
Abstract
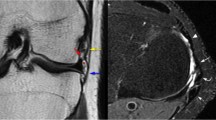
The purpose of this study was to evaluate the influence of the graft positioning on the clinical outcome and magnetic resonance imaging (MRI) signal of the graft following anterior cruciate ligament (ACL) reconstruction using the central one-third of the patellar tendon. Twentytwo patients with a chronic anterior instability underwent a modified Marshall-MacIntosh procedure, while 27 with a subacute torn ACL had an ACL reconstruction using a free bone-patellar tendon-bone graft. The patients were retrospectively reviewed with a 1.8-year average followup (1–3 years). The clinical result was evaluated through the comparative range of motion and the residual laxity as measured with the KT 1000 arthrometer. The roentgenographic analysis was performed from anteroposterior (AP) and mediolateral (ML) views, made first on one-leg standing with the knee at 30° of flexion, and secondly at “zero” extension with active quadriceps contraction. Lines were drawn to visualise the location of the tibial and femoral tunnels in relation to the tibial plateaus and the intercondylar roof represented by Blumensaat's line. The analysis of the lateral MRI views of the graft allowed discrimination between homogenous and heterogenous graft signals. On lateral roentgenograms of normal knees, it was found that Blumensaat's line crossed the surface of the medial tibial plateau at 30%±9% of its sagittal width (20%–40% range), demonstrating the variability of intercondylar roof inclination. The range of motion was normal in 34 patients (group I), 9 patients had a flexion deficit (group II), and 6 exhibited an extension deficit (group III). The residual laxity was similar in each group (P>0.05). When comparing group III to group I, patients from the former group had a tibial tunnel significantly more anterior with regard to Blumensaat's line (P=0.02). In group III, all patients exhibited a heterogenous MRI graft signal (P<0.05). and the angle between the intra-articular part of the graft and the tibial tunnel was higher (P<0.001). These findings were not observed in group II where the location only of the femoral tunnel seemed to influence the flexion deficit (P<0.05). This study demonstrated that the location of the tibial tunnel with regard to the intercondylar roof, when the knee is at “zero” extension, was the most relevant parameter in control of the extension deficit resulting from a graft impingement. No relation was found between the tibial tunnel location with regard to the tibial plateaus and the mobility deficit. Also, graft impingement was always associated with a heterogenous graft MRI signal. When reconstructing the ACL, care must be taken when inserting the K-wire aimed to guide the tibial drill to obtain a proper position with regard to the roof of the intercondylar notch. The K-wire location must be checked at “zero” extension. Intraoperative X-rays may help.
Similar content being viewed by others


References
Aglietti P, Buzzi R, D'Andria S, Zaccherotti G (1992) Long term study of anterior cruciate ligament reconstruction for chronic instability using the central one-third patellar tendon and a lateral extraarticular tenodesis. Am J Sports Med 20: 38–45
Arms SW, Pope MH, Johnson RJ et al (1984) The biomechanics of anterior cruciate ligament rehabilitation and reconstruction. Am J Sports Med 12: 8–18
Berns GS, Howell SM (1993) Roofplasty requirements in vitro for different tibial hole placements in anterior cruciate ligament reconstruction. Am J Sports Med 21: 292–298
Bradley J, Fitzpatrick D, Daniel D, Shertcliff T, O'Connor J (1988) Orientation of the cruciate ligament in the sagittal plane. J Bone Joint Surg [Br] 70: 94–99
Burks RT (1990) Gross anatomy in: Daniel D et al (eds) Knee ligaments: structure, function, injury, and repair. Raven Press, New York, pp 59–76
Christel P, Roger B, Witvoet J, Laval Jeantet M, Cabanis EA (1988) Valeur et intérêt diagnostiques de l'imagerie par résonance magnétique dans la pathologie ménisco-ligamentaire traumatique du genou. Rev Chir Orthop 74: 402–412
Christel P, Djian P, Darman Z, Witvoet J (1993) Etude des résultats de l'intervention de Marshall-macIntosh selon trois systèmes d'évaluation (ARPEGE, Lysholm, IKDC). Rev Chir Orthop 79: 473–483
Clancy W, Nelson D, Reider B, Narechania R (1982) Anterior cruciate ligament reconstruction using one-third patellar ligament augmented by extraarticular tendon transfer. J Bone Joint Surg [Am] 64: 352–359
Daniel MD, Penner DA, Burks RT (1988) Anterior cruciate ligament graft isometry and tensioning. In: Friedman MJ, Ferkel RD (eds) Prosthetic ligament reconstruction of the knee, Saunders, Philadelphia, pp 17–21.
Davis P, Crook L, Arakawa M, McRee R, Kaufman L, Margulis A (1981) NMR characteristics of the normal and abnormal rat tissues. In: Kaufman L, Crook L, Margulis A (eds) Nucleart magnetic imaging medicine. Igasu-shoin, Tokyo, pp 71–100
Djian P, Christel P, Fossier E, Witvoet J (1993) Traitement des ruptures récentes du ligament croisé antérieur selon la technique du transplant libre de tendon rotulien avec tunnel fémoral borgne. J Traumatol Sport 10: 230–240
Dorlot JM, Christel P, Witvoët J, Sedel L (1984) Déplacement des insertions des ligaments croisés durant la flexion du genou normal. Rev Chir Orthop 70 [Suppl 2]: 50–53
Friederich NF, Müller W (1993) How important is isometric placement of cruciate ligament grafts: intraoperative measurement vs mid-term clinical follow-up (1st European Congress of Orthopaedics, Paris, 1993). Rev Chir Orthop 79 (Spécial): abstract 443
Fullerton LR, Andrews JR (1984) Mechanical block to extension following augmentation of the anterior cruciate ligament: a case report Am J Sports Med 12: 166–168
Graf BK (1987) Isometric placement of substitutes for the anterior cruciate ligament. In: Jackson DW, Drez DJ (eds) The anterior cruciate deficient knee. Mosby, St Louis, pp 102–113
Grood ES (1992) Placement of knee ligament grafts. In: Finerman GAM, Noyes FR (eds) Biology and biomechanics of the traumatized synovial joint: the knee as a model. American Academy of Orthopaedic Surgeons. Rosemont, pp. 393–417
Harner CD, Irrgang JJ, Paul JJ, Dearwater S, Fu FH (1992) Loss of motion after anterior cruciate ligament reconstruction. Am J Sports Med 20: 499–506
Hoogland T, Hillen B (1984) Intra-articular reconstruction of the anterior cruciate ligament. An experimental study of length changes in different ligament reconstructions. Clin Orthop 185: 197–202
Howell SM, Clark JA (1992) Tibial tunnel placement in anterior cruciate ligament reconstructions and graft impingement. Clin Orthop 283: 187–195
Howell SM, Taylor MA (1993) Failure of reconstruction of the anterior cruciate ligament due to impingement by the intercondylar roof. J Bone Joint Surg [Am] 75: 1044–1055
Howell SM, Clark JA, Farley TE (1991) A rationale for predicting anterior cruciate graft impingement by the intercondylar roof: a magnetic resonance imaging study. Am J Sports Med 19: 276–282
Howell SM, Berns G, Faley TE (1991) Unimpinged and impinged anterior cruciate ligament grafts: MR signal intensity measurement. Radiology 179: 639–643
Howell SM, Clark JA, Farley TE (1992) Serial magnetic resonnance study assessing the effects of impingement on the MR image of the patellar tendon graft. Arthroscopy 8: 350–358
Jackson DW, Drez D Jr (1987) Isometric placement of substitution for the anterior cruciate deficient knee. In: Jackson DW, Drez D Jr (eds) The anterior cruciate deficient knee. Mosby, St Louis, pp 102–113
Jackson DW, Schaefer RK (1990) Cyclops syndrome: loss of extension following intra-articular cruciate ligament reconstruction. Arthroscopy 6: 171–178
Jones KG (1963) Reconstruction of the anterior cruciate ligament: a technique using the central one-third of the patellar ligament. J Bone Joint Surg [Am] 45: 925–932
Maywood RM, Murphy BJ, Uribe JW, Hechtman KS (1993) Evaluation of arthroscopic anterior cruciate ligament reconstruction using magnetic resonance imaging. Am J Sports Med 21: 523–527
Moeser P, Bechtold RE, Clark T (1989) Imaging of the anterior cruciate ligament repair. J Comput Assist Tomogr 13: 105–109
Mohtadi NG, Webster-Bogaert S, Fowler PJ (1991) Limitation of motion following anterior cruciate ligament reconstruction. A case-control study. Am J Sports Med 19: 620–636
Muneta T, Yamamoto H, Sakai H, Ishibashi T, Furuya K (1993) Relationship between changes in length and force of in vitro reconstructed anterior cruciate ligament. Am J Sports Med 21: 299–304
Noyes FR, Keller CS, Grood ES (1984) Advances in the understanding of knee ligament injury, repair, and rehabilitation. Med Sci Sports Exerc 16: 427–443
O'Brien WR, Henning CE (1987) Anterior cruciate ligament substitute load versus tibial positioning: an in vitro study. Am J Sports Med 15: 398
Odensten M, Gillquist J (1985) Functional anatomy of the anterior cruciate ligament and a rationale for reconstruction. J Bone Joint Surg [Am] 67: 257–262
Penner DA, Daniel DM, Wood P, Mishra D (1988) An in vitro study of anterior cruciate ligament graft placement and isometry. Am J Sports Med 16: 238–243
Rack RM, Gillogly SD, Schaefer RA (1991) Anterior cruciate ligament reconstruction: evaluation with magnetic resonance imaging. Radiology 178: 553–556
Romano VM, Graf BK, Keene JS, Lange RH (1993) Anterior cruciate ligament reconstruction. The effect of tibial tunnel placement on range of motion. Am J Sports Med 21: 415–418
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Djian, P., Christel, P., Roger, B. et al. Roentgenographic and magnetic resonance imaging of anterior cruciate reconstruction using a patellar tendon graft —correlations with physical findings. Knee Surg, Sports traumatol, Arthroscopy 2, 207–213 (1994). https://doi.org/10.1007/BF01845589
Issue Date:
DOI: https://doi.org/10.1007/BF01845589