
Abstract
The use of single-photon emission computed tomography/computed tomography (SPECT/CT) for sentinel node (SN) detection has been evaluated in the majority of malignancies with predominantly superficial lymphatic drainage. In breast cancer and melanoma, important initial contributions of SPECT/CT were based on the anatomical localisation of SNs already visualised on planar images, the detection of additional SNs in aberrant basins, and the depiction of SNs in cases with no visualisation on planar images. However, more recently, the finding that SPECT/CT use is associated with a higher rate of SN detection, more metastatic SNs, and a higher rate of disease-free survival in large series of patients is leading SPECT/CT to be routinely performed in melanoma. The incorporation of SPECT/CT into the SN procedure in melanoma also appears to be cost effective and was significantly related to shorter operative times, shorter hospital stays, and fewer complications. In penile and vulvar cancer, the use of SPECT/CT has led to the detection of additional SNs. In oral cavity cancer and thyroid cancer, SPECT/CT not only appears to be useful for planar image interpretation but is also becoming an essential component of the SN procedure, providing surgeons with additional anatomical information. As regards malignancies with deep lymphatic drainage, SPECT/CT has been extensively validated in urological and gynaecological cancers. In these malignancies, SPECT/CT was able to localise SNs not only in the basins included in the area of extended pelvic lymph node dissection but also in aberrant locations. In gastrointestinal and lung malignancies, SPECT/CT has been used only incidentally. SPECT/CT must be considered complementary to planar lymphoscintigraphy for SN identification, and a combined interpretation of both modalities is necessary. With the improvement of the CT component, nuclear physicians today can also identify lymph nodes corresponding to radioactive SNs. This visual information is helpful for the intraoperative procedure and for post-excision assessment using portable devices.
Similar content being viewed by others



Avoid common mistakes on your manuscript.
Introduction
When Donald Morton introduced the modern sentinel node (SN) concept in 1992, he also presented methodological aspects of the procedure in patients with melanoma [1]. This initial approach involved the injection of blue dye prior to skin excision and surgical search for SNs in the expected basin of drainage. In 1993, radiocolloids and intraoperative gamma probes were added to the procedure, making it possible to use acoustic signals for SN detection in the operating room [2]. Through the use of radiocolloids, preoperative imaging using lymphoscintigraphy became possible and, principally in Europe, this approach, involving radiotracer injection and skin marking of the identified SNs the day before surgery, became incorporated into daily practice [3]. Therefore, lymphoscintigraphy may be regarded as the first roadmap for surgeons, allowing preoperative determination of lymphatic drainage and SN localisation. This preoperative lymphatic mapping was reinforced a few years later by the incorporation of single-photon emission computed tomography/computed tomography (SPECT/CT) into the SN procedure. Using this modality, it was possible to establish anatomical landmarks to facilitate the localization of SNs. The functional information obtained from SPECT could be combined with the morphological information from CT, applying both the techniques in the same session. The resulting fused SPECT/CT images were able to depict SNs in an anatomical landscape, thereby adding a dimension to the surgeon’s roadmap.
The use of SPECT/CT depends on the complexity of the lymphatic drainage. In malignancies with predominantly superficial drainage (e.g. melanoma and breast cancer), the technique has been validated for specific indications, such as when SNs in the axilla are not depicted on planar images or when the overlying injection site masks lymph nodes that are located in its vicinity. SPECT/CT may also be helpful in patients with unusual or complex drainage, as observed in melanomas of the neck or the upper part of the trunk and in breast cancer in patients presenting drainage outside the axilla.
In tumours with complex lymphatic drainage, such as gynaecological and urological malignancies, SPECT/CT is becoming mandatory to localise SNs in difficult anatomical areas such as the pelvis and abdomen. Also, in patients with oral cavity cancer and papillary thyroid carcinoma, SPECT/CT contributes to SN identification in the neck basins.
This review discusses published papers in which the systematic use of SPECT/CT in the SN procedure was evaluated. The PubMed database was searched for studies concerning the use of SPECT/CT for lymphatic mapping. The following medical subject headings (MeSH terms) were used to find relevant articles: breast neoplasms, melanoma, sentinel lymph node biopsy, tomography, gynaecology, urology, oral cavity, emission-computed, single-photon. Papers using only SPECT were excluded, as were case reports.
SPECT/CT in malignancies with predominantly superficial lymphatic drainage
Cutaneous melanoma
In cutaneous melanoma, lymphatic drainage from primary lesions located in the extremities is highly predictable, and the inguinal or axillary basins are the expected areas of drainage. In the groin, SNs are mostly superficial and located below the inguinal ligament, whereas in some cases there is direct drainage to Cloquet’s node or to the obturator or iliac nodes, bypassing the superficial lymph nodes. Primary lesions located in the posterior area of the foot or leg may drain to popliteal SNs. For primary lesions of the upper extremities, SNs are frequently located in level I of the axilla; however, aberrant drainage to epitrocheal/epicondyleal or supraclavicular SNs may also occur when primary lesions are located in the hand or forearm. In the trunk, melanomas of the flank may drain to the groin and/or to the axilla. The variability in drainage is higher for trunk melanomas than for melanomas of the extremities and for dorsal locations it can be as high as 60 %. For instance, melanomas of the scapular region often drain to the axilla, but SNs can also be present in the supraclavicular fossa or in the intermuscular space of the shoulder.
Against this background, SPECT/CT in melanoma has been validated for specific indications. An initial study demonstrated that SPECT/CT had added value in 30 out of 85 patients (35 %), by detecting extra SNs, not visualised on planar images, by localising SNs in other basins, or by modifying the surgical incision planning. In seven patients, 12 additional SNs were detected, and in two of them the SN contained metastases [4]. In another study, concerning 18 melanoma patients, a visualisation rate of 100 % was found for SPECT/CT versus 89 % for planar lymphoscintigraphy; furthermore, SPECT/CT also provided additional anatomical information leading to an adjustment of the surgical approach in four patients [5]. These findings were confirmed in another series including 35 melanoma patients; SPECT/CT detected additional SNs in seven of them and contributed to modify the surgical approach in ten [6]. More recently, SPECT/CT and planar lymphoscintigraphy detected SNs in 32 patients, both techniques having a visualisation rate of 97 %; however, SPECT/CT contributed to the decision to adjust the surgical approach in 12 patients [7]. In another study including 113 melanoma patients, SPECT showed a clearly higher (95 %) SN detection rate than planar lymphoscintigraphy (89 %); SPECT/CT was able to visualise lymphatic drainage in eight patients without SN visualisation on planar images [8].
Most studies applying SPECT/CT in melanoma have sought to estimate its contribution to SN detection. However, from the clinical practice perspective, the additional value of SPECT/CT in adjusting the surgical approach has probably been more important. Such additional value was reported in 14 out of 63 (22 %) melanoma patients, whereas the SN visualisation rate on a patient basis was not significantly different between planar lymphoscintigraphy (98 %) and SPECT/CT (100 %) [9]. Recently, the global contribution of SPECT/CT in melanoma was established in a study comparing the results of 149 patients submitted to SPECT/CT with those of a group of 254 patients who did not undergo SPECT/CT. Not only did SPECT/CT detect more SNs (average 2.4 versus 1.87 without SPECT/CT) and more metastatic SNs (average 0.34 versus 0.21), its use was associated with a significantly higher rate of four-year disease-free interval (93.9 %) when compared with the group of patients not submitted to SPECT/CT (79.2 %) [10]. The same group of investigators evaluated the cost effectiveness of the use SPECT/CT in combination with planar lymphoscintigraphy. When SPECT/CT was incorporated into the preoperative imaging, its use was associated with a mean cost reduction of €710.50 (30.5 %); this was achieved mainly through shorter operative times and hospital stays. The addition of SPECT/CT also led to a significant reduction of postoperative morbidity [11].
Breast cancer
The axilla is the principal area of lymphatic drainage from breast cancer. Although axillary SNs are mostly located in level I, direct lymphatic drainage to level II or level III may be observed. In a minority of patients, SNs may also be found in the internal mammary chain, as well as in supraclavicular, intramammary and/or interpectoral locations. Lymphatic drainage outside the axilla is principally seen when tracer injection is peritumoural or intratumoural.
In a study involving 134 patients receiving intratumoural tracer injection, SPECT/CT, by detecting extra SNs or by modifying the surgical incision planning, demonstrated additional value in 48 of them (42 %). In 15 patients, 19 additional SNs were visualised by SPECT/CT not just in the axilla but also in interpectoral and intramammary locations. Four of these SNs contained metastases. The SPECT/CT information led to a more precise or an additional incision [12]. In another series including 41 patients, SPECT/CT led to accurate anatomical SN localisation in the axilla differentiating between levels I, II and III [13]. The use of SPECT/CT for the identification of SNs in overweight/obese patients was one of the first clinical indications for this technique. In a study including 122 patients scheduled for the SN procedure, SPECT/CT led to the detection of SNs in 29 out of 49 obese patients (59 %) in whom no SNs had been visualised on planar images [14]. In another study of 157 patients with breast cancer, SPECT/CT showed a 95 % visualisation rate and important complementary information was provided by the detection of SNs in patients with negative planar findings, the detection of additional drainage basins, and the identification of false-positive findings on planar images [15]. Also, the low-dose CT component of SPECT/CT was found to be helpful in detecting lymph node abnormalities in the drainage basin; a lymph node was considered positive if one out of four criteria for abnormality were seen: node size >10 mm in axial transverse diameter, irregular borders, round shape, and inhomogeneous structure. Applying these criteria, low-dose CT yielded 36 % sensitivity in 51 patients, with a 50 % positive predictive value and 69 % diagnostic accuracy for axillary staging [16]. In the same study, the number of SNs visualised by SPECT/CT and low-dose CT was discrepant in 13 patients, with more lymph nodes seen on CT.
In a more extensive series of 741 patients, SPECT/CT was used to study axillary SN locations. A SN was found in the axilla in almost 98 % of the patients; just under 50 % of these SNs were located in the mid or posterior group of level I and not in the anteropectoral group, traditionally considered the expected basin of axillary drainage of the breast [17].
The role of SPECT/CT as a valuable tool for SN localisation, especially in difficult cases when planar lymphoscintigraphy shows no SN or unexpected drainage, was recently emphasised in a systematic review that included 11 studies published since 2006. Limitations of SPECT/CT include extra acquisition time, inconvenience for the patient as well as additional radiation dose [18].
Head and neck malignancies
The lymphatic system in the head and neck includes approximately 250–300 lymph nodes divided into various nodal groups. This high lymph node density is one of the principal causes of the marked variations in lymphatic drainage. Another important factor explaining the high variability of drainage is the site of the primary lesion. For instance, scalp melanomas of the frontal zone can drain to different lymph nodes when compared with melanomas of the parietal or occipital areas. In the case of primary lesions located at the face and the forehead, drainage to different basins may occur. In the oral cavity, malignancies of the lingual apex may drain to other groups in comparison with well-lateralised lesions in the tongue or floor of the mouth. Moreover, there exist certain pitfalls, such as poor performance in identifying true SNs in floor-of-the-mouth carcinomas. In such tumours, the SNs may be masked because of radioactive scattering from the primary injection site, resulting in a reduction of the detection rate from 96 to 88 %, a decrease in sensitivity from 97 to 80 %, and a reduction in the negative predictive value from 98 to 88 %, respectively, as confirmed in the multicentre ACOSOG-Z0360 trial. Due to these factors, SPECT/CT appears to be essential not only to accurately identify SNs in an anatomical landscape, but also to detect additional SNs in the vicinity of the primary lesions or in patients with aberrant drainage to different lymph node basins. Following the introduction of SPECT/CT, some initial studies in oral cavity cancer, considering the number and location of visualised hot spots, reported no advantage over tomographic imaging [19]. However, more recent studies using SPECT/CT with high-end CT components have shown advantages over planar imaging, with SPECT/CT found to be able to detect additional SNs and to achieve better anatomical localisation. In a series of 58 patients with oral or oropharyngeal carcinoma, 11 additional SNs were detected; one of these nodes contained metastases [20]. In another study involving 34 patients, extra SNs were found by SPECT/CT in 15 patients and in seven of these the anatomical level of SN location was reconsidered [21]. The superior anatomical information provided by SPECT/CT may lead to modification of the surgical approach as shown in 11 out of 38 patients (29 %) with head and neck melanoma; in six of these 38 patients, SPECT/CT detected additional SNs (16 %) [22]. In another study, SPECT/CT modified the surgical approach (more superficial incision or incision at other site) in 9 out of 34 (27 %) patients with head and neck malignancies [23]. The surgical adjustment rate due to additional information from SPECT/CT increases when SNs are located in the periparotid areas; in eight out of 14 patients (57 %) with melanoma and drainage to the parotid region on planar lymphoscintigraphy, SPECT/CT was able to distinguish SNs in level II of the neck from those located in or around the parotid [24]. SPECT/CT anatomical information was also used to adjust superselective prophylactic irradiation of the neck in a feasibility study including 10 patients with squamous cell carcinoma of head and neck [25].
Recently, SPECT/CT has been validated for SN identification in papillary thyroid cancer. In an initial study, SNs were identified in 19 out of 24 patients (79 %) using lymphoscintigraphy and SPECT/CT; the identification rate increased to 96 % during surgery involving the use of a hand-held gamma probe. Multidirectional drainage to both central and laterocervical compartments was seen in 50 % of the patients [26]. In another series including 23 clinically node-negative patients, the combined visualisation rate of lymphoscintigraphy and SPECT/CT was 91 %. The two patients without drainage were not SN-positive for metastases. Most SNs were located in level VI (83 %) and II (35 %) of the neck, whereas in four patients contralateral drainage was also noted [27].
Vulvar and penile cancer
In spite of extensive validation of the SN procedure in these two malignancies, SPECT/CT has been evaluated only in limited patient series. In a group of 14 patients with gynaecological cancers, SPECT/CT localised SNs in all of them; in a subgroup of seven patients with vulvar cancer, the SPECT/CT SN detection rate was 100 versus 85 % for planar imaging, with impact on treatment in one patient (14 %) [28]. In 10 patients with vulvar carcinoma, SPECT fused with CT/MRI, compared with planar lymphoscintigraphy, detected 12 additional SNs [29].
In a study in patients with penile cancer, SPECT/CT was used to analyse the lymphatic drainage of the malignancy and to evaluate the implications as regards the extent of inguinal lymph node dissection. In 50 patients, lymphatic drainage was visualised in 82 out of 86 clinically node-negative groins (95 %) scheduled for the SN procedure. All SNs were located in the medial superior (73 %), lateral superior (8.7 %) and central (18.3 %) inguinal zones on SPECT/CT. No lymphatic drainage to the inferior zones of the groin was seen which suggests that it may be possible to exclude these zones from a subsequent inguinal lymph node dissection in the case of a tumour-positive SN [30]. Lymphatic drainage can be blocked by extensive metastatic involvement of the SN with rerouting of lymph fluid to a “neo-SN”. This entity was studied using SPECT/CT in 17 penile cancer patients with unilateral palpable and cytologically proven inguinal metastases who were scheduled for the SN procedure in the N0 contralateral groin. On CT, the palpable node metastases could be identified in all 17 groins. Only four of these metastatic lymph nodes showed uptake of the radioactivity. In 10 patients, rerouting of lymphatic drainage to a neo-SN was observed: ipsilateral in nine cases, and contralateral in one patient [31].
SPECT/CT in malignancies with deep lymphatic drainage
Urological malignancies
Male and female urogenital malignancies located in the pelvis generally drain to lymphatic basins in the vicinity of the primary tumour. There are different nodal groups receiving lymphatic drainage from the pelvic structures: the external iliac nodes whose medial subgroup includes the obturator nodes, the internal iliac lymph nodes, and the nodes in the trajectory of the common iliac vessels. SNs from malignancies of the prostate, bladder, cervix and endometrium have been found in these iliac basins. However, aberrant drainage to the para-aortic and aortocaval lymph nodes as well as to SNs in the proximity of the sacrum and anterior abdominal wall is also possible.
SPECT/CT is particularly useful for anatomically localising SNs both in the expected drainage basins of the pelvis and in aberrant abdominal locations. In prostate cancer, SPECT/CT increased the SN visualisation rate from 91 % for planar scintigraphy to 98 %. In 46 patients, SPECT/CT also depicted more SNs than planar images did (average 4.3 versus 2.2 SNs); 44 % of the SNs containing metastases were visualised only by SPECT/CT [32]. In another evaluation, SPECT/CT identified SNs outside the area of extended pelvic lymph node dissection (often used to stage the pelvis) in 37 out of 121 prostate cancer patients (31 %). These SNs were found in different locations: presacral, Cloquet’s node, inguinal, para-aortic, abdominal wall, pararectal, behind the common iliac artery, and lateral to the external iliac artery [33]. In a study comparing treated and untreated prostate cancer patients, SPECT/CT revealed a higher percentage of SNs (80 versus 34 %) outside the pelvic para-iliac region in the treated cases [34]. In another series, SPECT/CT findings led to a 25 % impact of lymphatic drainage on conformal pelvic irradiation in 23 prostate cancer patients [35]. In a study designed to validate laparoscopic SN versus hyperextensive pelvic dissection for staging clinically localised prostate carcinoma, SPECT/CT identified SNs in 191 of 203 patients (94 %). Bilateral SNs were found in 159 patients (83 %) and unilateral ones in 32 (17 %). The most frequent drainage site was the common iliac region (31 %), followed by the internal iliac (20 %), the obturator fossa (18 %), the external iliac (15 %), and the promontory/presacral area (6 %) [36]. A similar presacral SN rate (5.4 %) was found in another study involving 18 patients with prostate cancer of intermediate prognosis; in this series, para-aortic (5.4 %), pararectal (5.4 %) and paravesical (3.6 %) SNs, too, were found outside the area of extended pelvic lymphadenectomy [37].
Drainage to lymph nodes along the abdominal aorta and vena cava is usually found in testicular cancer; however, in some cases, SNs are also found in the trajectory of the funicular vessels. SPECT/CT identified aortocaval or paracaval SNs in five patients with right-sided testicular cancer, and para-aortic SNs in five patients with left-sided tumours; in three patients, SNs along the funicular vessels were detected [38].
In renal cell carcinoma, lymphatic drainage was seen in 14/20 patients (70 %) and SPECT/CT detected 26 SNs. The SNs were most frequently located para-aortically, but also drainage to retrocaval, hilar, celiac trunk, and thoracic (internal mammary chain, mediastinal and pleural) SNs was seen [39]. Lymphatic drainage from renal cell carcinoma along the thoracic duct was further documented using SPECT/CT in four out of 22 patients (18 %) with SN already visualised on SPECT [40].
Gynaecological malignancies
SPECT/CT increased the SN detection rate to 95 % in a series of 41 patients with cervical cancer, and was found to be useful for depicting unilateral drainage in 19 patients [41]. In another study of 44 patients with high-risk endometrial cancer, SPECT/CT identified SNs in 34 of them (77 %), visualising a total of 110 SNs. The most frequent location was the external iliac chain (71 %), but drainage to para-aortic SNs was also common (44 %). SPECT/CT was able to localise the only pelvic metastatic lymph node that was not depicted on planar images [42]. In a series of seven patients with cervical and seven with vulvar cancer, SPECT/CT increased the SN visualisation rate to 100 %, from the 85 % obtained with planar imaging [27]. In another evaluation including 36 patients with cervical cancer, 21 with endometrial cancer, and seven with vulvar cancer, the SPECT/CT detection rate was 94 versus 89 % for planar scintigraphy [43]. SPECT/CT has also been helpful in more sophisticated SN procedures, such as robotic surgery. In particular, in a group of 29 cervical cancer patients, SPECT/CT led to more bilateral visualisation (86.2 %) than in a group of 33 patients investigated only with planar lymphoscintigraphy (75.8 %). Robot-assisted laparoscopic SN retrieval times were significantly reduced in the SPECT/CT group (50.1 ± 15.6 versus 75.4 ± 33.5 min) in comparison with the group evaluated only with planar scintigraphy [44]. More recently, in a study of 70 patients with endometrial cancer SPECT/CT detected SNs in 64 of them (91.4 %). However, SPECT/CT detected only 88.9 % of the SNs found during surgery; most of these nodes that were undetected on SPECT/CT had very low activity [45]. The SPECT/CT SN identification rate (94 %) was significantly higher than the identification rate obtained with planar lymphoscintigraphy (68 %) in a series of 31 patients with endometrial cancer investigated after transcervical injection of tracer into the isthmocervical myometrium [46].
Other malignant tumours
Preoperative SPECT/CT and lymphoscintigraphy for SN localisation have not been used extensively in gastrointestinal malignancies. In a first evaluation, SPECT/CT detected SNs in seven of eight patients with oesophageal cancer (88 %) after endoscopic submucosal radiotracer injection the day before surgery [47]. In stage Ia non-small cell lung cancer, SPECT/CT visualised SNs in 39/63 patients (62 %) and was useful in the anatomical depiction of SNs in the hilar and mediastinal lymph node basins [48].
Some requirements for SPECT/CT imaging
SPECT/CT is used primarily for the anatomical localisation of SNs and imaging protocols are, in principle, related to this objective. This also explains why SPECT/CT is usually acquired using a low-dose CT scanner. Acquisition of a diagnostic high-dose CT scan, with or without intravenous contrast, is not really necessary since the aim of the SN procedure is simply to identify subclinical metastases in lymph nodes that are not enlarged.
SPECT/CT is performed in addition to lymphoscintigraphy and both are preoperative parts of the SN procedure. For this, preoperative imaging colloid particles labelled with 99mTc are usually employed. After phagocytosis, these radiocolloids are incorporated into macrophages, thus resulting in prolonged lymph node retention and an adequate detection window. This not only enables the acquisition of delayed planar images and SPECT/CT, but also intraoperative gamma ray-guided SN localisation.
A specific requirement for SN localisation is that the CT component of SPECT/CT be of sufficient quality to provide optimal anatomical information. Early reports on SPECT/CT for SN localisation were based on the use of a low-end slow CT scanner [19]. The second generation of SPECT/CT gamma cameras includes an improved fast high-end CT component; this means that it is possible to identify and evaluate the lymph nodes corresponding to the radioactive nodes on fused SPECT/CT images by acquiring a low-dose CT scan. The acquisition protocol for CT at the Netherlands Cancer Institute is based on 130 kV, 40 mAs, and Kernel B30s medium. A low radiation dose, ranging from 1.3 to 5 mGy, is added to lymphatic mapping by the low-dose CT scan, together with a radiation exposure of about 1.5 mSv (depending on the scanning protocol) [8]. In superficial areas such as the groin and the axilla, 5-mm slices may provide adequate anatomical detail. For more complex anatomical areas (head/neck, pelvis, abdomen), 2-mm slices may be necessary. With this approach, SPECT/CT can accurately localise SNs in relation to the vascular structures in deep anatomical areas.
The CT component is also used to correct the SPECT signal for tissue attenuation and scattering. After these corrections, SPECT can be fused with CT [49]. For fused images, a grey scale is used to display the morphology in the background image (CT), whereas a colour scale is used to display the SN in the foreground image (SPECT).
For reading/reporting purposes, SPECT/CT images are mostly displayed in a manner similar to that of conventional tomography. The two-dimensional display of fused images to be correlated with CT and SPECT is facilitated by multiplanar reconstruction and the use of cross-reference lines allows navigation between axial, coronal and sagittal views. At the same time, this tool enables the correlation of radioactive SNs seen on fused SPECT/CT with lymph nodes seen on CT. Most frequently, a radioactive SN corresponds to a single lymph node on CT, but in some cases it correlates with a cluster of lymph nodes. This information may be useful for the intraoperative procedure and the post-excision control using portable gamma cameras or probes, as more radioactive SNs may be harvested at the same location.
The use of maximum intensity projection (MIP) to display fused SPECT/CT images may also help surgeons to anatomically recognise and localise SNs. MIP is a specific type of rendering in which the brightest voxels are projected into a three-dimensional image. A limitation of MIP is that the presence of other high-attenuation voxels on CT may make it difficult to recognise the vasculature and other anatomical structures. Further, MIP provides a two-dimensional representation, which cannot accurately depict the actual relationships of the vessels and other structures [50].
Finally, SN localisation in a three-dimensional context can be supported by the application of volume rendering. In this modality, different colours are assigned to anatomical structures such as vessels, muscle, bone and skin. This results in easily recognisable anatomical reference points facilitating the localisation of SNs, for instance, in relation to the vasculature. By incorporating a colour display, volume rendering improves visualisation of complex anatomy and 3D relationships.
Combined image reading of SPECT/CT and lymphoscintigraphy
SPECT/CT should be considered a complementary modality to planar lymphoscintigraphic imaging. The primary objective of SPECT/CT is to anatomically localise SNs already visualised on planar images. However, SPECT/CT frequently detects additional SNs, especially in areas with a high number of lymph nodes, such as the neck, or having a complex anatomy, such as the pelvis and abdomen. SPECT/CT is also useful to detect SNs in the vicinity of the injection site.
SPECT/CT findings and the findings of planar images must be interpreted together [51]. The acquisition of early and delayed planar lymphoscintigraphic images allows the identification of SNs in a majority of cases. In most current protocols, SPECT/CT is performed following delayed planar imaging (usually 2–4 h after tracer administration). This sequential acquisition helps to clarify the role of the two modalities.
There are certain factors to consider when seeking to identify radioactive lymph nodes as SNs: the visualisation of lymphatic ducts, the time of appearance, the lymph node basin, and the intensity of lymph node uptake [52]. On the basis of these factors, visualised radioactive lymph nodes may be considered definite SNs (when lymph nodes draining from the site of the primary tumour are visualised with their own afferent lymphatic vessel or when a single radioactive lymph node in a lymph node basin is seen) [53], highly probable SNs (when lymph nodes appear between the injection site and a first draining node or when nodes with increasing uptake appear in other lymph node stations), or less probable SNs (all higher echelon lymph nodes in trunk and extremities, or lower echelon lymph nodes in the head and neck).
Early planar images mostly lead to identification of the first draining lymph nodes as SNs by visualisation of their lymphatic ducts. These lymph nodes can be distinguished from secondary lymph nodes which mostly appear on delayed planar images.
In other cases, a single lymph node is seen on early and/or delayed images. This node is also considered a definite SN. However, in some cases, SPECT/CT detects additional lymph nodes in other basins such as the pelvis for instance (Fig. 1). These nodes can be considered definite or highly probable SNs. Less frequently, a radioactive lymph node may appear between the injection site and a first draining node (Fig. 2); its increased uptake can confirm this node as a highly probable SN and help to distinguish it from prolonged valve activity in a lymphatic duct, which usually shows decreased uptake intensity on delayed images.

In a patient with prostate cancer, a delayed anterior planar image (a) shows drainage to a left pelvic lymph node. By contrast, on volume rendering SPECT/CT (b), two additional radioactive nodes are seen between the injection site in the prostate and the first appearing pelvic node. These additional sentinel nodes are located in two different basins in the presacral area (c–e), whereas the first appearing sentinel node is seen more ventrally in the pelvis (f) (colour figure online)

An early planar anterior image (a) showing drainage from the injection site in the left breast to a lymph node in the upper area of the left axilla (arrow). On a delayed planar image (b), a lymph node (dotted arrow) can be observed between the injection site and the first draining node. It can be noted on SPECT/CT with volume rendering (c) and axial slices that the first draining lymph node is located in the interpectoral space (d) together with a second echelon lymph node showing less uptake, and corresponds to a single small lymph node (circle) on CT (e). The most caudal radioactive node is located in level 1 of the axilla (f) and corresponds to an elongated lymph node (circle) on CT (g). Both the interpectoral and the axillary lymph nodes are considered sentinel nodes (colour figure online)
Summarising indications for SPECT/CT in lymphatic mapping
As mentioned earlier in this paper, the indications for SPECT/CT in the SN procedure depend on the type of malignancy and the complexity of the lymphatic drainage. For some malignancies, such as breast cancer [54] and gynaecological malignancies [55], indications for SPECT/CT have been incorporated into the guidelines of international nuclear medicine associations. Indications for this technique also depend on the criteria adopted by surgeons and nuclear physicians in different hospitals. In general, the indications for incorporation of SPECT/CT imaging into the SN procedure are as follows:
-
(a)
SN detection when no lymphatic drainage is observed on planar lymphoscintigraphy. Due to the correction for tissue attenuation, SPECT/CT is usually more sensitive than planar imaging (Fig. 3) and may be particularly useful in obese patients, as has been demonstrated in breast cancer [56].
Fig. 3 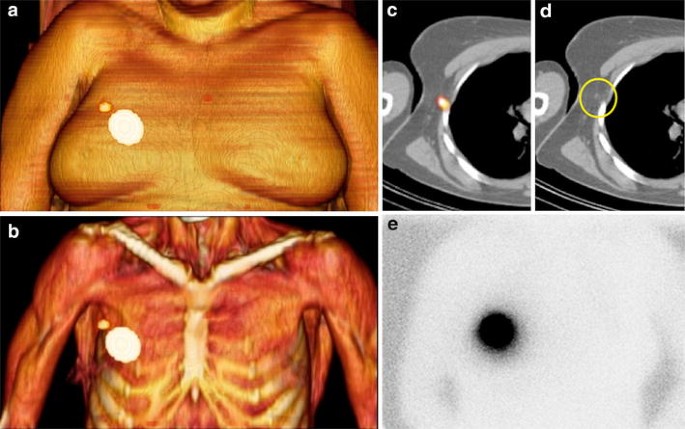
In an obese patient with breast cancer, SPECT/CT displayed with volume rendering (a, b) shows drainage from the injection site in the right breast to a lymph node in the ipsilateral axilla. On axial SPECT/CT (c), this sentinel node is seen in level 1 of the axilla and is not enlarged (circle) on CT (d). Note that on a delayed planar anterior image (e), no migration of the radiotracer is observed (colour figure online)
-
(b)
SN localisation in areas with a complex anatomy and a high number of lymph nodes such as the head and neck (Fig. 4), or in cases with unexpected lymphatic drainage (e.g. interpectoral, internal mammary chain, level II or III of the axilla, in the vicinity of the scapula) on planar lymphoscintigraphy. SPECT/CT is also helpful in cases with aberrant lymphatic drainage, as can be seen, for instance, in breast cancer recurrence or in patients who have undergone breast surgery in the past (Fig. 5).
Fig. 4 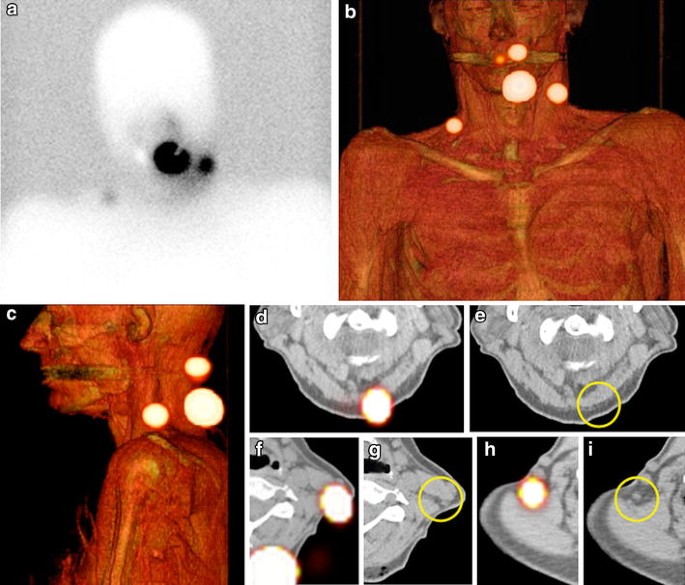
In a patient with a melanoma located dorsally at the neck, delayed planar anterior imaging (a) and volume rendering SPECT/CT (b, c) show drainage to both sides of the neck and to the suboccipital area. Note that on SPECT/CT and CT, these sentinel nodes are seen as single small lymph nodes (d–i) (colour figure online)
Fig. 5 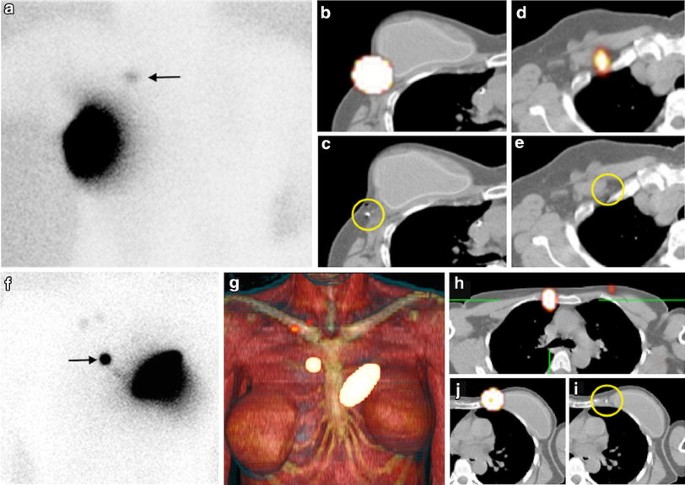
In a patient with a non-palpable cancer recurrence in the left breast, a planar anterior image (a) shows drainage to a solitary lymph node (arrow). On axial SPECT/CT (b), the injection site coincides with the site of an intratumoral marker (circle) lateral to the breast prosthesis on CT (c). The sentinel node (d) is located close to the inner border of the minor pectoral muscle in the infraclavicular area and corresponds to a small node (circle) on CT (e). In another patient with a cancer recurrence in the left breast, a planar image (f) shows contralateral drainage (arrow). SPECT/CT images (g, h) show a sentinel node near the right border of the manubrium. The tracer was administered medially to the breast prosthesis (j) at the site of a marker indicating the tumour recurrence (circle) as seen on CT (i) (colour figure online)
-
(c)
Anatomical localisation and detection of additional SNs in areas of deep lymphatic drainage such as the pelvis, abdomen or mediastinum [57].
-
(d)
Detection of SNs in the vicinity of the injection as observed, for instance, in:
-
periauricular melanomas with drainage to SNs in the parotid region and/or level II of the neck
-
oral cavity cancer and melanomas of the lower part of the face draining to submental and submaxillary SNs (Fig. 6)
Fig. 6 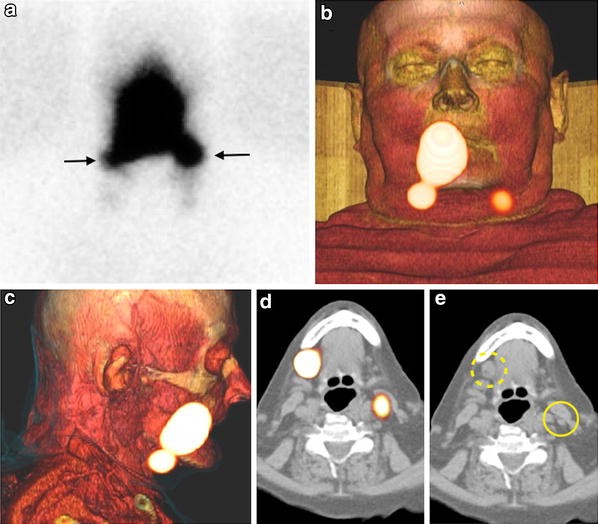
In a patient with an oral cavity cancer, a delayed anterior planar image (a) shows drainage to both sides of the neck (arrows). On volume rendering SPECT/CT (b, c), both sentinel nodes are visualised as clearly distinct from the injection site in the right border of the tongue. Note that the sentinel node on the left (d) corresponds to a small lymph node (circle) on CT (e), whereas the right submandibular sentinel node (dotted circle) is enlarged; on histopathology, it was found to contain metastasis (colour figure online)
-
melanomas of the upper part of the trunk draining to periscapular and supraclavicular nodes
-
melanomas of the back draining to intercostal and retroperitoneal nodes
-
breast cancer draining to intramammary SNs or axillary nodes close to the primary tumour in the upper outer quadrant of the breast
-
prostate cancer or cervical cancer draining to pelvic SNs.
-




SPECT/CT as the basis for new technological approaches
SPECT/CT appears to provide a basis for novel approaches in the SN procedure. The first one is related to the introduction of hybrid tracers for SN detection Due to their radioactive component, these novel tracers are able to facilitate preoperative mapping with lymphoscintigraphy and SPECT/CT without modification of the imaging protocols used for standard radioactive colloids. On the other hand, the fluorescence component of the tracer facilitates high-resolution optical SN imaging during surgery [58]. In 25 patients with melanoma or penile cancer, SPECT/CT helped to establish, with respect to lymphatic drainage, 100 % reproducibility between the hybrid tracer ICG-99mTc-nanocolloid and the parental tracer 99mTc-nanocolloid; SPECT/CT in combination with lymphoscintigraphy detected SNs in all patients [59]. Using the same hybrid tracer, SPECT/CT detected additional SNs in 3 out of 14 oral cavity cancer patients (7 tongue, 5 floor of mouth, 1 lower lip, and 1 buccal mucosa); SN visualisation was achieved in all the patients [60]. In another study of 11 head and neck melanoma patients, SPECT/CT performed 2 h after injection of ICG-99mTc-nanocolloid in combination with lymphoscintigraphy visualised SNs in all patients [61]. The combination of preoperative SPECT/CT with intraoperative imaging using a portable gamma camera together with a near-infrared fluorescence camera led to the detection of 26 % additional SNs in 25 patients with head and neck malignancies who received the hybrid tracer ICG-99mTc-nanocolloid [62]. The same multimodal approach based on SPECT/CT and hybrid intraoperative imaging detection was able to identify SNs in all 14 patients in a study aimed at evaluating SN identification in vulvar cancer using ICG-99mTc-nanocolloid [63], as well as in all the 65 penile cancer patients included in another study [64]; in both series, the multimodal approach significantly improved optical SN detection compared with blue dye. Also, in prostate cancer, SPECT/CT after administration of ICG-99mTc-nanocolloid helped to localise SNs in 11 patients scheduled for a robot-assisted laparoscopic procedure [65].
SPECT/CT incorporated into the evaluation of the novel radiotracer 99mTc-tilmanocept led to the identification of additional SNs in 11 of 20 patients (55 %) with oral cavity squamous cell carcinoma [66].
Another novel approach is constituted by the transfer of preoperative SPECT/CT imaging to the operating room through mixed reality protocols. In 1994, Milgram and Kishino introduced the mixed reality concept which refers to the merging of real and virtual elements to produce new environments [67]. One aspect of the mixed reality concept concerns the possibility of generating a continuum of virtual elements from a real object. Applying this concept to the current situation in nuclear medicine and radioguided surgery, SPECT/CT emerges as an important source of virtual elements generated from patients scheduled for SN biopsy. Currently, SPECT/CT is exclusively used for preoperative SN localisation in radioguided surgery. Through the use of a tracking protocol based on reference targets, it has now become possible to transfer virtual SPECT/CT images to the operating room, thus creating a merged environment adequate for surgical navigation (Fig. 7). This approach was used to navigate towards the prostate and SNs in a patient undergoing robot-assisted prostatectomy [68], as well as in a patient with a primary parotid malignancy scheduled for the SN procedure [69]. Also crucial for SPECT/CT image-guided surgical navigation, in addition to the creation of a mixed reality environment, is real-time visualisation or guidance. Fixed screen visualisation is currently applied for open surgery and will probably become a frequently used modality in laparoscopic procedures, as recently reviewed in relation to genitourinary cancers [70]. However, the development of special glasses, head-mounted display devices or portable screens enabling surgeons to display virtual elements directly in their field of view during the operation appears to be mandatory for open surgery. This direct projection of 3D SPECT/CT imaging into the surgical field is in the development phase and in this context the introduction of head-mounted display devices may represent an important advance [71].

In a patient with oral cavity cancer drainage to the left side of the neck is seen on volume rendering SPECT/CT (a). Note the reference target (ReT) placed on the left side of the head. Based on this ReT, the SPECT/CT image is displayed in the operating room (b) creating a mixed reality environment allowing surgical navigation towards the sentinel nodes (c) using a tracked gamma probe (Surgic Eye, Munich) (colour figure online)
Final remarks
SPECT/CT has been incorporated into the SN procedure as an important preoperative imaging component and a complement to planar lymphoscintigraphy. Although in breast cancer SPECT/CT is limited to specific indications, in melanoma the use of SPECT/CT is growing due to its role in modification of the surgical approach, its greater detection rate of additional SNs, its cost effectiveness, and its possible association with higher rates of disease-free interval. In malignancies with lymphatic drainage to complex body areas, SPECT/CT appears to be mandatory due to its essential contribution to the anatomical localisation of SNs. SPECT/CT is also adequate as a preoperative imaging tool when hybrid tracers, which combine radioactivity and fluorescence in one signature, are used. Finally, SPECT/CT will probably play an important role in the development of mixed reality protocols for surgical navigation in the future.
References
Morton DL, Wen DR, Wong JH, Economou JS, Cagle LA, Storm FK et al (1992) Technical details of intraoperative lymphatic mapping for early stage melanoma. Arch Surg 127:392–399
Krag DN, Weaver DL, Alex JC, Fairbank JT (1993) Surgical resection and radiolocalization of the sentinel lymph node in breast cancer using a gamma probe. Surg Oncol 2:335–339
Valdés Olmos RA, Hoefnagel CA, Nieweg OE, Jansen L, Rutgers EJ, Border J et al (1999) Lymphoscintigraphy in oncology: a rediscovered challenge. Eur J Nucl Med 26:S2–S10
Van der Ploeg IM, Valdés Olmos RA, Kroon BB, Wouters MW, van den Brekel MW, Vogel WV et al. (2009) The yield of SPECT/CT for anatomical lymphatic mapping in patients with melanoma. Ann Surg Oncol l16: 1537–1542
Mucientes Rasilla J, Cardona Arbonies J, Delgado Bolton R, Izarduy Pereyra L, Salazar Andia G, Prieto Soriano A et al (2009) SPECT-CT in sentinel node detection in patients with melanoma. Rev Esp Med Nucl 28:229–234
Veenstra HJ, Vermeeren L, Valdés Olmos RA, Nieweg OE (2012) The additional value of lymphatic mapping with routine SPECT/CT in unselected patients with clinically localized melanoma. Ann Surg Oncol 19:1018–1023
Fairbairn N, Munson C, Ali Khan Z, Butterworth M (2013) The role of hybrid SPECT/CT for lymphatic mapping in patients with melanoma. J Plastic Rec Aesthet Surg 66:1248–1255
Kraft O, Havel M (2012) Localisation of sentinel lymph nodes in patients with melanomas by planar lymphoscintigraphic and hybrid SPECT/CT imaging. Nucl Med Rev Cent East Eur 15:101–107
Martínez Castillo R, Fernández López R, Acevedo Bañez I, Alvarez Pérez RM, García Solis D, Vázquez Albertino R, Fernández Ortega P (2014) Utility of single photon emission computed tomography-computed tomography in selective sentinel lymph node biopsy in patients with melanoma. Rev Esp Med Nucl Imagen Mol 33:129–135
Stoffels I, Boy C, Pöppel T, Kuhn J, Klötgen K, Dissemond J et al (2012) Association between lymph node excision with or without preoperative SPECT/CT and metastatic node detection and disease-free survival in melanoma. JAMA 308:1007–1014
Stoffels I, Müller M, Geisel MH, Leyh J, Pöppel T, Schadendorf D, Klode J (2014) Cost-effectiveness of preoperative SPECT/CT combined with lymphoscintigraphy vs. lymphoscintigraphy for sentinel lymph node excision in patients with cutaneous malignant melanoma. Eur J Nucl Med Mol Imaging 41:1723–1731
Van der Ploeg IM, Nieweg OE, Kroon BB, Rutgers EJ, Baas-Vrancken Peeters MJ, Vogel WV et al (2009) The yield of SPECT/CT for anatomical lymphatic mapping in patients with breast cancer. Eur J Nucl Med Mol Imaging 36:903–909
Husarik DB, Steinert HC (2007) Single-photon emission computed tomography/computed tomography for sentinel node mapping in breast cancer. Semin Nucl Med 37:29–33
Leman H, Lievshitz G, Zak O, Metser U, Schneebaum S, Even-Sapir E (2007) Improved sentinel node identification by SPECT/CT in overweight patients with breast cancer. J Nucl Med 48:201–206
Leman H, Metser U, Lievshitz G, Sperber F, Shneebaum S, Even-Sapir E (2006) Lymphoscintigraphic sentinel node identification in patients with breast cancer: the role of SPECT/CT. Eur J Nucl Med Mol Imaging 33:329–337
Gallowitsch HJ, Kraschi P, Igerc I, Hussein T, Kresnik E, Mikosch P et al (2007) Sentinel node SPECT-CT in breast cancer. Can we expect any additional and clinically relevant information? Nuklearmedizin 46:252–256
Uren RF, Howman-Giles R, Chung DKV, Spillane AJ, Noushi F, Gillet D et al (2012) SPECT/CT scans allow precise anatomical location of sentinel lymph nodes in breast cancer and redefine lymphatic drainage from the breast to the axilla. Breast 21:486–489
Vercellino L, Ohnona J, Groheux D, Slama A, Colletti PM, Chondrogiannis S et al (2014) Role of SPECT/CT in sentinel lymph node detection in patients with breast cancer. Clin Nucl Med 39:431–436
Alkureishi LWT, Burak Z, Alvarez JA, Ballinger J, Bilde A, Britten AJ et al (2009) Joint practice guidelines for radionuclide lymphoscintigraphy for sentinel node localization in oral/oropharyngeal squamous cell carcinoma. Eur J Nucl Med Mol Imaging 36:1915–1936
Haerle SK, Hany TF, Strobel K, Sidler D, Stoeckli SJ (2009) Is there an additional value of SPECT/CT over planar lymphoscintigraphy for sentinel node mapping in oral/oropharyngeal squamous cell carcinoma? Ann Surg Oncol 16:3118–3124
Bilde A, Von Buchwald C, Mortensen J, Marving J, Hamilton Therkildsen M, Kirkegaard J et al (2006) The role of SPECT-CT in the lymphoscintigraphic identification of sentinel nodes in patients with oral cancer. Acta Otolaryngol 126:1096–1103
Vermeeren L, Valdés Olmos RA, Klop MC, van der Ploeg IMC, Nieweg OE, Balm AJM et al (2011) SPECT/CT for sentinel lymph node mapping in head and neck melanoma. Head Neck 33:1–6
Klode J, Poeppel T, Boy C, Mueller S, Schadendorf D, Korber A et al (2011) Advantages of preoperative hybrid SPECT/CT in detection of sentinel lymph nodes in cutaneous head and neck malignancies. J Eur Acad Dermatol Venereol 25:1213–1221
Zender C, Guo T, Weng C, Faulhaber P, Rezaee R (2014) Utility of SPECT/CT for periparotid sentinel lymph node mapping in the surgical management of head and neck melanoma. Am J Otolaryngol 35:12–18
Daisne JF, Installé J, Bihin B, Laloux M, Vander Borght T, Mathieu I, Lawson G (2014) SPECT/CT lymphoscintigraphy of sentinel node(s) for superselective prophylactic irradiation of the neck in cN0 head and neck cancer patients: a prospective phase I feasibility study. Rad Oncol 9:121
Garcia-Burillo A, Roca Bielsa I, Gonzalez O, Zafon C, Sabate M, Castellvi J et al (2013) SPECT/CT sentinel lymph node identification in papillary thyroid cancer: lymphatic staging and surgical management improvement. Eur J Nucl Med Mol Imaging 40:1645–1655
Cabrera RN, Chone CT, Zantut-Wittmann D, Matos P, Ferreira DM, Pereira PSG et al (2014) Value of sentinel lymph node biopsy in papillary thyroid cancer: initial results of a prospective trial. Eur Arch Otorhinolaryngol. doi:10.1007/s00405-014-3018-2
Belholcine TZ, Prefontaine M, Lanvin D, Bertrand M, Rachinsky I, Etter H et al (2013) Added-value of SPECT/CT to lymphatic mapping and sentinel lymphadenectomy in gynaecological cancers. Am J Nucl Med Mol Imaging 3:182–193
Beneder C, Fuechsel FG, Krause T, Kuhn A, Mueller MD (2008) The role of 3D fusion imaging in sentinel lymphadenectomy for vulvar cancer. Gynecol Oncol 109:76–80
Leijte JA, Valdés Olmos RA, Nieweg OE, Horenblas S (2008) Anatomical mapping of lymphatic drainage in penile cancer with SPECT/CT: implications for the extent of inguinal lymph node dissection. Eur Urol 54:885–890
Leijte JA, van der Ploeg IM, Valdés Olmos RA, Nieweg OE, Horenblas S (2009) Visualization of tumor blockage and rerouting of lymphatic drainage in penile cancer by use of SPECT/CT. J Nucl Med 50:364–367
Vermeeren L, Valdés Olmos RA, Meinhardt W, Bex A, van der Poel HG, Vogel WW et al (2009) Value of SPECT/CT for detection and anatomic localization of sentinel lymph nodes before laparoscopic sentinel node lymphadenectomy in prostate cancer. J Nucl Med 50:865–870
Meinhardt W, van der Poel HG, Valdés Olmos RA, Bex A, Brouwer OR, Horenblas S (2012) Laparoscopic sentinel lymph node biopsy for prostate cancer: the relevance of locations outside the extended dissection area. Prostate Cancer 2012:751753
Vermeeren L, Meinhardt W, van der Poel HG, Valdés Olmos RA (2010) Lymphatic drainage from the treated versus untreated prostate: feasibility of sentinel node biopsy in recurrent cancer. Eur J Nucl Med Mol Imaging 37:2012–2026
Krengli M, Ballare A, Cannillo B, Rudoni M, Kocjancic E, Loi G et al (2006) Potential advantage of studying the lymphatic drainage by sentinel node technique and SPECT-CT image fusion for pelvic irradiation of prostate cancer. Int J Radiat Oncol Biol Phys 66:1100–1104
Rousseau C, Rousseau T, Campion L, Lacoste J, Aillet G, Potiron E et al (2014) Laparoscopic sentinel lymph node versus hyperextensive pelvic dissection for staging clinically localized prostate carcinoma; a prospective study of 200 patients. J Nucl Med 55:753–758
de Bonilla-Damiá A, Brouwer OR, Meinhardt W, Valdés Olmos RA (2012) Lymphatic drainage in prostate carcinoma assessed by lymphoscintigraphy and SPECT/CT: its importance for the sentinel node procedure. Rev Esp Med Nucl Imagen Mol 31:66–70
Brouwer OR, Valdés Olmos RA, Vermeeren L, Hoefnagel CA, Nieweg OE, Horenblas S (2011) SPECT/CT and a portable γ-camera for image-guided laparoscopic sentinel node biopsy in testicular cancer. J Nucl Med 52:551–554
Bex A, Vermeeren L, Meinhardt W, Prevoo W, Horenblas S, Valdés Olmos RA (2011) Intraoperative sentinel node identification and sampling in clinically node-negative renal cell carcinoma: initial experience in 20 patients. World J Urol 29:793–799
Brouwer OR, Noe A, Valdes Olmos RA, Bex A (2013) Lymphatic drainage from renal cell carcinoma along the thoracic duct visualized with SPECT/CT. Lymphat Res Biol 11:233–238
Martinez A, Zerdoud S, Mery E, Bouissou E, Ferron G, Querleu D (2010) Hybrid imaging by SPECT/CT for sentinel lymph node detection in patients with cancer of the uterine cervix. Gynecol Oncol 119:431–435
Perissinotti A, Paredes P, Vidal-Sicart S, Torné A, Albela S, Navales I et al (2013) Use of SPECT/CT for improved sentinel lymph node localization in endometrial cancer. Gynecol Oncol 129:42–48
Kraft O, Havel M (2012) Detection of sentinel lymph nodes in gynecologic tumors by planar scintigraphy and SPECT/CT. Mol Imaging Radionucl Ther 21:47–55
Hoogendam JP, Hobbelink MGG, Veldhuis WB, Verheijen RHM, van Diest PJ, Zweemer RP (2013) Preoperative sentinel node mapping with 99mTc-nanocolloid SPECT-CT significantly reduces the intraoperative sentinel node retrieval time in robot assisted laparoscopic cervical cancer surgery. Gynecol Oncol 129:389–394
Sawicki S, Kobierski J, Lapinska-Szumczyk S, Lass P, Cytawa W, Bianek-Bodzak A, Wydra D (2013) Comparison of SPECT/CT results and intraoperative detection of sentinel lymph nodes in endometrial cancer. Nucl Med Commun 34:590–596
Mücke J, Klapdor R, Scheider M, Länger F, Gratz KF, Hillemans P, Hertel H (2014) Isthmocervical labeling and SPECT/CT for optimized sentinel node detection in endometrial cancer: technique, experience and results. Gynecol Oncol 134:287–292. doi:10.1016/j.ygyno.2014.05.001
Tsai JA, Celebioglu F, Lindblad M, Lörinc E, Nilsson M, Olsson A, Lundell L, Axelsson R (2013) Hybrid SPECT/CT imaging of sentinel nodes in esophageal cancer: first results. Acta Radiol 54:369–373
Nomori H, Ikeda K, Mori T, Shiraishi S, Kobayashi H, Kawanaka K et al (2007) Sentinel node identification in clinical stage Ia non-small cell lung cancer by a combined single photon emission computed tomography/computed tomography system. J Thorac Cardiovasc Surg 134:182–187
Delbeke D, Coleman RE, Guiberteau MJ, Brown ML, Royal HD, Siegel BA et al (2006) Procedure guidelines for SPECT/CT imaging. J Nucl Med 47:1227–1234
Fishman EK, Ney DR, Heath DG, Corl FM, Horton KM, Johnson PT (2006) Volume rendering versus maximum intensity projection in CT angiography: what works best, when, and why. Radiographics 26:905–922
Vidal-Sicart S, Brouwer OR, Valdés Olmos RA (2011) Evaluation of the sentinel lymph node combining SPECT/CT with the planar images and its importance for the surgical act. Rev Esp Med Nuc 30:331–337
Nieweg OE, Estourgie S, Valdés Olmos RA (2004) Lymphatic mapping and sentinel node biopsy. In: Ell PJ, Gambhir SS (eds) Nuclear medicine in clinical diagnosis and treatment, 3rd edn. Churchill Livingstone, Edinburgh, pp 229–260
Alazraki N, Glass EC, Castronovo F, Valdés Olmos RA, Podoloff D (2002) Procedure guideline for lymphoscintigraphy and the use of intraoperative gamma probe for sentinel lymph node localization in melanoma of intermediate thickness 1.0. J Nucl Med 43:1414–1418
Giammarile F, Alazraki N, Aarsvold JN, Audisio RA, Glass E, Grant SF et al (2013) The EANM and SNMMI practice guideline for lymphoscintigraphy and sentinel node localization in breast cancer. Eur J Nucl Med Mol Imaging 40:1932–1947
Giammarile F, Fani Bozkurt M, Cibula D, Pahisa J, Oyen WL, Paredes P, Valdés Olmos R, Vidal Sicart S (2014) The EANM clinical and technical guidelines for lymphoscintigraphy and sentinel node localization in gynaecological cancers. Eur J Nucl Med Mol Imaging 41:1463–1477
Van der Ploeg IM, Valdés Olmos RA, Kroon BB, Wouters MW, van den Brekel MW, Vogel WV et al (2009) The yield of SPECT/CT for anatomical lymphatic mapping in patients with melanoma. Ann Surg Oncol 16:1537–1542
Vermeeren L, van der Ploeg IM, Valdés Olmos RA, Meinhardt W, Klop WM, Kroon BB et al (2010) SPECT/CT for preoperative sentinel node localization. J Surg Oncol 101:184–190
Rietbergen D, Van den Berg NS, Van Leeuwen FWB, Valdés Olmos RA (2013) Hybrid techniques for intraoperative sentinel lymph node imaging: early experiences and future prospects. Imaging Med 5:147–159
Brouwer OR, Vermeeren L, Klop WMC, Balm AJM, van der Poel HG, van Rhijn BW et al (2012) Comparing the hybrid fluorescent-radioactive tracer indocyanine green-99mTc-nanocolloid with 99mTc-nanocolloid for sentinel node identification: a validation study using lymphoscintigraphy and SPECT/CT. J Nucl Med 53:1034–1040
Van den Berg NS, Brouwer OR, Klop WMC, Karakullucku B, Zuur CL, Tan IB et al (2012) Concomitant radio-and fluorescence-guided sentinel node biopsy in squamous cell carcinoma of the oral cavity using ICG-99mTc-nanocolloid. Eur J Nucl Med Mol Imaging 39:1128–1136
Brouwer OR, Klop MC, Buckle T, Vermeeren L, van der Brekel MWM, Balm AJM et al (2012) Feasibility of sentinel node biopsy in head and neck melanoma using a hybrid radioactive and fluorescent tracer. Ann Surg Oncol 19:1988–1994
Borbón-Arce M, Brouwer OP, van den Berg NS, Mathéron H, Klop WM, Balm AJ, van Leeuwen FW, Valdés Olmos RA (2014) An innovative multimodality approach for sentinel node mapping and biopsy in head and neck malignancies. Rev Esp Med Nucl Imagen Mol 33:274–279. doi:10.1016/j.remn.2013.11.005
Mathéron HM, van den Berg NS, Brouwer OP, Kleijan GH, van Driel WJ, Trum JW, Vegt E, Kenter G, van Leeuwen FW, Valdés Olmos RA (2013) Multimodal surgical guidance towards the sentinel node in vulvar cancer. Gynecol Oncol 131:720–725
Brouwer OR, van den Berg NS, Mathéron HM, van der Poel HG, van Rhijn BW, Bex A, van Tinteren H et al (2014) A hybrid radioactive and fluorescent tracer for sentinel node biopsy in penile carcinoma as a potential replacement for blue dye. Eur Urol 65:600–609
van der Poel HG, Buckle T, Brouwer OR, Valdés Olmos RA, van Leeuwen FWB (2011) Intraoperative laparoscopic fluorescence guidance to the sentinel node in prostate cancer patients: clinical proof of concept of an integrated functional imaging approach using a multimodal tracer. Eur Urol 60:826–833
Marcinow AM, Hall N, Byrum E, Teknos N, Old MO, Agrawal A (2013) Use of a novel receptor-targeted (CD206) radiotracer 99mTc-tilmanocept, and SPECT/CT for sentinel lymph node detection in oral squamous cell carcinoma: initial institutional report in an ongoing phase 3 study. JAMA Otolaryngol Head Neck Surg 139:895–902
Milgram P, Kishino FA (1994) A taxonomy of mixed reality visual displays. IEICE Trans Inform Syst E77-D:1321–1329
Brouwer OR, Buckle T, Bunschoten A, Vahrmeijer A, Wendler T, Valdés Olmos RA et al (2012) Image navigation as a means to expand the boundaries of fluorescence guided surgery. Phys Med Biol 57:3123–3136
Schilling C, Gnanasegaran G, McGurk M (2014) Three-dimensional imaging and navigated sentinel node biopsy for primary parotid malignancy: new application in parotid cancer management. Head Neck 36:E91–E93. doi:10.1002/hed.23560
Greco F, Cdeddu JA, Gill IS, Kaouk JH, Remzi M, Houston Thompson R, van Leeuwen FW, van der Poel HG, Formara P, Rassweller L (2013) Current perspectives in the use of molecular imaging to target surgical treatments for genitourinary cancers. Eur Urol 65:947–964
Sadda P, Azimi E, Jallo G, Doswell J, Kazanzides P (2013) Surgical navigation with a head-mounted tracking system and display. Stud Health Technol Inform 184:363–369
Conflict of interest
The authors confirm that they have not conflict of interest.
Human and animal studies
This paper is a review of available scientific literature on this topic including papers published in other journals that deal with human patients (in prospective and retrospective form). This article does not contain any direct studies with human or animal subjects performed by any of the authors.
Author information
Authors and Affiliations
Corresponding author
Additional information
Color figures online at http://link.springer.com/article/10.1007/s40336-014-0087-6.
Rights and permissions
About this article

Cite this article
Valdés Olmos, R.A., Rietbergen, D.D.D. & Vidal-Sicart, S. SPECT/CT and sentinel node lymphoscintigraphy. Clin Transl Imaging 2, 491–504 (2014). https://doi.org/10.1007/s40336-014-0087-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s40336-014-0087-6