
Abstract
Objective
We sought to compare strengths of association among multiple emergency department (ED) input, throughput and output metrics and the outcome of 72-h ED re-visits.
Methods
This database analysis used healthcare administrative data from three urban, university-affiliated EDs in Calgary, Canada, calendar years 2010–2014. We used data from all patients presenting to participating EDs during the study period, and the primary analysis was performed on patients discharged from the ED. Regression models quantified the association between input, throughput and output metrics and the risk of return ED visit within 72 h of discharge from the index ED encounter. Strength of association between the crowding metrics and 72-h ED re-visits was compared using Akaike’s Information Criterion.
Results
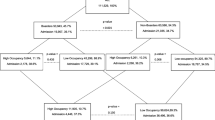
The findings of this study are based on data from 845,588 patient encounters ending in discharge. The input metric with the strongest association with 72-h re-visits was median ED waiting time. The throughput metric with the strongest association with 72-h re-visits was the ED occupancy. The output metric with the strongest association with 72-h re-visits was the median inpatient boarding time.
Conclusion
Input, throughput and output metrics are all associated with 72-h re-visits. Delays in any of these operational phases have detrimental effects on patient outcomes. ED waiting time, ED occupancy, and boarding times are the most meaningful input, throughput and output metrics. These should be the preferred metrics for quantifying ED crowding in research and quality improvement efforts, and for clinicians to monitor ED crowding in real time.
Résumé
Objectif
Nous avons cherché à comparer la force de l'association entre plusieurs paramètres d'entrée, de débit et de sortie des services d'urgence (SU) et l'issue des nouvelles visites aux SU après 72 heures.
Méthodes
Cette analyse de base de données a utilisé des données administratives sur les soins de santé de trois services d'urgence urbains affiliés à une université à Calgary, au Canada, pour les années civiles 2010-2014. Nous avons utilisé les données de tous les patients se présentant aux urgences participantes pendant la période de l'étude, et l'analyse primaire a porté sur les patients sortis des urgences. Des modèles de régression ont quantifié l'association entre les paramètres d'entrée, de débit et de sortie et le risque d'une nouvelle visite aux urgences dans les 72 heures suivant la sortie des urgences de référence. La force de l'association entre les paramètres d'encombrement et les réadmissions aux urgences à 72 heures a été comparée à l'aide du critère d'information d'Akaike.
Résultats
Les résultats de cette étude sont basés sur les données de 845 588 rencontres de patients se terminant par une sortie. La mesure d'entrée présentant la plus forte association avec les nouvelles visites dans les 72 heures était le temps d'attente médian aux urgences. La mesure du débit avec la plus forte association avec les visites répétées de 72 heures était l’occupation par le SU. La métrique de sortie présentant la plus forte association avec les revisites à 72 heures était la durée médiane d'embarquement des patients hospitalisés.
Conclusions
Les mesures d'entrée, de débit et de sortie sont toutes associées aux revisites de 72 heures. Les retards dans l'une de ces phases opérationnelles ont des effets néfastes sur les résultats pour les patients. Le temps d'attente aux urgences, le taux d'occupation des urgences et le temps d'embarquement sont les paramètres les plus significatifs en termes d'entrée, de débit et de sortie. Ces paramètres devraient être privilégiés pour quantifier l'encombrement des urgences dans le cadre de la recherche et des efforts d'amélioration de la qualité, et pour permettre aux cliniciens de surveiller l'encombrement des urgences en temps réel.

Similar content being viewed by others
Data access and sharing
De-identified data were provided to the investigators by Alberta Health Services and the University of Calgary Clinical Research Unit. Under the terms of our data sharing agreement and research ethics board approval, sharing of primary data is not possible.
References
Affleck A, Parks P, Drummond A, Rowe BH, Ovens HJ. CAEP position statement. Emergency department overcrowding and access block. CJEM. 2013;15:359–70.
Institute of Medicine Committee on the Future of Emergency Care in the United States Health System. Hospital-Based Emergency Care: At the breaking point. Washington, D.C.: The National Academies Press. 2006.
Bernstein SL, Aronsky D, Duseja R, et al. The effect of emergency department crowding on clinically oriented outcomes. Acad Emerg Med. 2009;16(1):1–10.
Pines J, Hollander J, Localio AR, Metlay J. The association between Emergency Department crowding and hospital performance on antibiotic timing for pneumonia and percutaneous intervention for myocardial infarction. Acad Emerg Med. 2006;13(8):873–8.
Chalfin DB, Trzeciak S, Likourezos A, Baumann BM, Dellinger RP. Impact of delayed transfer of critically ill patients from the emergency department to the intensive care unit. Crit Care Med. 2007;35(6):1477–83.
Guttman A, Schull M, Vermeulen MJ, Stukel TA. Association between waiting times and short term mortality and hospital admission after departure from emergency department: population based cohort study from Ontario, Canada. BMJ. 2011;342:d2983.
Sprivulis PC, Da Silva JA, Jacobs IG, Frazer AR, Jelinek GA. The association between hospital overcrowding and mortality among patients admitted via Western Australian emergency departments. Med J Aust. 2006;184(5):208–12.
Asplin BR, Magid DJ, Rhodes KV, Solberg LI, Lurie N, Camargo CA. A conceptual model of emergency department crowding. Ann Emerg Med. 2003;42(2):173–80.
Yoon P, Steiner I, Reinhardt G. Analysis of factors influencing length of stay in the emergency department. CJEM. 2003;5(3):155–61.
Ospina MB, Bond K, Schull M, Innes G, Blitz S, Friesen C, Rowe BH. Measuring overcrowding in emergency departments: a call for standardization [Technology report no 67.1]. Ottawa: Canadian Agency for Drugs and Technologies in Health; 2006.
Statistics Canada. Population and dwelling counts, for census metropolitan areas, 2016 and 2011 censuses – 100% data". https://www12.statcan.gc.ca/census-recensement/2016/dp-pd/hlt-fst/pd-pl/Table.cfm?Lang=Eng&T=205&S=3&RPP=100. Accessed 2 Sept 2021.
Scarlett J. ED timestamp validation (June 2008 for RGH and FMC). 2008. Alberta Health Services. Unpublished/internal document.
Scarlett J. PLC ED Timestamp validation. 2007. Alberta Health Services. Unpublished/internal document.
Schull MJ, Guttmann A, Hatcher CM, Leaver CA, Vermeulen M, Rowe BH, Zwarenstein M, Anderson GM. Consensus on evidence-based quality of care indicators for canadian emergency departments. CJEM. 2011;13(5):300–9 (E28–43).
National Health Service. Methodology for producing the A&E clinical quality indicator from provisional Hospital Episode Statistics data. https://files.digital.nhs.uk/D6/CA6CEA/Provisional%20Accident%20Emergency%20Quality%20Indicators%20for%20England%20-%20Indicator%20Generation%20Methodology%20-%20NHS%20Digital.pdf. Accessed 2 Sept 2021.
Siegel DM, Crocker PJ. Continuous quality improvement for emergency departments. Dallas: ACEP Publishing; 1994.
Solberg LI, Asplin BR, Weinick RM, Magid DJ. Emergency department crowding: consensus development of potential measures. Ann Emerg Med. 2003;42:824–34.
Welch SJ, Asplin BR, Stone-Griffith S, et al. Emergency department operational metrics, measures and definitions: results of the Second Performance Measures Benchmarking Summit. Ann Emerg Med. 2011;58:33–40.
Beveridge R, Clark B, Janes L, et al. Canadian emergency department triage and acuity scale: implementation guidelines. CJEM. 1999;1(suppl):S2–28.
Burnham KP, Anderson DR. Model selection and multimodel inference: a practical information-theoretic approach. 2nd ed. New York: Springer-Verlag; 2002.
Akaike H. Information theory as an extension of the maximum likelihood principle. In: Petrov BN, Csaki F, editors. Second international symposium on information theory. Budapest: Akademiai Kiado; 1973. p. 267–81.
Steyerberg EW, Harrell FE Jr, Borsboom GJ, et al. Internal validation of predictive models: efficiency of some procedures for logistic regression analysis. J Clin Epidemiol. 2001;54(8):774–81. https://doi.org/10.1016/s0895-4356(01)00341-9.
Canadian Institute for Health information. Emergency Department Data Tables, 2016–2017. https://www.cihi.ca/sites/default/files/document/nacrs-2016-2017-qs-static-table-en.xlsx. Accessed 2 Sept 2021.
Centers for Disease Control and Prevention national Center for Health Statistics. National Hospital Ambulatory Medical Care Survey: 2016 Emergency Department summary tables. https://www.cdc.gov/nchs/data/nhamcs/web_tables/2016_ed_web_tables.pdf. Accessed 2 Sept 2021.
Canadian Institute for Health Information. Yourhealthsystem Dashboard. https://yourhealthsystem.cihi.ca/hsp/indepth;jsessionid=c8XYozY-9HBHcGhnWqMkVjue.yhs?lang=en#/theme/f3647a180b929173539c81ef6e4de088e99bdff8/3/N4IgKgFgpgtlDCAXATgGxALlAYwPatQEMAHAZygBNNQAGGgRkxQFcoBfNgGhAC1cA7KABEoiQgEtUpJGmogoAD2KF-FSk2SsOQA. Accessed 2 Sept 2021.
Acknowledgements
This study was funded by an Open Operating Grant from the Canadian Institutes of Health Research (CIHR; Ottawa, Canada, MOP-133494). The funding sources had no direct involvement in the study design, analysis, interpretation or decision to submit this work.
Funding
This study was funded by an Open Operating Grant from the Canadian Institutes of Health Research (CIHR; Ottawa, Canada, MOP-133494). At the time of this project, BHR was supported by Tier I Canada Research Chair in Evidence-based Emergency Medicine from the CIHR. Dr. Rowe’s research is currently supported by a Scientific Director’s Grant (SOP 168483) from the Institute of Circulatory and Respiratory Health at CIHR through the Government of Canada (Ottawa, ON).
Author information
Authors and Affiliations
Contributions
ADM, RJR, GI, EL, BR and MS conceived the study and obtained funding. ADM managed the study, oversaw data retrieval, drafted and edited the manuscript. RJR designed the analytic approach, performed the final analysis and contributed to the drafting and editing of the final manuscript. IU performed a substantial portion of the analysis and contributed to early drafts of the manuscript. GI, EL, BR and MS reviewed results, interpreted findings and contributed to the revision of the manuscript. ADM takes responsibility for the manuscript as a whole.
Corresponding author
Ethics declarations
Conflict of interest
The authors have no other relevant conflicts of interest. The funding sources had no direct involvement in the study design, analysis, interpretation or decision to submit this work.
Supplementary Information
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
McRae, A.D., Rowe, B.H., Usman, I. et al. A comparative evaluation of the strengths of association between different emergency department crowding metrics and repeat visits within 72 hours. Can J Emerg Med 24, 27–34 (2022). https://doi.org/10.1007/s43678-021-00234-4
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s43678-021-00234-4