
Abstract
Objective
Pressure Support Ventilation (PSV) is now widely used in the process of weaning patients from mechanical ventilation. The aim of this study was to evaluate the effects of various levels of PS on respiratory pattern and diaphragmatic efforts in patients affected by chronic obstructive pulmonary disease (COPD).
Setting
Intermediate intensive care unit.
Patients
We studied ten patients undergoing PSV and recovering from an episode of acute respiratory failure due to exacerbation of COPD.
Methods
Three levels of PSV were studied, starting from the lowest (PSb) one at which it was possible to obtain an adequate Vt with a pH≥7.32 and an SaO2>93%. Then, PS was set at 5 cmH2O above (PSb+5) and below (PSb-5) this starting level. Ventilatory pattern, transdiaphragmatic pressure (Pdi), the pressure-time product of the diaphragm (PTPdi), the integrated EMG of the diaphragm, static PEEP (PEEPi, stat), dynamic PEEP (PEEPi, dyn), and the static compliance and resistance of the total respiratory system were recorded.
Results
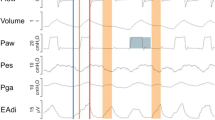
Minute ventilation did not significantly change with variations in the level of PS, while Vt significantly increased with PS (PS−5=6.3±0.5 ml/kg vs. PSb=10.1±0.9 [p<0.01] and vs. PS+5=11.7±0.6 [p<0.01]), producing a reduction in respiratory frequency with longer expiratory time. The best values of blood gases were obtained at PSb, while at PSb−5, PaCO2 markedly increased. During PSb and PSb+5 and to a lesser extent during PSb−5, most of the patients made several inspiratory efforts that were not efficient enough to trigger the ventilator to inspire; thus, the PTPdi “wasted” during these inefficient efforts was increased, especially during PS+5. The application of an external PEEP (PEEPe) of 75% of the static intrinsic PEEP during PSb caused a significant reduction in the occurrence of these inefficient efforts (p<0.05). Minute ventilation remained constant, but Vt decreased, together with Te, leaving the blood gases unaltered. The PTPdi per breath and the dynamic PEEPi were also significantly reduced (by 59% and 31% of control, respectively,p<0.001) with the application of PEEPe.
Conclusion
We conclude that in COPD patients, different levels of PSV may induce different respiratory patterns and gas exchange. PS levels capable of obtaining a satisfactory equilibrium in blood gases may result in ineffective respiratory efforts if external PEEP is not applied. The addition of PEEPe, not exceeding dynamic intrinsic PEEP, may also reduce the metabolic work of the diaphragm without altering gas exchange.
Article PDF
Similar content being viewed by others

Avoid common mistakes on your manuscript.
References
Brochard L, Pleskwa F, Lemaire F (1987) Improved efficacy of spontaneous breathing with inspiratory pressure support. Am Rev Respir Dis 136: 411–415
Brochard L, Harf A, Lorino H, Lemaire F (1989) Inspiratory pressure support prevents diaphragmatic fatigue during weaning from mechanical ventilation. Am Rev Respir Dis 139:513–521
MacIntyre NR, Leatherman NE (1990) Ventilatory muscle loads, and the frequency-tidal volume pattern during inspiratory pressure-assisted (pressure-supported) ventilation. Am Rev Respir Dis 141:327–331
Marini JJ (1986) Exertion during ventilator support: how much and how important? Respir Care 31:385–387
Braun NMT, Faulkner J, Hughes RL, Roussos C, Sahgal V (1983) When should respiratory muscles be exercised? Chest 84:76–84
Kimura T, Takezawa J, Nishiwaki K, Shimada Y (1991) Determination of the optimal pressure support level evaluated by measuring transdiaphragmatic pressure. Chest 100:112–117
McIntyre NR, Nishimura M, Usada Y, Tokioka H, Takezawa J, Shimada Y (1990) The Nagoya conference on system design and patient-ventilator interactions during pressure support ventilation. Chest 97:1463–1466
Pepe PE, Marini JJ (1982) Occult positive end-expiratory pressure in mechanically ventilated patients with airflow obstruction: the auto-PEEP effect. Am Rev Respir Dis 126:166–170
Marini JJ (1989) Should PEEP be used in airflow obstruction? Am Rev Respir Dis 140:1–3
Field S, Grassino A, Sanci S (1984) Respiratory muscle oxygen consumption estimated by the diaphragm pressure-time index. J Appl Physiol 57:44–51
Gattinoni L, Pesenti A, Avalli L, Rossi F, Bombino M (1987) Pressure-volume curve of total respiratory system in acute respiratory failure. Am Rev Respir Dis 136:730–736
Ranieri MV, Eissa NT, Corbeil C, Chasse M, Braidy J, Matar N, Milic-Emili J (1991) Effects of PEEP on alveolar recruitment and gas exchange in ARDS patients. Am Rev Respir Dis 144:544–551
Milic-Emili J, Mead JJ, Turner JD, Glauser FM (1964) Improved technique for studying pleural pressure from esophageal balloons. J Appl Physiol 13:207–211
Baydur A, Behrakis PK, Zin WA, Jaeger MJ, Milic-Emili J (1982) A simple method for assessing the validity of the esophageal balloon technique. Am Rev Respir Dis 126:788–791
Petrof BJ, Legare M, Goldberg P, Milic-Emili J, Gottfried SB (1990) Continuous positive airway pressure reduces work of breathing and dyspnea during weaning from mechanical ventilation in severe chronic obstructive pulmonary disease. Am Rev Respir Dis 141:281–289
Rochester DF, Bettini G (1976) Diaphragmatic blood flow and energy expenditure in the dog: effects of inspiratory airflow resistance and hypercapnia. J Clin Invest 57:661–672
Whitelaw WA, Derenne JP, Milic-Emili J (1975) Occlusion pressure as a measure of respiratory center output in conscious man. Respir Physiol 23:181–199
Stradling JR, Chadwick GA, Quirk C, Phillips T (1985) Respiratory inductance plethysmography: calibration, techniques, their validation and the effects of posture. Bull Eur Physiopathol Respir 21:317–324
Rossi A, Gottfried SB, Zocchi L, Higgs BD, Lennos S, Calverley PMA, Begin P, Grassino A, Milic-Emili J (1985) Measurement of static compliance of the total respiratory system in patients with acute respiratory failure during mechanical ventilation. Am Rev Respir Dis 131:672–677
Bates JHT, Rossi A, Milic-Emili J (1985) Analysis of the behaviour of the respiratory system with constant inspiratory flow. J Appl Physiol 64: 441–450
Rubini F, Rampulla C, Nava S (1994) Acute effect of corticosteroids on respiratory mechanics in mechanically ventilated patients with chronic airflow obstruction and aucte respiratory failure. Am J Respir Crit Care Med 149:306–310
Kochi T, Okubo S, Zin WA, Milic-Emili J (1986) Flow and volume dependence of pulmonary mechanics in anesthetized cats. J Appl Physiol 64:441–450
Fernandez R, Benito S, Blanch L, Net A (1988) Intrinsic PEEP: a cause of inspiratory muscle ineffectivity. Intensive Care Med 15:51–52
Ranieri M, Giuliani R, Cinella G, Pesce C, Brienza N, Ippolito EL, Pomo V, Fiore T, Gottfried SB, Brienza A (1993) Physiologic effects of positive end-expiratory pressure in patients with chronic obstructive pulmonary disease during acute ventilatory failure and controlled mechanical ventilation. Am Rev Respir Dis 147:5–13
Fernandez Mondejar E, Vazquez Mata G, Navarrette Navarro P, Rivera Fernandez R, Torres Ruiz JM, Carazo E (1992) Increase in lung volume originated by extrinsic PEEP in patients with auto-PEEP. Intensive Care Med 18: 269–273
Armitage P (1980) Statistical methods in medical research. Wiley, New York
MacIntyre NR (1986) Respiratory function during pressure support ventilation. Chest 89:677–686
Prakash O, Meij S (1985) Cardiopulmonary response to inspiratory pressure support during spontaneous ventilation vs. conventional ventilation. Chest 88:403–408
Tuxen DV (1989) Detrimental effects of positive end-expiratory pressure during controlled mechanical ventilation of patients with severe airflow obstruction. Am Rev Respir Dis 140:5–9
Martin JG, Shore S, Engle LA (1982) Effect of continuous positive airway pressure on respiratory mechanics and pattern of breathing in induced asthma. Am Rev Respir Dis 126:812–817
Widdicombe J (1963) Reflex effects of lung inflation in tracheal volume. J Appl Physiol 18:681–686
Petrof BJ, Calderini E, Gottfried S (1990) Effect of CPAP on respiratory effort and dyspnea during exercise in severe COPD. J Appl Physiol 69:179–188
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Nava, S., Bruschi, C., Rubini, F. et al. Respiratory response and inspiratory effort during pressure support ventilation in COPD patients. Intensive Care Med 21, 871–879 (1995). https://doi.org/10.1007/BF01712327
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01712327