
Abstract
Background
Primary chemoradiotherapy (CRT) is the standard treatment for locally advanced anal carcinoma. This study compared volumetric intensity-modulated arc therapy (VMAT) to 3-dimensional conformal radiotherapy (3DCRT) in terms of treatment-related side effects and survival.
Patients and methods
From 1992–2014, 103 consecutive patients with anal carcinoma UICC stage I–III were treated. Concomitant CRT consisted of whole pelvic irradiation, including the iliac and inguinal lymph nodes, with 50.4 Gy (1.8 Gy per fractions) by VMAT (n = 17) or 3DCRT (n = 86) as well as two cycles of 5-fluorouracil and mitomycin C. Acute organ and hematological toxicity were assessed according to the Common Terminology Criteria (CTC) for Adverse Events version 3.0. Side effects ≥ grade 3 were scored as high-grade toxicity.
Results
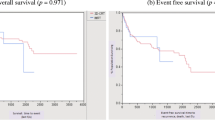
High-grade acute organ toxicity CTC ≥ 3 (P < 0.05), especially proctitis (P = 0.03), was significantly reduced in VMAT patients. The 2-year locoregional control (LRC) and disease-free survival (DFS) were both 100 % for VMAT patients compared with 80 and 73 % for 3DCRT patients.
Conclusion
VMAT was shown to be a feasible technique, achieving significantly lower rates of acute organ toxicity and promising results for LRC and DFS. Future investigations will aim at assessing the advantages of VMAT with respect to late toxicity and survival after a prolonged follow-up time.
Zusammenfassung
Hintergrund
Die primäre Radiochemotherapie (RCT) gilt als Standardtherapie für lokal fortgeschrittene Analkarzinome. In dieser Studie wurde die volumetrisch modulierte Rotationstherapie („volumetric intensity-modulated arc therapy“, VMAT) mit der klassischen dreidimensionalen konformalen Radiotherapie (3DCRT) hinsichtlich therapieassoziierter Nebenwirkungen und Überleben verglichen.
Methoden
Von 1992–2014 wurden 103 aufeinanderfolgende Patienten mit einem Analkarzinom im UICC-Stadium I–III behandelt. Die kombinierte RCT bestand aus der Bestrahlung des gesamten Beckens inklusive der iliakalen und der inguinalen Lymphknoten mit einer Gesamtdosis von 50,4 Gy (1,8 Gy pro Fraktion) entweder mit VMAT (n = 17) oder 3DCRT (n = 86) sowie zwei begleitenden Chemotherapiezyklen mit 5-Fluorouracil und Mitomycin C. Alle akuten Organ- und/oder hämatologischen Nebenwirkungen wurden gemäß der Common Terminology Criteria (CTC) for Adverse Events Version 3.0 erfasst. Nebenwirkungen ≥ Grad 3 wurden als hochgradige Toxizität gewertet.
Ergebnisse
Die VMAT-Patienten entwickelten insgesamt signifikant weniger hochgradige (CTC ≥ 3) Akutnebenwirkungen an den Organen bzw. im gesunden Gewebe (P < 0,05), insbesondere die Proktitis (P = 0,03) war verringert. Die lokoregionäre Tumorkontrolle (LRC) und das erkrankungsfreie Überleben (DFS) lagen nach 2 Jahren bei 100 % für alle VMAT-Patienten verglichen mit 80 und 73 % für die 3DCRT-Patienten.
Schlussfolgerung
VMAT hat sich als eine praktikable Radiotherapietechnik bewiesen, die signifikant niedrigere Raten an akuter Organtoxizität und vielversprechende LRC- und DFS-Ergebnisse zeigt. Zukünftige Untersuchungen sollten darauf abzielen, die Vorteile von VMAT in Hinblick auf die Spättoxizität und das Langzeitüberleben zu analysieren.



Similar content being viewed by others


References
Siegel R, Naishadham D, Jemal A (2012) Cancer statistics, 2012. CA Cancer J Clin 62:10–29
Daling JR, Madeleine MM, Johnson LG et al (2004) Human papillomavirus, smoking, and sexual practices in the etiology of anal cancer. Cancer 101:270–280
Melbye M, Cote TR, Kessler L et al (1994) High incidence of anal cancer among AIDS patients. The AIDS/Cancer Working Group. Lancet 343:636–639
Hoots BE, Palefsky JM, Pimenta JM et al (2009) Human papillomavirus type distribution in anal cancer and anal intraepithelial lesions. Int J Cancer 124:2375–2383
Engstrom PF, Arnoletti JP, Benson AB 3rd et al (2010) NCCN clinical practice guidelines in oncology. Anal carcinoma. J Natl Compr Canc Netw 8:106–120
Gunderson LL, Winter KA, Ajani JA et al (2012) Long-term update of US GI intergroup RTOG 98-11 phase III trial for anal carcinoma: survival, relapse, and colostomy failure with concurrent chemoradiation involving fluorouracil/mitomycin versus fluorouracil/cisplatin. J Clin Oncol 30:4344–4351
Nigro ND, Vaitkevicius VK, Considine B Jr (1974) Combined therapy for cancer of the anal canal: a preliminary report. Dis Colon Rectum 17:354–356
n a (1996) Epidermoid anal cancer: results from the UKCCCR randomised trial of radiotherapy alone versus radiotherapy, 5-fluorouracil, and mitomycin. UKCCCR Anal Cancer Trial Working Party. UK Co-ordinating Committee on Cancer Research. Lancet 348:1049–1054
Bartelink H, Roelofsen F, Eschwege F et al (1997) Concomitant radiotherapy and chemotherapy is superior to radiotherapy alone in the treatment of locally advanced anal cancer: results of a phase III randomized trial of the European Organization for Research and Treatment of Cancer Radiotherapy and Gastrointestinal Cooperative Groups. J Clin Oncol 15:2040–2049
Das P, Crane CH, Ajani JA (2007) Current treatment for localized anal carcinoma. Curr Opin Oncol 19:396–400
Chen YJ, Liu A, Tsai PT et al (2005) Organ sparing by conformal avoidance intensity-modulated radiation therapy for anal cancer: dosimetric evaluation of coverage of pelvis and inguinal/femoral nodes. Int J Radiat Oncol Biol Phys 63:274–281
Lin A, Ben-Josef E (2007) Intensity-modulated radiation therapy for the treatment of anal cancer. Clin Colorectal Cancer 6:716–719
Menkarios C, Azria D, Laliberte B et al (2007) Optimal organ-sparing intensity-modulated radiation therapy (IMRT) regimen for the treatment of locally advanced anal canal carcinoma: a comparison of conventional and IMRT plans. Radiat Oncol 2:41
Milano MT, Jani AB, Farrey KJ et al (2005) Intensity-modulated radiation therapy (IMRT) in the treatment of anal cancer: toxicity and clinical outcome. Int J Radiat Oncol Biol Phys 63:354–361
Kachnic LA, Winter K, Myerson RJ et al (2013) RTOG 0529: a phase 2 evaluation of dose-painted intensity modulated radiation therapy in combination with 5-fluorouracil and mitomycin-C for the reduction of acute morbidity in carcinoma of the anal canal. Int J Radiat Oncol Biol Phys 86:27–33
Bazan JG, Hara W, Hsu A et al (2011) Intensity-modulated radiation therapy versus conventional radiation therapy for squamous cell carcinoma of the anal canal. Cancer 117:3342–3351
Chuong MD, Freilich JM, Hoffe SE et al (2013) Intensity-modulated radiation therapy vs. 3D conformal radiation therapy for squamous cell carcinoma of the anal canal. Gastrointest Cancer Res 6:39–45
Salama JK, Mell LK, Schomas DA et al (2007) Concurrent chemotherapy and intensity-modulated radiation therapy for anal canal cancer patients: a multicenter experience. J Clin Oncol 25:4581–4586
Cozzi L, Dinshaw KA, Shrivastava SK et al (2008) A treatment planning study comparing volumetric arc modulation with RapidArc and fixed field IMRT for cervix uteri radiotherapy. Radiother Oncol 89:180–191
Verbakel WF, Cuijpers JP, Hoffmans D et al (2009) Volumetric intensity-modulated arc therapy vs. conventional IMRT in head-and-neck cancer: a comparative planning and dosimetric study. Int J Radiat Oncol Biol Phys 74:252–259
Richetti A, Fogliata A, Clivio A et al (2010) Neo-adjuvant chemo-radiation of rectal cancer with volumetric modulated arc therapy: summary of technical and dosimetric features and early clinical experience. Radiat Oncol 5:14
Wolff HA, Wagner DM, Christiansen H et al (2010) Single fraction radiosurgery using Rapid Arc for treatment of intracranial targets. Radiat Oncol 5:77
Wolff D, Stieler F, Hermann B et al (2010) Clinical implementation of volumetric intensity-modulated arc therapy (VMAT) with ERGO++. Strahlenther Onkol 186:280–288
Pasler M, Georg D, Bartelt S et al (2013) Node-positive left-sided breast cancer: does VMAT improve treatment plan quality with respect to IMRT? Strahlenther Onkol 189:380–386
Cambria R, Cattani F, Jereczek-Fossa BA et al (2014) Planning study to compare dynamic and rapid arc techniques for postprostatectomy radiotherapy of prostate cancer. Strahlenther Onkol 190:569–574
Clivio A, Fogliata A, Franzetti-Pellanda A et al (2009) Volumetric-modulated arc radiotherapy for carcinomas of the anal canal: a treatment planning comparison with fixed field IMRT. Radiother Oncol 92:118–124
Myerson RJ, Garofalo MC, El Naqa I et al (2009) Elective clinical target volumes for conformal therapy in anorectal cancer: a radiation therapy oncology group consensus panel contouring atlas. Int J Radiat Oncol Biol Phys 74:824–830
Wolff HA, Wagner DM, Conradi LC et al (2012) Irradiation with protons for the individualized treatment of patients with locally advanced rectal cancer: a planning study with clinical implications. Radiother Oncol 102:30–37
Chavaudra J (1998) Last ICRU recommendations for the prescription, recording and reporting of external bean therapy. Cancer Radiother 2:607–614
n a (2010) Prescribing, recording, and reporting photon-beam intensity-modulated radiation therapy (IMRT): contents. J International Commission on Radiation Units and Measurements (ICRU) 10:NP
Trotti A, Colevas AD, Setser A et al (2003) CTCAE v3.0: development of a comprehensive grading system for the adverse effects of cancer treatment. Semin Radiat Oncol 13:176–181
Trotti A, Byhardt R, Stetz J et al (2000) Common toxicity criteria: version 2.0. an improved reference for grading the acute effects of cancer treatment: impact on radiotherapy. Int J Radiat Oncol Biol Phys 47:13–47
Cox JD, Stetz J, Pajak TF (1995) Toxicity criteria of the Radiation Therapy Oncology Group (RTOG) and the European Organization for Research and Treatment of Cancer (EORTC). Int J Radiat Oncol Biol Phys 31:1341–1346
Mok H, Briere TM, Martel MK et al (2011) Comparative analysis of volumetric modulated arc therapy versus intensity modulated radiation therapy for radiotherapy of anal carcinoma. Pract Radiat Oncol 1:163–172
Stieler F, Wolff D, Lohr F et al (2009) A fast radiotherapy paradigm for anal cancer with volumetric modulated arc therapy (VMAT). Radiat Oncol 4:48
Renard-Oldrini S, Brunaud C, Huger S et al (2012) Dosimetric comparison between the intensity modulated radiotherapy with fixed field and Rapid Arc of cervix cancer. Cancer Radiother 16:209–214
Foroudi F, Wilson L, Bressel M et al (2012) A dosimetric comparison of 3D conformal vs intensity modulated vs volumetric arc radiation therapy for muscle invasive bladder cancer. Radiat Oncol 7:111
Ajani JA, Winter KA, Gunderson LL et al (2008) Fluorouracil, mitomycin, and radiotherapy vs fluorouracil, cisplatin, and radiotherapy for carcinoma of the anal canal: a randomized controlled trial. JAMA 299:1914–1921
Acknowledgments
This manuscript was edited by the “American Journal Experts” editorial service. The results of this manuscript were presented as a poster presentation at the annual meeting of the DEGRO 2014 in Düsseldorf, Germany.
Funding Source
None.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
H.E. Weber, L.H. Dröge, S. Hennies, M.K. Herrmann, J. Gaedcke, and H.A. Wolff state that there are no conflicts of interest.
All studies on humans described in the present manuscript were carried out with the approval of the responsible ethics committee and in accordance with national law and the Helsinki Declaration of 1975 (in its current, revised form).
Rights and permissions
About this article

Cite this article
Weber, H., Dröge, L., Hennies, S. et al. Volumetric intensity-modulated arc therapy vs. 3-dimensional conformal radiotherapy for primary chemoradiotherapy of anal carcinoma. Strahlenther Onkol 191, 827–834 (2015). https://doi.org/10.1007/s00066-015-0859-6
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00066-015-0859-6