time-integrated absorbed dose to the thyroid, Dth,tot, during the first 5 years after fallout ranged from 0.5−4.1 mGy for infants and from 0.3−3.3 mGy for adults. The contribution to Dth,tot from 131I through inhalation and milk consumption varied considerably among different regions of Sweden, ranging from 9%−79% in infants, and from 4%−58% in adults. The external irradiation and exposure from the ingestion of 134,137Cs in foodstuffs accounted for the remaining contributions to Dth,tot (i.e. up to 96% for adults). These large variations can be explained by the highly diverse conditions in the regions studied, such as different degrees of fractionation between wet and dry deposition, different grazing restrictions on dairy cattle, and differences in 134,137Cs transfers through food resulting from differences in the local fallout. It is our conclusion that the main contribution to Dth,tot from nuclear power plant fallout in areas subjected to predominantly wet deposition will be from external exposure from ground deposition, followed by internal exposure from contaminated food containing the long-lived fission product 137Cs and the neutron-activated fission product 134Cs. The contribution from 134,137Cs to the thyroid absorbed dose should thus be taken into account in future epidemiological studies.
Export citation and abstract BibTeX RIS

Original content from this work may be used under the terms of the Creative Commons Attribution 3.0 licence. Any further distribution of this work must maintain attribution to the author(s) and the title of the work, journal citation and DOI.
1. Introduction
The increased incidence of thyroid cancer in Belarus, Russia, and Ukraine after the Chernobyl Nuclear Power Plant (NPP) accident among individuals who were children and adolescents at the time of the accident in 1986 initiated extensive research on the radiation dose–response relationship (e.g. UNSCEAR United Nations Scientific Committee on the Effects of Atomic Radiation 2008). Epidemiological studies in these countries revealed a clear exposure–response relationship between the individual thyroid radiation dose and the risk of thyroid cancer (Cardis et al 2005, Jacob et al 2006, Brenner et al 2011, Zablotska et al 2011, Ivanov et al 2012, Tronko et al 2017). Drozdovitch et al (2007) presented national- and region-specific estimates of thyroid absorbed doses, and found that the residents in some regions (oblasts) of Belarus, Russia, and Ukraine experienced thyroid doses well over 100 mGy. In most Western European countries, the thyroid absorbed doses ranged from <1 mGy (e.g. in the Scandinavian countries) to around 20 mGy (in many Eastern European countries outside the former USSR). However, large variations in the time-integrated plume concentration and atmospheric deposition of the Chernobyl fallout also suggest large variations in exposures within each country. In Belarus, there was a substantial dry deposition of 131I, reducing the otherwise relatively high correlation between 131I and 137Cs seen in other countries (e.g. Kruk et al 2004). Hence, the 131I/137Cs ratio in the ground deposition from the Chernobyl fallout in Belarus essentially decreased with increasing 137Cs deposition, and Kruk et al (2004) were able to fit a decreasing power function to the observed data. As a consequence of this, there will not be a proportionality between 131I internal exposures from local fallout and the ground deposition of 137Cs in Belarus (Gavrilin et al 1999), and for regions near the Chernobyl NPP, an inverse relationship was seen between the thyroid absorbed dose and the 137Cs ground deposition (Gavrilin et al 1999). However, Gavrilin et al did not consider the contribution to the thyroid dose from external radiation, and thus underestimated the total thyroid dose. However, estimates by Drozdovitch et al (2010), suggest that this contribution may be negligible (<5%) in areas with the highest deposition of 131I in Belarus and Russia. In contrast to the situation in Belarus, wet deposition of 131I dominated over dry deposition in Sweden, mainly due to rainfall on 28–29 April and rainfall on 8 May 1986, and therefore a more consistent 131I/137Cs ratio was observed (Erlandsson and Isaksson 1988, Mattson and Vesanen 1988, Olofsson and Svensson 1988).
The absorbed dose from radioiodine to the thyroid depends not only on the local deposition density of 131I, 132I, and 132Te, but also on the time-integrated concentration of inhaled short-lived isotopes of iodine in the plume, the iodine status of the population and remedial actions in the crucial period during and just after the passage of the plume. A combination of remaining indoors, restrictions on the grazing of dairy cattle and the intake of stable iodine tablets will substantially reduce the transfer of 131I. In Belarus, Ukraine, and the western part of Russia, where such measures were often not implemented, infants and children were especially affected by the unmitigated transfer of iodine from the Chernobyl NPP fallout. The transfer to the thyroid was further increased by the lack of iodine-supplemented table salt, the common practice of small-scale dairy farming, and the use of locally produced milk as a main source of protein for children. According to Drozdovitch et al 2010, the absorbed dose to the thyroid varied by a factor of 20 between infants and adolescents in a case-control study of thyroid cancer cases in Belarus and Russia. In addition to a higher milk consumption per unit body weight, this difference in absorbed dose is also explained by the smaller mass of the thyroid gland in infants.
Some research has focused on estimating the thyroid dose using data on the intake of 131I in contaminated dairy milk and direct monitoring of the radioiodine content in the thyroid gland. Estimates of national averages of thyroid doses to the general population in the study by Drozdovitch et al (2007) basically considered thyroid 131I uptake through inhalation and the ingestion of contaminated foodstuffs, but to some extent also considered the external dose contribution from short-lived nuclides. Although the national average, as estimated by both UNSCEAR (1988) and Drozdovitch et al (2007), suggests an average thyroid absorbed dose of 1 mGy for infants (1 year old), it can be assumed that the exposure in different countries will vary considerably. A large variation in the absorbed thyroid dose with age has been reported in a population-based case control study of childhood thyroid cancer in Belarus and Russia. The main contribution to the exposure was found to be the ingestion of 131I through milk consumption, whereas less than 1% was due to food contaminated with 134,137Cs (Drozdovitch et al 2010).
The contribution from external exposure of the thyroid can be estimated by modelling the external gamma radiation exposure to the individual as a function of the local 137Cs deposition (UNSCEAR 2014, Jönsson et al 2017). In previous studies models have been developed to calculate the whole-body external effective dose to the Swedish population using extensive databases of exposure (Jönsson et al 2017). We have also modelled the lifetime effective dose resulting from both internal and external exposure in hunter households in the three regions of Sweden with the highest fallout after the Chernobyl NPP accident (Tondel et al 2017). Our aim was to develop a valid method of assessing the individual lifetime dose for future epidemiological investigations. However, the main aim of the present study was to include all the available data on 131I, together with information available in databases, to develop a model for the estimation of the total thyroid absorbed dose from both internal and external exposure, in which all relevant nuclides are included. This will enable the quantification of various contributions to the thyroid absorbed dose using an expansion of the model developed by Jönsson et al (2017), as well as the internal contribution from the ingestion of 134Cs and 137Cs, obtained from a model presented by Rääf et al (2006). With the exception of the studies by Drozdovitch et al (2010, 2013), only a few studies have explicitly incorporated both internal and external radiation exposure in the modelling of the thyroid dose.
The second aim of this study was to determine whether this model, with its identifiable components, could be used to retrospectively reconstruct the thyroid radiation dose to populations in areas affected by the Chernobyl fallout for future applications in epidemiological studies on the incidence of thyroid cancer in Sweden. Therefore, efforts have been made to convert or express the various contributions to the thyroid absorbed dose, rather than quantifying the equivalent dose to the thyroid. Using the absorbed dose in epidemiological studies on the incidence of thyroid cancer makes such studies independent of previously used weighing of organ detriments (ICRP 2007).
2. Material and methods
The time-integrated absorbed dose to the thyroid, Dth,tot, accumulated at a given time after the onset of fallout, tacc, can be divided into four components:

i.e. the ingestion of 131I via milk (Dmilk(tacc)), the inhalation of airborne 131I (Dinh(tacc)), the combined external exposure from 134,137Cs and short-lived nuclides on the ground (Dext(tacc)), and the ingestion of 134,137Cs (DCs-ing*(tacc)). In the following sections, each of these components is identified using data on radioiodine in dairy milk, average regional values of inhalation doses, and either local or regional averages of 137Cs deposition. Drozdovitch et al (2010) found that both radioiodine (131I, 132I, 133I, 135I) and radiotellurium (131mTe, 132Te) decaying to 131I and 132I in the Chernobyl fallout might contribute to the thyroid dose by inhalation. However, when also considering ingestion pathways, the radiotellurium nuclides with their short half-lives and 132I accounted for less than 5% of the total thyroid absorbed dose. Therefore, the focus of the present study was on the dose contribution from 131I in milk, although some calculations on the additional 132Te contribution were performed to confirm that this contribution can been neglected in Sweden.
In this study, 11 regions (counties) were selected for the assessment of Dth,tot. The selection was based on (1) regions with large, predominantly urban populations, such as the areas around the cities of Stockholm, Gothenburg, and Malmö (Stockholm, Västra Götaland, and Skåne regions), (2) regions characterised by wet deposition of Chernobyl 137Cs, and (3) regions characterised by dry deposition of Chernobyl 137Cs (Gotland county). An overview of the ground deposition of 137Cs (in terms of surface equivalent distribution, Aesd) in the selected regions can be found in table 1.
Table 1. Time-integrated 131I activity concentration in dairy milk (Bq kg−1 d), average effective dose, Einh (μSv), resulting from inhalation for adults, and the average equivalent surface deposition of 137Cs, Aesd (kBq m−2), (Finck et al 1992) in 11 Swedish regions studied.
| Time-integrated cmilk,I-13 | Inhalation effective dose, Einh | Average equivalent surface deposition of 137Cs, Aesd | |
|---|---|---|---|
| Region | Bq kg−1 d | μSv | kBq m−2 |
| Dalarna | 100 | 16.0 | 2.47 (wet and high) |
| Gävleborg | 311 | 16.0 | 13.4 |
| Gotland | 1721 | 16.0 | 3.14 (dry and low) |
| Jämtland | 91.0 | 4.12 | 6.52 |
| Skåne | 160 | 7.2 | 1.76 |
| Södermanland | 449 | 16.0 | 5.2 |
| Uppsala | 302 | 16.0 | 15.4 |
| Västerbotten | 181 | 1.90 | 14.2 |
| Västernorrland | 357 | 4.12 | 28.4 (wet and high) |
| Västmanland | 224 | 16.0 | 11.1 |
| Västra Götaland | 142 | 3.4 | 1.87 |
*Integrated over at least 60 days after the event on 26 April 1986.
2.1. 131I ingestion doses via dairy milk
Dairy milk is considered one of the major pathways for the ingestion of radioactive iodine (e.g. Drozdovitch et al 2010). If Dmilk(tacc) (μGy) denotes the time-integrated absorbed dose contribution originating from the intake of dairy milk to an individual at a certain time tacc(days) after deposition, the following relationship can be expressed:

where cmilk,I-131 (Bq kg−1) is the regional average activity concentration of 131I in milk in dairies at a certain time t (days), and a(age) is the age-dependent milk consumption (kg d−1). The factor kdelay is the factor accounting for the decay of 131I in milk during the delay between packaging of the milk at the dairy and reaching the consumer (here assumed to be 3.5 d, corresponding to a relative decay of 0.75). ding(age) is the age-dependent committed absorbed dose per unit intake of 131I (μGy Bq−1). ding(age) is related to eing(age) (μSv Bq−1), which is the age- and gender-dependent committed equivalent dose per unit intake of 131I, as given by the ICRP (1993). The principal radionuclides of interest in this case, 131I, 134Cs, and 137Cs, all decay through beta emission with accompanying gamma emission, and it can be assumed that the equivalent dose to the thyroid is numerically identical to the internal absorbed dose. A multi-polynomial curve fitting of ding (μGy/Bq) for 131I as a function of age (y) was obtained using the age-dependent eing values from ICRP (1993) and is given in:

In the present study, cmilk,I-131 was retrieved from national measurements of 131I concentration in retail dairy milk obtained by the former Swedish Radiation Protection Institute (Andersson and Nyholm 1986). The data were obtained from milk bought in shops in various Swedish cities in 11 different regions, including those with the highest ground deposition of 137Cs (listed in table 1). The reported data on cmilk,I-131 varies greatly over time and between the counties. One could assume a roughly exponential decrease in the 131I concentration in dairy milk over time, but the data show that the concentration fluctuates, probably depending on the relative contributions from locally contaminated farms, and the limited number of sampling locations. Thus, data on dairy milk concentrations at the regional level are not suitable for curve fitting, which would have enabled the extraction of analytical expressions for cmilk as a function of t. Instead, the time-integrated dairy milk concentrations of 131I were computed numerically to obtain the accumulated 131I ingestion by milk at the regional level as a function of age.
Consumption estimates of dairy milk and dairy products have been published by the Swedish Board of Agriculture (SBA 2009), who estimated that an adult consumed, on average, 140 kg y−1 of fresh milk in 1986. It was assumed that an infant consumes no dairy milk, but instead, on average, 0.75 kg mother's milk per day during its first year. It is also assumed that 0.30 of the time-integrated intake of 131I by the mother through dairy milk would be transferred to mother's milk (ICRP 2004, 2012). Children between 1 and 6 years of age are assumed to consume 50 kg dairy milk y−1, pre-adolescents (7–12 y) 100 kg dairy milk y−1, and adolescents and adults 150 kg dairy milk y−1. Based on these three estimates, the following continuous expression was used to model the daily consumption of dairy milk, a(age) (kg d−1):

Table 1 presents the time-integrated 131I concentrations in milk used in the estimation of the ingestion doses, Dmilk.
2.2. 131I inhalation doses
Dinh(tacc) denotes the time-integrated absorbed dose to the thyroid from the inhalation of radionuclides during the time tacc after deposition. It is in principle given by:

where cair,nuclide (Bq m−3) is the activity concentration of a certain radionuclide in air at a certain time t (determined by air sampling); B(age) (m3 h−1) is the age-dependent inhalation rate of a person present in the area of the plume: and dinh(age) (μGy Bq−1) is the age-dependent, time-integrated absorbed dose to the thyroid (assumed to be numerically equal to the committed equivalent dose, einh) per unit intake of each radionuclide.
There are no detailed data available on the time pattern of the air concentration, cair,nuclide, for 131I, 132I, and 132Te for all the Swedish regions during the weeks following the Chernobyl NPP accident. This makes it difficult to compute the expression in (5). Therefore, estimates of the effective dose to an adult resulting from inhalation reported by Finck et al 1992 were used based on the authors' assessment of the time-integrated radionuclide concentration in air, measured at six air sampling stations in Sweden. The authors assumed that iodine in particle form had, on average, an activity median aerodynamic diameter of 1 μm. The data from each air sampling station were then associated with the geographically nearest region, allowing six different values of region-averaged Einh to be approximated. This allowed the average Einh (μSv) to be estimated for the 11 Swedish regions studied (table 1). Because the uptake of inhaled radioiodine and radiotellurium is significantly higher in the thyroid than in other organs, the quotient between the committed equivalent dose, einh, and the effective dose, Einh, is higher for these radionuclides than for other airborne radioactive elements in the Chernobyl NPP plume. A conservative estimate of einh can therefore be obtained by scaling up the values of Einh given by Finck et al (1992) by some representative quotient of einh/Einh for radioiodine and radiotellurium. Assuming then, as previously mentioned, that the equivalent thyroid dose is numerically equal the corresponding absorbed dose, Dinh(tacc,age),we estimated the Dinh(tacc,age) using an alternative expression:

where kth/E (Sv/Sv) is the ratio between the committed equivalent dose to the thyroid per unit intake of radioiodine or radiotellurium by inhalation, einh, and the committed effective dose, Einh, from the same intake. Fage is a parameter correcting for age-dependent breathing rates, B(age), and is described in more detail in the following.
Based on einh values of 131I and 132Te taken from ICRP (1993) it can be seen from table 2 that kth/E appears to be in the range of 15–20 for gaseous forms of radioiodine and radiotellurium, and for highly soluble aerosol particles (absorption type F = fast uptake to blood). Based on the results given by Devell (1991), that a major part of the iodine was in gaseous form (see table 5 below), it can be conservatively assumed that the committed equivalent thyroid dose from inhalation of airborne Chernobyl NPP releases in Sweden will not be underestimated if a generic value of kth/E of 20 is assumed for all ages. Hence, the contributions from medium (M) and slow absorption (S) of particulates to the respiratory tract are not included as they are assumed to have negligible impact on kth/E.
Table 2. Relative values of the equivalent dose per unit effective dose, kth/E, for inhaled forms of 131I and 132Te. Particulate form refers to inhaled particles with an activity median aerodynamic diameter of 1 μm, categorised in three different absorption types: F = fast, M = medium, and S = slow uptake from the respiratory tract through inhalation to the plasma. Data obtained from ICRP (1995).
| 131I | 132Te | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Age | Particulate | Elemental | Methyl iodide (CH3I) | Particulate | Elemental | ||||
| F | M | S | I2 | CH3I | F | M | S | gas | |
| 1 y | 19.4 | 14 | 2.6 | 20 | 19.2 | 16.1 | 5.4 | 0.32 | 17.3 |
| Adult | 20.3 | 9.2 | 0.69 | 19.5 | 20.7 | 13.9 | 2.2 | 0.16 | 14.9 |
The function Fage (6) has been used to transform the estimates of the thyroid absorbed dose to adults to a corresponding absorbed dose at various ages. Fage(age) accounts for: (1) the inhalation rate, B (m3 h−1), which is age-dependent and also governed by the distribution of physical activities during the day, (2) the relative fractions of the various forms of the airborne contaminant, fstate, and (3) the committed dose per unit intake of each form of the radionuclides (131I and 132Te).
To obtain age-dependent diurnal average breathing rates, B24h(age), representative of individuals engaged in normal physical activity, the breathing rates during various physical activities (table 3) were combined with the assumed distribution of the level of physical activity as a function of age proposed by ICRP (1993), and given in table 4.
Table 3. Inhalation rate B (m3 h−1) as a function of age during various types of physical activity. Data taken from table 4 in ICRP 1995.
| Age | Sleeping | Sitting | Light exercise | Heavy exercise |
|---|---|---|---|---|
| 3 months | 0.09 | 0 | 0.19 | 0 |
| 1 y | 0.15 | 0.22 | 0.35 | 0 |
| 5 y | 0.24 | 0.32 | 0.57 | 0 |
| 10 y | 0.31 | 0.38 | 1.12 | 2.22 |
| 15 y | 0.42 | 0.48 | 1.38 | 2.92 |
| Adults | 0.45 | 0.54 | 1.5 | 3.0 |
Table 4. Representative distribution of physical activity levels for individuals as a function of age, and representative diurnal average inhalation rates, B24h (m3 h−1).
| Age | Sleeping | Sitting | Light exercise | Heavy exercise | B24h |
|---|---|---|---|---|---|
| % | % | % | % | m3 h−1 | |
| 3 months | 70 | 0 | 30 | 0 | 0.12 |
| 1 y | 60 | 20 | 20 | 0 | 0.19 |
| 5 y | 50 | 27 | 23 | 0 | 0.36 |
| 10 y | 40 | 35 | 22 | 3 | 0.50 |
| 15 y | 37 | 38 | 22 | 3 | 0.62 |
| Adults | 33 | 40 | 24 | 3 | 0.74 |
As mentioned previously, it was assumed that 131I dominates the radioiodine dose contribution. Therefore, only the relative distribution of the chemical forms of that radionuclide was considered, and other radioiodine isotopes were not taken into account in the dose calculations. The relative impact of these 131I chemical states on the absorbed dose was obtained by summing the products of the relative fraction of a given chemical form, fstate, with the age-specific committed equivalent dose coefficient for the particular state, einh,state, over all different forms considered (7). Furthermore, the values of Fage are normalised to Fage for an adult who is present in air with a given concentration of organically bound iodine, to be consistent with the assumed value of kth/E of 20 in (6) for methyl iodide.

The values of fstate for the chemical forms of iodine during the weeks after the Chernobyl fallout in Sweden were estimated using data from Devell (1991) and are presented in table 5. The table gives the relative fractions, fstate, of particulate, elemental, and methyl iodide found in the air filter station at Studsvik (58°46 N; 17° 25 E) during certain periods after the arrival of the Chernobyl plume. The values of fstate were then combined with the breathing rate for a given age group, according to table 6, and the following continuous mathematical expression for Fage could then be obtained:

Table 5. Relative distribution, fstate, between particle-bound iodine, elemental iodine (I2), and methyl iodide (CH3I) according to air filter measurements reported by Devell (1991).
| Time period (yyyy-mm-dd) | Particulate | Elemental | Methyl iodide |
|---|---|---|---|
| 1986-04-30–1986-05-01 | 0.25 | 0.375 | 0.375 |
| 1986-05-01–1986-05-02 | 0.18 | 0.18 | 0.64 |
| 1986-05-05–1986-05-07 | 0.4 | 0.4 | 0.2 |
| 1986-05-07–1986-05-12 | 0.4 | 0.4 | 0.2 |
| After 1986-05-12 | 0.15 | 0.25 | 0.6 |
| Average | 0.276 | 0.362 | 0.362 |
Table 6. Age-dependent committed equivalent dose per unit intake of 131I, einh(age) (μSv/Bq) (ICRP 1993), normalised to that of methyl iodide in adults, and estimated Fage factor based on the relative distribution of iodine given in table 5.
| Particulate | ||||||
|---|---|---|---|---|---|---|
| Age (y) | S | F | M | Elemental (I2) | Methyl iodide (CH3I) | Fage |
| 1 | 0.0023 | 1.3 | 0.21 | 3.0 | 2.4 | 2.4 |
| 5 | 0.0021 | 1.4 | 0.20 | 3.6 | 2.8 | 2.8 |
| 10 | 0.0016 | 1.0 | 0.16 | 2.7 | 2.2 | 2.2 |
| 15 | 0.0010 | 0.69 | 0.11 | 2.0 | 1.5 | 1.5 |
| Adult | 0.000 67 | 0.59 | 0.071 | 1.9 | 1.0 | 1 |
In summary, the regional average effective dose values, Einh, presented by Finck et al (1992), and used in equation (6), were scaled up by a factor of 20, regardless of the chemical state of 131I and 132Te, to obtain a conservative estimate of the corresponding equivalent thyroid dose that could be transformed into the absorbed inhalation dose (mGy) to the thyroid, Dinh, regardless of age. The age dependence therefore originates mainly from a combination of age dependence in ingestion doses per unit intake and behavioural factors related to inhalation rates, Fage.
2.3. External gamma radiation exposure
Living in an area affected by fallout of gamma-emitting fission products will contribute to the external exposure of the individual's organs. The time pattern of the external dose, in terms of the ambient dose rate per unit ground deposition of the long-lived fission product 137Cs, has been expressed in a model presented by Jönsson et al (2017). This model can be extended to include estimates of the dose to a particular organ, provided the relationship between the specific organ exposure and air kerma is known. The time-integrated dose to the thyroid from external exposure, Dext(tacc) (μSv), can then be expressed as:

where Aesd(x, y) (kBq m−2) is the equivalent surface deposition of 137Cs at the location of the home of a fictive resident. If used in a study with authentic individuals, Aesd should be taken as the equivalent surface deposition of 137Cs (kBq m−2) at the coordinates of the dwelling of that person (taken, for example, from a digitised fallout map provided by the Swedish Geological Survey, SGU). In the present study, fictive individuals were assumed to live at a location where Aesd is equal to that of the regional average. The factor dCs (μSv h−1/kBq m−2) is the ratio between the initial ambient equivalent dose rate, H* (10), 1 m above ground at the location (x, y) and the equivalent surface deposition, Aesd, at the same location. The value of dCs was found to be 0.116 μSv h−1/(kBq m−2) in areas subjected to wet deposition in Sweden (Jönsson et al 2017). The ambient dose rate per hour is converted to the corresponding value per day by multiplying by 24. Φkerma/H(600 keV) (μGy μSv−1) is the conversion factor between air kerma and the ambient dose rate, H* (10), at location (x, y); set to 0.83 (ICRU 1992). The conversion factor refers to a photon energy of 600 keV, which is approximately the average photon energy emitted by the Chernobyl NPP fallout gamma emitters (Jönsson et al 2017). Fsnow is a factor accounting for the shielding of ground-deposited gamma emitters by the snow cover during the winter. Values for Fsnow for the various counties studied were taken from Finck (1992).
The factor kth,K (age) (μSv μGy−1) in (9) is the age-dependent conversion factor between the air kerma rate 1 m above ground and the equivalent dose rate in the thyroid for an individual. The equivalent dose rate is assumed to be numerically equal to the absorbed dose rate resulting from external gamma exposure. Table 7 presents a compilation of kth,K values taken from the literature, used to obtain an age-dependent continuous mathematical expression to calculate the thyroid absorbed dose rate from the kerma rate. A polynomial expression was fitted to the data up to 20 years, after which it is assumed that eth is constant at 1.017, i.e., the average for males and females of any age >20 years.

Table 7. Age-dependent conversion factors between air kerma and absorbed thyroid dose (Gy/Gy), kth,K(age), for a rotational irradiation geometry and a photon energy of 600 keV, corresponding to the mean primary photon energy of the gamma emitters in the Chernobyl NPP fallout in Sweden (Jönsson et al 2017). Data taken from Lee et al (2006) for individuals <20 y, and from Zankl et al (1997) for adults.
| Age (y) | Males | Females |
|---|---|---|
| 1 (9 months) | 1.327 | N/A |
| 1−6 | N/A | 1.347 |
| 8 | N/A | 1.041 |
| 11 | 0.967 | N/A |
| 14 | 0.930 | N/A |
| 20 | 0.962 | 1.072 |
| Equivalent surface distribution (kSEQ/ROT) | 0.785a | |
aThe average for men and women in Table B.68 in Zankl et al (1997). N/A = Data not available.
A further correction factor, kSEQ/ROT, is introduced to account for the fact that a surface distribution of gamma emitters generates a radiation field deviating from a parallel rotational gamma fluence. A factor of 0.785 was calculated as an average for males and females assuming infinite surface deposition shielded by a soil layer with a mass density of 0.5 g cm−2. In this study, this factor was assumed to be independent of age.
Finally, r(t) in (9) is the normalised time function of the ambient dose rate at time t after the onset of the Chernobyl fallout, taken from Jönsson et al 2017. It comprises the contributions from both short-lived fission products such as 131I, 132Te, and 140Ba, as well as the more long-lived radiocaesium isotopes 134Cs and 137Cs. r(t) is expressed as:

The factor fout is the fraction spent outdoors (0.20) taken from Almgren et al (2008). fshield is the shielding factor of the residential building, here set to 0.4 for a photon energy of 600 keV, in accordance with the aforementioned assumption of a mean gamma-ray energy of all deposited fission products (Jönsson et al 2017).
2.4. Internal dose from the ingestion of 134Cs and 137Cs
The fourth component in the time-integrated absorbed dose to the thyroid, DCs-ing, arises from the ingestion of 137Cs and 134Cs. Assuming uniform uptake in the whole body, the absorbed dose to the thyroid is the same as the rest of the body, according to the so-called S-factors presented by Snyder et al (1975). DCs-ing as a function of time, tacc, after the onset of fallout can then be expressed for 137Cs as:

where Aesd(region) (kBq m−2) is the average equivalent surface deposition of 137Cs in the region where the person lives (taken from the SGU digital map). Values of Aesd(region) are given in table 1, and the term f134/137 is the activity ratio between 134Cs and 137Cs in the initial Chernobyl fallout over Sweden, assumed to be 0.56 (Rääf et al 2006). Tag (Bq kg−1 (kBq m−2)−1) is the sex-dependent radioecological transfer of caesium from ground deposition to man, taken from region-averaged data in Rääf et al (2006). Tag(t, sex) for 137Cs is expressed as:

where Tag(t) is given by:

The above expression is obtained from data presented in Rääf et al (2006), where time-dependent expressions of the population averaged 137Cs body concentration, observed in various Swedish communities, as a function of initial ground deposition of 137Cs in the region of residence were made to obtain a measure of the long-term radioecological transfer of radiocaesium to man. The term ksex (1 for children and males and 0.61 for adult females (age > 20 y)) accounts for the difference in the 137Cs equilibrium whole-body content per unit body mass as observed, for example, by Rääf et al (2006). The term eCs-137 is the effective dose conversion factor (μSv y−1/(Bq kg−1)) taken from Falk et al (1991) based on the biokinetic models by Leggett et al (1984), and is in turn expressed as:

where w(age) (kg) is the mean body weight of an individual at a certain age. Body weight as a function of age among the Swedish residents in the study was taken from Wikland et al (2002). The mathematical expression deduced for the males and females is given in table 8.
Table 8. Typical body weights for males and females as a function of age.
| Age | Males | Females |
|---|---|---|
| <21 | −0.000 0021·age6 + 0.000 262·age5 − 0.0118·age4 | −0.000 0057·age6 + 0.000 553·age5 |
| + 0.230·age3 − 1.876·age2 + 8.077·age + 3.89 | − 0.0199·age4 + 0.319·age3 − 2.16·age2 + 7.44·age + 3.95 | |
| 21 and over | 78 | 63 |
The limitation of the model given in (15) is that it is not specifically intended for absorbed dose estimation in various risk organs. Ideally, it would be better to have model such as that presented by Snyder et al (1975) for a 70 kg adult male, but for body weights corresponding to children. However, to the best of our knowledge, no such model exists. Although the S-factors given by Snyder could be adapted and updated using the parameters presented by ICRP (2016), the photon absorption fractions for various source and target organs listed refer only to an adult male and an adult female phantom. Due to the lack of appropriate weight-dependent S-factors in risk organs for children, we have used the Leggett and Falk model to predict the weight-dependent S-factor.
The expression corresponding to equation (14) for the transfer of 134Cs is:

where T½,Cs-134 and T½,Cs-137 are the physical half-lives of 134Cs and 137Cs (2.06 and 30.0 y), respectively eCs-134 is the corresponding effective dose conversion factor (mSv y−1/(Bq kg−1)) for 134Cs taken from Falk et al (1991), and can be expressed as:

It is thus assumed that both eCs-134 and eCs-137 are numerically equal to the absorbed dose in the thyroid, since Cs is assumed to be homogeneously distributed in all the body organs. Support for this assumption can be found by comparing eCs-137 given by Falk et al (1991) for a 70 kg adult with the absorbed dose to the thyroid for the 70 mkg reference adult male used by Snyder et al (1975). For the homogeneous distribution of the radionuclide with a concentration of 1 Bq kg−1, values of 2.2 μSv and 2.3 μGy are obtained from Snyder et al (1975) and Falk et al (1991), respectively, and the numerical difference between the two models is therefore considered insignificant.
A factor of (1000/365.25) (μSv/mSv)(y d−1) is introduced into (12) to convert the dose coefficients eCs-134 and eCs-137 into daily absorbed dose (μSv d−1), since tacc, is consistently defined in terms of days after the onset of fallout for the other dose contributions Dinh, Dmilk, and Dext.
In analogy with the Dmilk component of radioiodine for infants we have assumed that all ingestion of radiocaesium by infants during their first year of life is through mother's milk, with a fraction of 18% of the integrated intake of radiocaesium by the mother ending up in the mothers' milk (ICRP 2004, 2012). Hence, the proportionality of 0.18 has been assumed between the Tag for infants compared with Tag for adult women (14).
2.5. Computation of the 5-year total thyroid absorbed dose from the Chernobyl NPP fallout
The above expressions (equations (2)–(17)) can be combined to give the following expression for the total absorbed thyroid dose to an individual, living at coordinates (x, y), of a certain age and sex at time tacc after the onset of the Chernobyl fallout:
The coordinates x, y can be expressed in a format that is compatible with that used in the GIS format of the SGU 137Cs fallout map to obtain Aesd (kBq 137Cs/m2 at the dwelling location). In this study, the time tacc was chosen to be 5 years (or 1826 d) after the onset of fallout (i.e. up to 1 May 1991), as this reflects the predicted latency period of thyroid cancer of 4–6 years (e.g., Nikiforov 2006).
2.6. Estimation of the time-integrated total absorbed dose to the thyroid in fictive individuals of certain ages
The expression in (18) was used to compute the 5-year time-integrated absorbed dose to the thyroid of reference individuals with standard body weights depending on age, the standard occupancy factor for Sweden, standard shielding factor for Swedish houses, region-specific snow shielding factor, and gender difference in 137Cs body concentration (represented in (13)), living in any of the 11 regions studied. It was assumed that these fictive individuals lived in the same dwelling during the five-year period considered, at a location with the same local Aesd as the regional average value. For the 131I intake through milk and inhalation, Dmilk and Dinh represent the time-integrated exposures to the thyroid, respectively, and incurred by the accumulated intakes during a time tacc (1986–1991). Due to the short physical half-life of 131I, 132I, and 132Te, these nuclides will not make any significant contribution to the 5-year absorbed dose to the thyroid after 3 months. Values of Dth,tot for each year between 1986 and 1991 were calculated for the fictive individual (with age-dependent parameters adjusted for the continuous aging of the person), and the relative proportions of the four components of Dth,tot were assessed.
A standard spreadsheet (MS Excel) was employed for calculations of the total dose, Dth,tot. STATISTICATM 10 was used for curve fitting of body weight w, the age-normalising factor, Fage, and the conversion factor kth,E.
3. Results
3.1. Average time-integrated regional 131I concentration in dairy milk and its correlation to regional fallout
The average regional values of cmilk for three different regions after the onset of the Chernobyl NPP fallout are plotted in figure 1. As mentioned above, the temporal variation in the average regional 131I concentration in dairy milk is not suitable for curve fitting and the time integration in (1) was done numerically. It can also be seen that after tacc = 50 d there was virtually no radioiodine in Swedish milk. Although a relatively high correlation was found between the average regional deposition of 137Cs and the corresponding ground deposition of 131I in Sweden (r2 = 0.84), the average time-integrated regional dairy milk concentration of 131I showed a surprisingly weak correlation with both the regional deposition of 131I and the deposition of 137Cs, Aesd (figure 2). This can probably be explained by the fact that grazing was interrupted or stopped when the Chernobyl plume reached the Swedish mainland, leading to considerable mitigation of the transfer of 131I into dairy milk in most counties, except, to some extent, Gotland, the most eastern part of Sweden, and first affected by the fallout. An additional explanation of the lack of correlation between cmilk and Aesd and cmilk and AI-131 could be that the contribution due to the inhalation of 131I by the grazing cattle varied between regions. It is also important to note that the regional average of 137Cs is calculated from detailed aerial measurements covering the entire region, whereas the calculation of the regional average 131I deposition is based only on a few measurements from grass surfaces, and therefore does not necessarily reflect the true 131I deposition in the entire region. Our conclusion is that neither the regional average values of AI-131 nor Aesd for 137Cs, can be used as a proxy for the regional transfer of 131I to milk, which necessitates the use of region-specific values of cmilk in (18).
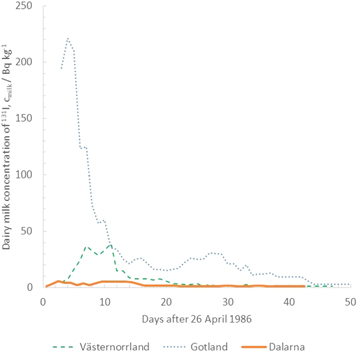
Figure 1. 131I concentration in dairy milk (Bq kg−1) in some Swedish counties as a function of time after the Chernobyl NPP accident on 26 April 1986. Gotland (low, dry deposition), Dalarna (low, wet deposition) and Västernorrland (high, wet deposition).
Download figure:
Standard image High-resolution image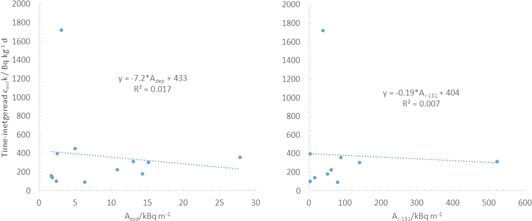
Figure 2. Time-integrated 131I concentration in dairy milk (Bq kg−1 d) in some Swedish regions (counties) versus average regional surface equivalent deposition of 137Cs, (Aesd) (left) and corresponding average deposition of 131I, (AI-131).
Download figure:
Standard image High-resolution image3.2. Time-integrated thyroid absorbed dose in various regions
The 5-year time-integrated absorbed dose to the thyroid (1986–1991) in fictive individuals living in 11 Swedish regions ranged from 0.3−3.3 mGy for adults and 0.5−4.1 mGy for infants (table 9). The values of Dinh are deliberately conservative on average, although there may have been local variations in inhalation doses depending on the 131I concentration in the air and the extent of the individual's outdoor activities. However, considering that in almost 10% of Swedish households at least one resident is a hunter, a transfer factor, Tag,int, of 30 must be applied (Rääf et al 2006), resulting in three times higher DCs-ing values to the thyroid in those living in hunter households. Furthermore, local deposition, Aesd(x,y), can be considerably higher than the regional average, which will increase the external contribution, Dext. For a member of a hunting household living in the most affected areas in Sweden (In the the town of Gävle with an average Aesd of 49.7 kBq m−2 137Cs (Lindgren and Hubbard 2002), the 5-year time-integrated absorbed dose to the thyroid of a baby born in 1986 could be, on average, up to 6.6 mGy).
Table 9. 5-year time-integrated (1986–1991) absorbed dose (mGy) to the thyroid, Dth,tot(5 y), and its contributions from inhalation of radioiodine, Dinh, milk consumption of radioiodine, Dmilk, external radiation, Dext, and ingestion of radiocesium, DCs-ing, for infants and adults in 11 Swedish regions resulting from the Chernobyl NPP fallout.
| Dinh | Dmilk | Dext | DCs-ing | Dth,tot | ||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Infant | Adult | Infant | Adult | Infant | Adult | Infant | Adult | NB | Adult | |||||||||||
| Region | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F | M | F |
| Dalarna | 0.66 | 0.66 | 0.32 | 0.32 | 0.06 | 0.06 | 0.01 | 0.01 | 0.28 | 0.28 | 0.21 | 0.23 | 0.04 | 0.04 | 0.07 | 0.04 | 1.05 | 1.05 | 0.61 | 0.60 |
| Gävleborg | 0.66 | 0.66 | 0.32 | 0.32 | 0.19 | 0.19 | 0.04 | 0.04 | 1.53 | 1.53 | 1.12 | 1.24 | 0.24 | 0.23 | 0.39 | 0.23 | 2.62 | 2.62 | 1.86 | 1.83 |
| Gotland | 0.66 | 0.66 | 0.32 | 0.32 | 1.06 | 1.06 | 0.21 | 0.21 | 0.41 | 0.41 | 0.30 | 0.33 | 0.06 | 0.05 | 0.09 | 0.05 | 2.19 | 2.19 | 0.92 | 0.92 |
| Jämtland | 0.17 | 0.17 | 0.08 | 0.08 | 0.06 | 0.06 | 0.01 | 0.01 | 0.74 | 0.74 | 0.54 | 0.60 | 0.12 | 0.11 | 0.19 | 0.11 | 1.08 | 1.08 | 0.82 | 0.81 |
| Skåne | 0.30 | 0.30 | 0.14 | 0.14 | 0.10 | 0.10 | 0.02 | 0.02 | 0.23 | 0.23 | 0.07 | 0.09 | 0.03 | 0.03 | 0.04 | 0.03 | 0.66 | 0.66 | 0.27 | 0.29 |
| Södermanland | 0.66 | 0.66 | 0.32 | 0.32 | 0.28 | 0.28 | 0.06 | 0.06 | 0.64 | 0.64 | 0.46 | 0.52 | 0.09 | 0.09 | 0.15 | 0.09 | 1.67 | 1.67 | 0.99 | 0.98 |
| Uppsala | 0.66 | 0.66 | 0.32 | 0.32 | 0.19 | 0.19 | 0.04 | 0.04 | 1.88 | 1.88 | 1.37 | 1.52 | 0.27 | 0.27 | 0.45 | 0.26 | 3.00 | 2.99 | 2.17 | 2.14 |
| Västerbotten | 0.08 | 0.08 | 0.04 | 0.04 | 0.11 | 0.11 | 0.02 | 0.02 | 1.60 | 1.62 | 1.18 | 1.31 | 0.25 | 0.25 | 0.41 | 0.24 | 2.05 | 2.05 | 1.65 | 1.62 |
| Västernorrland | 0.17 | 0.17 | 0.08 | 0.08 | 0.22 | 0.22 | 0.04 | 0.04 | 3.23 | 3.23 | 2.35 | 2.62 | 0.50 | 0.50 | 0.82 | 0.49 | 4.12 | 4.11 | 3.30 | 3.23 |
| Västmanland | 0.66 | 0.66 | 0.32 | 0.32 | 0.14 | 0.14 | 0.03 | 0.03 | 1.33 | 1.35 | 0.98 | 1.09 | 0.20 | 0.19 | 0.32 | 0.19 | 2.33 | 2.34 | 1.65 | 1.63 |
| Västra Götaland | 0.14 | 0.14 | 0.07 | 0.07 | 0.09 | 0.09 | 0.02 | 0.02 | 0.21 | 0.20 | 0.15 | 0.17 | 0.03 | 0.03 | 0.05 | 0.03 | 0.47 | 0.47 | 0.29 | 0.28 |
The dose contribution from short-lived 132Te (which decays to 132I) to Dmilk was estimated roughly using the ingestion dose coefficients provided by ICRP (1993). This coefficient is about a factor of 6 lower for 132Te than for 131I for infants (and more than 10 times lower for children older than 5 y), taking into account that the physical half-life of 132Te is considerably shorter (3.3 d for 132Te versus 8.06 d for 131I). Using data from Devell (1991), who reported an initial air concentration ratio between 132Te and 131I of 0.57 at one air sampling station in Sweden on 30 April 1986, and then assuming a similar transfer of 132Te from pasture through cow's milk, results in Dmilk values for 132Te in the range of 3%–4% of the corresponding value for 131I, which is in agreement with those computed by Droztdovitch et al (2010). It can thus be concluded that this contribution is also of negligible importance in the Swedish estimates of Dth,tot.
The relative contribution to the time-integrated total absorbed dose to the thyroid due to inhalation, external dose, and food consumption for individuals of various ages at the onset of the Chernobyl fallout in three Swedish counties over a 5-year period (1986–1991) is given in table 10. Västernorrland was the region with the highest regional-averaged Aesd, while Gotland had the highest time-integrated regional-averaged 131I concentration in dairy milk (see also table 1). The model predicts no significant gender difference for infants, whereas the difference is more evident for Dext and Ding in adults. In the case of Ding this is mainly due to the factor fsex, which accounts for the observed difference in the 137Cs uptake per kg body mass in males and females (Rääf et al 2006). The gender difference is reversed in Dext, and adult females exhibit somewhat higher values due to their different kth,K factor (which is due to the difference in average height between males and females). When combined to form Dth,tot, the gender differences appear to cancel out, or are unimportant.
Table 10. Relative contributions (%) to the 5-year time-integrated dose to the thyroid from the Chernobyl fallout in three Swedish regions. Västernorrland and Dalarna were subject to 131I fallout mainly through wet deposition, whereas Gotland was primarily affected by dry deposition (Arntsing et al 1991).
| Region | Dinh | Dmilk | Dext | Ding | |
|---|---|---|---|---|---|
| Västernorrland | Infant | 4.1 | 5.3 | 78.4 | 12.2 |
| Adult | 2.5 | 1.3 | 76.1 | 20.1 | |
| Dalarna | Infant | 63.0 | 5.9 | 26.9 | 4.1 |
| Adult | 52.7 | 2.0 | 35.9 | 9.4 | |
| Gotland | Infant | 30.3 | 48.5 | 18.8 | 2.5 |
| Adult | 34.7 | 23.0 | 34.4 | 7.9 |
The age dependence of Dth,tot is illustrated in three of the counties studied in figure 3. In the case of Gotland, the initial dip between infants and 1-year-olds at the onset of Chernobyl fallout is an effect of the way in which the model takes the 131I intake of infants being breastfed into account. This discontinuity in the model will be pronounced in a region such as Gotland, where the cmilk values were substantially higher in relation to the ground deposition Aesd than in other regions in Sweden.
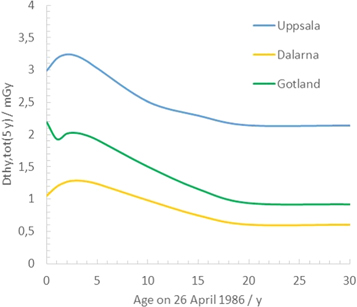
Figure 3. Time-integrated total absorbed dose to the thyroid, Dth,tot(5 y) in three Swedish counties as a function of age at the time of the Chernobyl NPP accident.
Download figure:
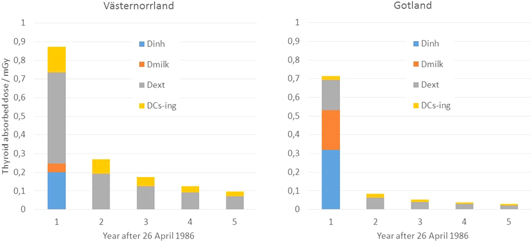
Standard image High-resolution imageThe time dynamics of the various components in the total absorbed dose to the thyroid according to the model developed in this study for Västernorrland and Gotland is illustrated in figure 4. It is evident that in the 5-year period after the accident the contribution from Dext dominates over Dinh, Dmilk, and DCs-ing in Västernorrland, while in Gotland Dinh is the main thyroid dose contributor during the first year after the fallout. This is explained by the early arrival of the Chernobyl plume combined with the consideration that the grazing cows in Gotland were not brought in, as it was not realised that the accident had taken place until the fallout reached the mainland.
{kind=link}
{kind=link}
{kind=link}
Figure 4. Time-integrated absorbed dose to the thyroid in adults resulting from inhalation, Dinh, consumption of 131I in milk, Dmilk, external exposure, Dext, and ingestion through food contaminated with 134Cs and 137Cs, DCs-ing, in Västernorrland (left) and Gotland (right).
Download figure:
Standard image High-resolution image{kind=link}
3.3. Comparison of the results from the model with thyroid measurements
A number of thyroid measurements were carried out in Sweden just after the Chernobyl NPP accident that can be used to validate some of the predictions made by the proposed model. Measurement series of the 131I content in the thyroids of people living in the city of Gothenburg in the Västra Götaland region (Cederblad et al 1988) and in Malmö in the Skåne region (Ahlgren and Hemdal 1987) cover a significantly longer time period than other Swedish measurements (table 11). Plotting these data, and calculating the integrated activity of the 131I content in the thyroid, combined with the S-factor for the absorbed dose to the thyroid (given by Snyder et al 1975) yielded an estimated absorbed dose to the thyroid of 0.037 mGy for adults and 0.046 mGy for children (1–7 years old). These values can be compared with the sum of the values of Dinh and Dmilk calculated with our model, which gives a value about a factor of 2 higher for adults (0.085 mGy), and a factor of 3 higher for 4-year-olds (0.13 mGy).
Table 11. Comparison of values of Dinh + Dmilk (mGy) calculated by the model (16) with those obtained from measurements on residents in selected areas. Thyroid measurements in Stockholm, Gotland, and Västerbotten were made in especially exposed groups, and may therefore not be representative of the adult population in these areas, whereas thyroid measurements in Gothenburg and Malmö represent the general adult population in these cities.
| Area | Dinh + Dmilk(model) | Thyroid measurements (range) | Dth,tot (5 y) using measured Dinh + Dmilk values and model estimates of Dext and Ding |
|---|---|---|---|
| Gothenburg, city (Cederblad et al 1988)a | 0.085 | 0.038–0.054 | (0.04–0.15) + 0.18 |
| Gothenburg, city (Andersson and Nyholm 1986) | 0.10–0.15 | ||
| Malmö, city (Ahlgren and Hemdal 1987)b | 0.16 | 0.050–0.087 | (0.05–0.09) + 0.19 |
| Stockholm, city (Andersson and Nyholm 1986) | 0.37 | 0.12–0.19 | (0.12–0.19) + 0.28 |
| Gotland, region (Andersson and Nyholm 1986) | 0.53 | 2.7–4.4 | (2.7–4.4) + 0.35 |
| Västerbotten, region (Olofsson and Svensson 1988) | 0.06 | 0.37c (0–3.7) | (0–3.7) + 1.40 |
aDinh and Dmilk are based on regional average values for the region of Västra Götaland. bDinh and Dmilk are based on regional average values for the region of Skåne. cAverage for people not drinking rainwater and living in areas with Aesd between 10 and 40 kBq/m−2.
It is also interesting to validate the other contributions to Dth,tot. The contribution to the internal dose to the thyroid from the ingestion of radiocaesium, Ding (12), calculated with the model can be compared with whole-body measurements of 137Cs carried out during the first year after the Chernobyl NPP accident in residents of Gothenburg (these values were obtained from a national database provided by SSM). The value of Ding was extracted from these data. It was found that the Ding value calculated by the model underestimated the observed values by 37%. However, when integrating over a 5-year period, the difference decreased to less than 20%. Consequently, in the case of residents of Gothenburg it appears that the proposed model does not underestimate the 131I contribution, and does not overestimate the Cs-related contribution to Dth,tot.
Assessing the Swedish measurement series further, the model appears to overestimate the sum of Dinh and Dmilk for the three largest urban regions in Sweden (Stockholm, Gothenburg, and Malmö), (see table 11). For Gotland, however, this sum is underestimated by the model when using the regional averages of Dinh given by Finck et al (1992) and the dairy milk data from Gotland, Dmilk. The high thyroid dose to the residents of Gotland is not explained by the higher dairy milk concentrations alone, but also by the higher initial inhalation dose, Dinh, compared to elsewhere in Sweden. However, comparison is difficult as these measurements were only carried out during a few days around 16 May 1986, and the individuals chosen for the measurements were those deemed to be especially susceptible to iodine uptake (e.g. outdoor workers and high milk consumers). A considerable difference was also found between the model prediction and observed Dinh + Dmilk values for Västerbotten (table 11). However, the data are from residents from highly contaminated areas, and they are not necessarily representative of the value of Einh over the whole region, which also makes comparison difficult.
A coarse uncertainty assessment of Dth,tot(5 y) was performed by using the random number generator in a standard spreadsheet (MS Excel), and assuming a rectangular probability density function (pdf) between a minimum and maximum value around the central estimate of the variables in (18). Repeating the calculations, e.g. more than 100 times, gives a prediction of the pdf for Dth,tot(5 y). A rectangular pdf in the interval of ±5% of the central estimate was used for f134/137 and ±10% for w(age), ∅_(Kerma/H) (600 keV), kSEQ,ROT, kth, and Fsnow (for counties with a central estimate of Fsnow < 0.9). Intermediate interval lengths of ±20% of the central estimate were set for a(age), kdelay, Adep,local, dCs, kth/E, eing(age), r(t), fout, fshield, fsex, and the transfer to mothers milk (both 131I and 137Cs). The largest intervals, ±50% of the central estimate, were set for Einh, F(age), cmilk,I-131, and Tag (both for 134Cs and 137Cs). N.B. that these pdfs refer to the esteemed confidence in the regional average in terms of area and age cohorts.
For the most affected region (Västernorrland county) it was found that the simulated Dth,tot(5 y) for newborns (average over males and females) spanned from 2.9–5.2 mSv (5th–95th percentile). For the region of Gotland the corresponding value of Dth,tot(5 y) ranged from 1.6–3.0 mSv. This result indicates that the regional averages of Dth,tot may vary by almost a factor of 2. This applied also for the simulated range of the mean value for the 131I dominating component of Dth,tot (=the sum of Dinh and Dmilk), for adults in the two regions Skåne and Västra Götaland is found to be 0.088–0.25 mSv (5th–95th percentile) and 0.050–0.12 mSv, respectively. Comparing these values with the observed mean thyroid 131I absorbed dose in adults made in the cities of Malmö (Skåne county) and Gothenburg (Västra Götaland county) (table 11), and here deemed the most extensive thyroid data available in Sweden in terms of follow-up over time, it is found that the observed mean values agree with the 5th percentile level of the model predictions. Thus, the aforementioned discrepancies for the iodine dominating components of Dth,tot are most likely associated with the large uncertainties in regional averages of inhalation dose, Einh, and ingestion of 131I through milk, cmilk. The influence of the uncertainty of a majority of the parameters in (18) on the prediction of long-term absorbed dose from a nuclear power plant fallout is more extensively explored in Isaksson et al (2019).
4. Discussion
We have developed a model for calculating the 5-year time-integrated total absorbed dose to the thyroid in individuals of varying age after a nuclear accident, including the dose contribution from short-lived radionuclides (131I, 132I, and 132Te) through milk consumption and inhalation, and the external and internal dose contributions from the more long-lived nuclides 134Cs and 137Cs. This model can be applied to populations living under conditions similar to those in Sweden after 1986. Interestingly, the results suggest that the contribution from the inhalation and ingestion of short-lived radionuclides accounts for less than half of the total thyroid dose in most of the Swedish counties studied. Therefore, reducing the intake of radioiodine in order to reduce the dose to the thyroid might not be sufficient to prevent future cases of thyroid cancer, especially in areas affected by wet deposition and areas remote from the release point of the fallout.
The intake of stable iodine is nowadays used to block the uptake of radioiodine after a nuclear accident, not only for the purpose of avoiding acute effects, but also to prevent thyroid cancer in the future. Prompt intake of stable iodine is considered of key importance, especially in areas close to the release point, to avoid an anticipated thyroid dose from radioiodine due to inhalation and/or through the food chain, mainly contaminated milk. At greater distances, however, where enhanced deposition is mainly due to wet deposition, 134,137Cs may account for the main contribution to the dose to the thyroid. Administering stable iodine may then not be as efficient in preventing future cases of thyroid cancer.
Modelling the combined contributions of internal and external exposure to the dose to the thyroid is important in cases of extensive nuclear fallout, and the model presented here may provide indications of the magnitude of the respective contributions to the total absorbed dose to the thyroid. Efforts were made to estimate the various contributions in terms of absorbed organ dose, rather than in terms of risk-related quantities, such as equivalent dose (ICRP 1991, 2007). However, the use of this model may be limited in epidemiological studies, as it incorporates two equivalent dose coefficients (einh and eing), which were originally intended for radiation protection purposes, and may, therefore, be overly conservative. Furthermore, the relative contribution from the dietary intake of 131I in milk will depend not only on the daily intake, but will also vary widely depending on which remedial measures are taken in connection with a radioactive release, as well as when in the growth season the event takes place. In the present study, only 131I transfer through milk was considered in the estimation of doses attributed to radioiodine ingestion, which may lead to underestimation of the contributions from the ingestion of 131I from other contaminated foodstuffs such as leafy vegetables. However, the estimated average absorbed thyroid doses resulting from time-integrated 131I intake through milk appear to agree with the generic estimates for 1 y ingestion presented by Drozdovitch et al (2007).
When comparing the results obtained with our model with existing thyroid measurements in Sweden, it appears that the model slightly overestimates the contribution to the dose to the thyroid from radioiodine by inhalation (Dinh) and from milk (Dmilk) in the three most populated counties. A striking contrast is Gotland, where measurements performed on 16 May 1986, which were scaled and extrapolated after the observations made by SSM in Stockholm, gave values of Dinh + Dmilk one order of magnitude higher than predicted by the model. We believe that this can be explained by the coarse regional averages of inhalation doses which were extrapolated geographically from six different air sampling stations located over the whole country (Finck et al 1992), which did not account for the high 131I air concentration over Gotland, which was one of the first areas affected by the Chernobyl fallout. The difference found for Västerbotten is, however, more likely to be caused by the fact that the population on which measurements were made were close to the border with Västernorrland, where the deposition was considerably higher than the regional average for Västerbotten. A detailed reconstruction of air trajectories during the first 10–20 days after the event on 26 April 1986 would be needed to obtain a more precise estimate of the initial doses due to inhalation, Dinh. The uncertainties associated with the model are, however, considered to be within a factor of 2 for the majority of residents of Sweden, and the assumption of a value of kth/E of 20 will ensure some conservatism, apart from the extreme case of Gotland.
According to our model, uptake of 131I by means of inhalation and milk consumption, gives a 5-year time-integrated thyroid dose (Dinh + Dmilk) of up to 1.7 mGy in infants in Sweden (table 9), which is about 1000 times less than the corresponding value estimated for the region of Gomel in Belarus, one of the most heavily affected areas in terms of thyroid exposure resulting from the Chernobyl fallout. The region of Gomel received, on average, 1–4 MBq m−2 of 137Cs as ground deposition, which is about 100 times higher than the regional average 137Cs ground deposition in the areas studied in this work (table 1). Scaling up the Swedish values of Dinh, Dmilk, Dext, and Ding, assuming similar ground deposition of 137Cs and similar radioiodine uptake through inhalation and milk consumption as in Gomel, would result in a contribution from Dinh + Dmilk of 1000 mGy. The contribution of DCs-ing and Dext to Dth,tot(5 y) would be in the range of 100–400 mGy, and the average contribution to the 5-year time-integrated absorbed dose to the thyroid from exposures not related to the uptake of radioiodine would be between 10% and 40% (table 10). Assuming a similar radioecological transfer for rural Belarusian residents as for the urban Swedish population, and a similar ecological half-time for migration processes (governing the ground penetration and the external dose contribution from the ground deposition of 134,137Cs), it is hypothesised that up to 40% of the 5-year time-integrated thyroid absorbed dose has arisen from non-131I-related exposures, based on the deposition values from Belarus. However, according to Drozdovitch et al (2010), the contribution from external radiation to the thyroid absorbed dose is less than 5%, and the Cs-ingestion values are even lower (<1%) for infants and children. These values appear rather low in proportion to the average 137Cs deposition in these areas, as compared with our model predictions.
The impact of the external dose and Cs ingestion on Dth,tot can also be illustrated by comparing data from Bernhardsson et al (2011) and Ramzaev et al (1996). In the region of Bryansk the time-integrated external effective dose between 1986 and 1991 was about 70 mSv. The average total activity deposition of 1.3 MBq m−2 137Cs in the Bryansk region (Bernhardsson et al 2011) can be translated into a surface equivalent deposition, Aesd, of 0.8 MBq m−2 by multiplying it by a factor of (1/1.6). This factor is based on an empirical relationship between the total activity deposition measured by means of soil sampling and the corresponding value obtained from airborne measurements (Edvarson 1991). With Aesd = 0.8 MBq m−2 our model predicts a value of Dext(5 y) of 76 mGy for adults and 99 mGy for infants (average of both sexes), which is in reasonable agreement with the Russian data. Furthermore, these values can be compared with the average thyroid absorbed dose from 131I of 246 mGy in the Bryansk region (Shaktarin et al 2003). Evidently, our model predicts an at least 30% additional contribution from the external radiation to the thyroid absorbed dose, not considered in the estimates by Shaktarin et al (2003). When the internal dose from 134,137Cs ingestion in contaminated foodstuff is included, our model predicts an additional 10% contribution to the 246 mGy thyroid absorbed dose.
Although the proposed model appears to predict values of Dth,tot that can be validated by measured data in Sweden, it underestimates the contribution to Dth,tot due to radioiodine over one of the regions investigated (Gotland). The airborne Chernobyl fallout reached this region first, albeit without any major precipitation, leading to relatively low ground deposition of 137Cs (Adep = 3.1 kBq m−2) compared with regions with wet deposition, such as Västerbotten (Adep = 28.4 kBq m−2). If the local air concentration of radioiodine in Gotland was higher than for the nearest air filter station situated in the mainland (Studsvik) this will lead to substantial underestimations of the doses due to inhalation, Dinh. Thus, due to the low Adep value and the subsequently lower dose due to external irradiation, Dext, it is therefore expected that the relative proportion of Dinh to the 5-year time-integrated absorbed dose to thyroid is underestimated as well. These findings warrant further studies on methods of retrospectively reconstructing inhalation doses to the residents of Gotland during the days and weeks after the Chernobyl fallout, for example, using historical records of meteorological data. Studies should also be carried out to determine whether such local variations in inhalation doses explain the somewhat low relative radiocaesium-attributed component of thyroid doses reported elsewhere for Eastern European populations.
5. Conclusions
We have presented a radioecological model in which various exposure pathways to the thyroid can be combined in order to estimate the 5-year time-integrated total absorbed dose to the thyroid, including dose contributions from inhalation, ingestion of radioiodine in milk, external exposure and ingestion of radiocaesium after a Chernobyl-type nuclear power plant release. The estimates for fictive residents in Sweden indicate that the external dose and the ingestion of 134,137Cs may contribute most to the time-integrated total absorbed dose to thyroid in a situation with low contamination of milk by radioiodine, except in areas with predominantly dry 131I deposition and low ground deposition of 137Cs. This study also indicates that the non-radioiodine-related contribution to the thyroid dose may have been overlooked in previous studies in areas mainly affected by wet deposition. Therefore, we believe non-radioiodine contributions to the thyroid dose should be addressed in future epidemiological studies and the follow-up of inhabitants affected by releases from a nuclear power plant accident.
One limitation of this study is that the proposed model relies on manually integrated dairy milk data, instead of a generic transfer factor between the ground deposition of 131I and 131I ingested by milk consumption. In addition, the precision in the prediction of the dose to the thyroid could be improved by using data on inhalation doses to inhabitants with higher geographical resolution, and data on 131I concentrations in the dairy milk that actually reached consumers in the affected counties. However, our model seems to predict the absorbed dose to the thyroid with sufficient precision at a population level when validated by thyroid measurements in Sweden, and when compared with published thyroid absorbed dose estimates from other countries. Further studies are required to investigate the possibility of developing a similar type of radioecological model for the transfer of ground-deposited radioiodine to man, as has been done for radiocaesium (e.g. Rääf et al 2006, Isaksson et al 2018). However, simplified generic modelling will never be suitable to predict the main contributions to the thyroid dose during the first days after a nuclear power plant accident, since the inhalation doses in a release event will depend on the local weather conditions, and the extent to which residents in the affected area can comply with recommended sheltering and administration of stable iodine.
Acknowledgements
The authors acknowledge the input made by Asst Prof Robert Wålinder and Dr Robert Finck. The authors also acknowledge all experts involved at the universities, the Swedish Radiation Protection Authority and the Swedish Defence Research Institute, whose thorough records of relevant radiometry data in the initial phase of the Chernobyl fallout in Sweden now can contribute to modelling and future predictions of radiation exposures in connection with nuclear releases.