
Background and Purpose:
Locoregional relapse is a problem frequently encountered with advanced gastric cancer. Data from the randomized Intergroup trial 116 suggest effectiveness of adjuvant radiochemotherapy, albeit with significant toxicity. The potential of intensity-modulated radiotherapy (IMRT) to reduce toxicity by significantly reducing maximum and median doses to organs at risk while still applying sufficient dose to the target volume in the upper abdomen was studied.
Patient and Methods:
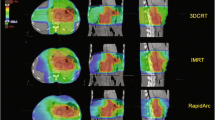
For a typical configuration of target volumes and organs, a step-and-shoot IMRT plan (eight beam orientations), developed as a class solution for treatment of tumors in the upper abdomen (Figures 1 to 3), a conventional plan, a combination of the conventional plan with a kidney-sparing boost plan, and a conventional plan with noncoplanar ap and pa fields for improved kidney sparing were compared with respect to coverage of target volume and dose to organs at risk with a dose of 45 Gy delivered as the median dose to the target volume.
Results:
When using the conventional three-dimensionally planned box techniques, the right kidney could be kept below tolerance, but median dose to the left kidney amounted to between 14.8 and 26.9 Gy, depending on the plan. IMRT reduced the median dose to the left kidney to 10.5 Gy, while still keeping the dose to the right kidney < 8 Gy. Liver was spared better with IMRT. Dose to the lungs was not significantly different, and dose to the spinal cord was higher (but well below tolerance) with IMRT. The dose distribution within the target volume was less homogeneous than for the conventional plans. With regard to target coverage, > 90% of prescription dose were delivered to > 90% of target volume with IMRT (Table 1).
Conclusion:
IMRT has the potential to deliver efficient doses to target volumes in the upper abdomen, while delivering dose to organs at risk in a more advantageous fashion than a conventional technique. For clinical implementation, the possibility of extensive organ motion in the upper abdomen has to be taken into account for treatment planning and patient positioning. The multitude of potential risks related to its application has to be the subject of thorough follow-up and further studies.
Hintergrund und Ziel:
Die adjuvante Therapie des fortgeschrittenen Magenkarzinoms wird kontrovers diskutiert. Der Intergroup- Trial 116 wies jedoch erstmals die prinzipielle Effizienz einer adjuvanten Radiochemotherapie nach. Des Weiteren stellt bei suffizienter strahlentherapeutischer Einfassung der Zielregion jedoch die Toxizität dieser Behandlungsstrategie ein Problem dar. Es wurde daher versucht, durch Einsatz der intensitätsmodulierten Strahlentherapie (IMRT) bei einem typischen Zielvolumen im Oberbauch die mediane und maximale Risikoorganbelastung bei vergleichbarer Zielvolumenabdeckung zu reduzieren.
Patient und Methodik:
Für eine typische Konfiguration von Zielvolumen und Risikoorganen wurden eine als „class solution“ entwickelte Acht-Felder-IMRT-Technik (Abbildungen 1 bis 3), ein konventioneller Plan, eine Kombination dieses konventionellen Plans mit einem nierenschonenden Boostplan und ein konventioneller Plan mit nonkoplanarer Ausrichtung von a.p. und p.a. Feld zur besseren Nierenschonung hinsichtlich Zielvolumeneinfassung und Belastung der Risikoorgane verglichen.
Ergebnisse:
Mit konventionellen Techniken konnte zwar die rechte Niere ausreichend geschont werden, die linke Niere wurde jedoch je nach Plan mit einer medianen Dosis zwischen 14,8 und 26,9 Gy belastet. IMRT reduzierte die mediane linksseitige Nierendosis auf 10,5 Gy, während die mediane rechtsseitige Nierendosis immer noch < 8 Gy gehalten werden konnte. Die Leberbelastung war bei IMRT ebenfalls reduziert. Die Lungendosen unterschieden sich nicht wesentlich. Die Rückenmarkdosis war bei IMRT höher als bei konventioneller Bestrahlung, jedoch deutlich unter der Toleranz. Die Dosisverteilung im Zielvolumen war bei IMRT inhomogener, auch mittels IMRT konnten zuverlässig > 90% der Verschreibungsdosis auf > 90% des Zielvolumens appliziert werden (Tabelle 1).
Schlussfolgerung:
IMRT moduliert die Belastung der Risikoorgane im Oberbauch gegenüber einer konventionell 3-D-geplanten Technik günstiger, sodass Ausschöpfung und Einhaltung der Organtoleranzen erleichtert werden. Bei der klinischen Implementierung muss die besondere Mobilität der Oberbauchorgane bei der Planung und der Patientenpositionierung berücksichtigt werden. Die zahlreichen technischen und biologischen Unwägbarkeiten der Anwendung der IMRT insbesondere in dieser Region erfordern die vorsichtige Implementierung, langfristige Nachbeobachtung und weitere Untersuchungen.
Similar content being viewed by others


Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Lohr, F., Dobler, B., Mai, S. et al. Optimization of Dose Distributions for Adjuvant Locoregional Radiotherapy of Gastric Cancer by IMRT. Strahlenther Onkol 179, 557– 563 (2003). https://doi.org/10.1007/s00066-003-1087-z
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1007/s00066-003-1087-z