
Abstract
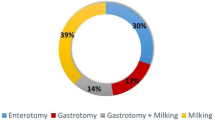
We present a series of 56 patients with gastrointestinal bezoar following previous gastric surgery for gastroduodenal peptic ulcer. The following parameters were studied: factors predisposing to bezoar formation (type of previous surgery, alimentation, and mastication), form of clinical presentation, diagnostic tests, and treatment. A bilateral truncal vagotomy plus pyloroplasty had been performed previously on 84% of patients, 44% revealed excessive intake of vegetable fiber, and 30% presented with bad dentition. The most frequent clinical presentation was intestinal obstruction (80%). This was diagnosed mainly by clinical data and simple abdominal radiology. The main exploratory technique for diagnosing cases of gastric bezoar was endoscopy. Surgery is necessary for treating the intestinal forms, and one should always attempt to fragment the bezoar and milk it to the cecum, reserving enterotomy and extraction for cases where this is not possible. The small intestine and stomach should always be explored for retained bezoars. Gastric bezoars should always receive conservative treatment, endoscopic extraction, and/or enzymatic dissolution; gastrotomy and extraction should be performed when this fails.
Similar content being viewed by others


References
Siffert G: Cuerpos extraños en el estómago.In HL Bockus (ed). Gastroenterología. Tomo I. Exploración del paciente. Esófago. Estómago. 3rd ed. Barcelona, Ed. Salvat, 1980, pp 1130–1134
Vilar Bonet J: Bezoares en operados del estómago: dos observaciones con oclusión intestinal. Rev. Quir. Esp 5(2):100–107, 1973
Baudamant WW: Memoire sur des cheveux trouves dans l'estomac, et dans les intestines grêles. J.D. Med 52:507, 1779
DeBakey M, Ochsner A: Bezoars and concretions: Comprehensive review of literature, with analysis of 303 collected cases and presentation of eight additional cases. Surgery 5:132–160, 1939
Norberg PB: Intestinal obstruccion due to citrus fruits after partial gastrectomy. Acta Chir Scand 109:43–47, 1955
Moseley DAJ: Diosphytobezoar in the postgastrectomy stomach. Arch Surg 71:946–948, 1955
Mir AM: Phytobezoar after vagotomy with drainaje or resection. Br J Surg 60(1):846–849, 1973
Galera FJ, Illana J, Morcillo M, Sanchez Bueno F, et al: Bezoares de estómago e intestino delgado. Revisión a propósito de 20 casos. Cir Esp 37(1):51–62, 1983
Calabuig R, Navarro S, Carrió I, Artigas V, Mones J, Puig Lacalle J: Gastric emptying and bezoar. Am J Surg 157:287–290, 1989
Robles Campos R, Parrilla Paricio P, Aguayo Albasini JL, Riquelme Riquelme J, Cifuentes Tébar J, Luján Mompeán JA, Garcia Ayllón J: Gastrointestinal bezoars. Presentation of 60 cases. Dig Surg 7:39–44, 1990
Kott I, Urca I, Tivka P: Intestinal obstruction after partial gastrectomy due to orange pith. Arch Surg 100:79–81, 1970
Buchholz RR, Haisten AS: Phytobezoars following gastric surgery for duodenal ulcer. Surg Clin North Am 52:341–352, 1972
Cain GB, Moore P Jr, Patterson M: Bezoars: A complication of the postgastrectomy state. Am J Dig Dis 13:801–809, 1968
Malagelada JR, Rees WDW, Mazzotta L, Go VLW: Gastric motor abnormalities in diabetic and postvagotomy gastroparesis: Effect of metoclopramide and bethanecol. Gastroenterology 78:286–293, 1980
Martinez de Haro LF: Motilidad del antro gástrico y su coordinación con el duodeno durante el periodo postprandial. Estudio experimental en perros. Cir Esp 41:281–287, 1987
Jahnberg T: Gastric adaptive relaxation. Scand J Gastroenterol 12(suppl 48):1, 1977
Johnson HD: The pylorus its function and some surgical considerations. Proc R Soc Med 54:938–940, 1961
Rogers LF, Davis EK, Harle TS: Phytobezoar formation and food boli following gastric surgery. Am J Roentgenol Radium Ther Nucl Med 119:280–290, 1973
Schlang HA: Acetylcysteine in removal of bezoar. JAMA 214:1329–1331, 1970
Goldstein HM, Cohen LE, Hagen RO, Wells RF: Gastric bezoars: A frequent complication in the postoperative ulcer patient. Radiology 107:341–344, 1973
Zurita M, Lago J, Marti A, Llobera M, Soto JA: Fitobezoares: Obstrucciones gástricas e intestinales. Barcelona Quir 29:166–171, 1979
Dieatrich NA, Gau FC: Postgastrectomy phytobezoars: Endoscopy diagnosis and treatment. Arch Surg 120:432–435, 1985
Klammer TW, Max MH: Recurrent gastric bezoars. A new approach to treatment and prevention. Am J Surg 45:417–419, 1983
Mangold D, Woolamm GL, Garcia-Rinaldi R: Intestinal obstruction due to phytobezoars. Arch Surg 113:1001–1003, 1978
Eliakim R, Fich A, Libson E, Katz E, Rach Milewit D: Crohn's disease of the duodeum presented as pancreatitis due to persimmon bezoar. J Clin Gastroenterol 9:553–555, 1987
Kadian RS, Rose JF, Mann MS: Gastric bezoars. Spontaneous resolution. Am J Gastroenterol 70:79–82, 1978
Zarling EI, Moeller DD: Bezoar therapy: Complications using Adolph's meat tenderizer and alternatives from literature review. Arch Intern Med 141:1669–1670, 1983
Deal DR, Vitah P, Raffin SB: Dissolution of a postgastrectomy bezoar by cellulase. A rapid noninterventive technique. Gastroenterology 64:467–469, 1973
Holloway WD, Lee SP, Nicholson GL: The composition and dissolution of phytobezoars. Arch Pathol Lab Med 104:159–161, 1980
Aguayo JL, Galera FJ, Morcillo M, et al: Tratamiento conservador del bezoar gástrico mediante fragmentación endoscópica. Rev Quir Esp 14(4):235–237, 1987
Brady PG: Gastric phytobezoars consequent to delayed gastric emptying. Gastrointest Endosc 24:159–161, 1978
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Cifuentes Tebar, J., Robles Campos, R., Parrilla Paricio, P. et al. Gastric surgery and bezoars. Digest Dis Sci 37, 1694–1696 (1992). https://doi.org/10.1007/BF01299861
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/BF01299861