
Abstract
Summary
Fractures are common in chronic kidney disease (CKD). We determined if bone mineral density testing by dual energy X-ray absorptiometry (DXA) and high resolution peripheral quantitative computed tomography (HR pQCT) could discriminate fracture status in CKD patients. Both tests were able to discriminate fracture status. Further, the addition of HR pQCT measurements to DXA measurements did not improve fracture discrimination.
Introduction
The optimal method to identify individuals with CKD at high fracture risk is unknown.
Methods
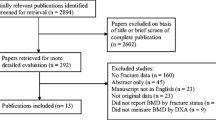
We determined if bone mineral density (BMD) by DXA and HR pQCT could discriminate fracture status in 211 adult men and women with stages 3 to 5 CKD, attending predialysis clinics in Toronto Canada, using logistic regression. Results are expressed as the odds ratio (OR) of fracture (prevalent vertebral and/or low trauma since age 40 years) per standard deviation decrease in the predictor adjusted for age, weight, sex, and CKD stage. We constructed receiver operating characteristic curves to examine the discriminative ability of BMD measures for fracture.
Results
Most participants were Caucasian men with a mean age of 63.3 ± 15.5 years. There were 77 fractures in 74 participants. Decreases in BMD were associated with increased fracture risk: OR = 1.56 (95% confidence interval (CI), 1.41 to 1.71) for BMD by DXA at the ultradistal radius, and OR = 1.24 (95% CI, 1.12 to 1.36) for cortical area by HR pQCT. Further, while both tests were able to discriminate fracture status, the addition of HR pQCT measures to BMD by DXA did not improve fracture discrimination ability.
Conclusions
Among CKD patients not yet requiring renal replacement therapy, BMD by DXA is able to discriminate fracture status.

Similar content being viewed by others


References
Lindberg JS, Moe SM (1999) Osteoporosis in end-state renal disease. Semin Nephrol 19:115–122
Yamaguchi T, Kanno E, Tsubota J, Shiomi T, Nakai M, Hattori S (1996) Retrospective study on the usefulness of radius and lumbar bone density in the separation of hemodialysis patients with fractures from those without fractures. Bone 19:549–555
Fontaine MA, Albert A, Dubois B, Saint-Remy A, Rorive G (2000) Fracture and bone mineral density in hemodialysis patients. Clin Nephrol 54:218–226
Jamal S, Chase C, Goh Y, Richardson R, Hawker G (2002) Bone density and heel ultrasound testing do not identify patients with dialysis-dependent renal failure who have had fractures. Am J Kidney Dis 39:843–849
Kaji H, Suzuki M, Yano S, Sugimoto T, Chihara K, Hattori S, Sekita K (2002) Risk factors for hip fracture in hemodialysis patients. Am J Nephrol 22:325–331
Jamal SA, Hayden JA, Beyene J (2007) Low bone mineral density and fractures in long-term hemodialysis patients: a meta-analysis. Am J Kidney Dis 49:674–681
Dolgos S, Hartmann A, Bonsnes S, Ueland T, Isaksen GA, Godang K, Pfeffer P, Bollerslev J (2008) Determinants of bone mass in end-stage renal failure patients at the time of kidney transplantation. Clin Transplant 22:462–468
Elder GJ, Mackun K (2006) 25-Hydroxyvitamin D deficiency and diabetes predict reduced BMD in patients with chronic kidney disease. J Bone Miner Res 21:1778–1784
Ersoy FF, Passadakis SP, Tam P, Memmos ED, Katopodis PK, Ozener C, Akcicek F, Camsari T, Ates K, Ataman R, Vlachojannis JG, Dombros AN, Utas C, Akpolat T, Bozfakioglu S, Wu G, Karayaylali I, Arinsoy T, Stathakis PC, Yavuz M, Tsakiris JD, Dimitriades CA, Yilmaz ME, Gultekin M, Karayalcin B, Yardimsever M, Oreopoulos DG (2006) Bone mineral density and its correlation with clinical and laboratory factors in chronic peritoneal dialysis patients. J Bone Miner Metab 24:79–86
Nickolas TL, Stein E, Cohen A, Thomas V, Staron RB, McMahon DJ, Leonard MB, Shane E (2010) Bone mass and microarchitecture in CKD patients with fracture. J Am Soc Nephrol 21:1371-1380.
Russo CR, Taccetti G, Caneva P, Mannarino A, Maranghi P, Ricca M (1998) Volumetric bone density and geometry assessed by peripheral quantitative computed tomography in uremic patients on maintenance hemodialysis. Osteoporos Int 8:443–448
Jamal SA, Gilbert J, Gordon C, Bauer DC (2006) Cortical PQCT measures are associated with fractures in dialysis patients. J Bone Miner Res 21:543–548
Hasegawa K, Hasegawa Y, Nagano A (2004) Estimation of bone mineral density and architectural parameters of the distal radius in hemodialysis patients using peripheral quantitative computed tomography. J Biomech 37:751–756
Nickolas TL, McMahon DJ, Shane E (2006) Relationship between moderate to severe kidney disease and hip fracture in the United States. J Am Soc Nephrol 17:3223–3232
Ensrud KE, Lui LY, Taylor BC, Ishani A, Shlipak MG, Stone KL, Cauley JA, Jamal SA, Antoniucci DM, Cummings SR (2007) Renal function and risk of hip and vertebral fractures in older women. Arch Intern Med 167:133–139
Coresh J, Selvin E, Stevens LA, Manzi J, Kusek JW, Eggers P, Van Lente F, Levey AS (2007) Prevalence of chronic kidney disease in the United States. JAMA 298:2038–2047
(2002) K/DOQI clinical practice guidelines for chronic kidney disease: evaluation, classification, and stratification. Am J Kidney Dis 39:S1-266.
(1994) Assessment of osteoporotic fracture risk and its role in screening for postmenopausal osteoporosis. WHO Technical Series, Geneva.
Black DM, Palermo L, Nevitt MC, Genant HK, Christensen L, Cummings SR (1999) Defining incident vertebral deformity: a prospective comparison of several approaches. The study of Osteoporotic Fractures Research Group. J Bone Miner Res 14:90–101
Genant HK, Jergas M, Palermo L, Nevitt M, Valentin RS, Black D, Cummings SR (1996) Comparison of semiquantitative visual and quantitative morphometric assessment of prevalent and incident vertebral fractures in osteoporosis. The Study of Osteoporotic Fractures Research Group. J Bone Miner Res 11:984–996
Boutroy S, Bouxsein ML, Munoz F, Delmas PD (2005) In vivo assessment of trabecular bone microarchitecture by high-resolution peripheral quantitative computed tomography. J Clin Endocrinol Metab 90:6508–6515
Vico L, Zouch M, Amirouche A, Frere D, Laroche N, Koller B, Laib A, Thomas T, Alexandre C (2008) High-resolution pQCT analysis at the distal radius and tibia discriminates patients with recent wrist and femoral neck fractures. J Bone Miner Res 23:1741–1750
Hanley JA, McNeil BJ (1983) A method of comparing the areas under receiver operating characteristic curves derived from the same cases. Radiology 148:839–843
McClish DK (1987) Comparing the areas under more than two independent ROC curves. Med Decis Making 7:149–155
Miller PD, Roux C, Boonen S, Barton IP, Dunlap LE, Burgio DE (2005) Safety and efficacy of risedronate in patients with age-related reduced renal function as estimated by the Cockcroft and Gault method: a pooled analysis of nine clinical trials. J Bone Miner Res 20:2105–2115
Jamal SA, Bauer DC, Ensrud KE, Cauley JA, Hochberg M, Ishani A, Cummings SR (2007) Alendronate treatment in women with normal to severely impaired renal function: an analysis of the fracture intervention trial. J Bone Miner Res 22:503–508
Ishani A, Blackwell T, Jamal SA, Cummings SR, Ensrud KE (2008) The effect of raloxifene treatment in postmenopausal women with CKD. J Am Soc Nephrol 19:1430–1438
Miller PD, Schwartz EN, Chen P, Misurski DA, Krege JH (2007) Teriparatide in postmenopausal women with osteoporosis and mild or moderate renal impairment. Osteoporos Int 18:59–68
Miller PD (2009) Diagnosis and treatment of osteoporosis in chronic renal disease. Semin Nephrol 29:144–155
Duan Y, De Luca V, Seeman E (1999) Parathyroid hormone deficiency and excess: similar effects on trabecular bone but differing effects on cortical bone. J Clin Endocrinol Metab 84:718–722
Elder G (2002) Pathophysiology and recent advances in the management of renal osteodystrophy. Bone and Mineral Research 17:2094–2105
(2009) KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of chronic kidney disease-mineral and bone disorder (CKD-MBD). Kidney International S1-130.
Acknowledgments
The authors would like to thank Paul Miller for his careful review of this manuscript. Funding was provided by the Canadian Institutes of Health Research (FRN: 93785), the Physicians Services Incorporated Foundation, and The Kidney Foundation of Canada. Some results of this study were presented in abstract format at the 2010 ASN Renal Week and in abstract format at the 2010 and 2011 American Society for Bone and Mineral Research Annual Meeting.
Conflicts of interest
None.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jamal, S.A., Cheung, A.M., West, S.L. et al. Bone mineral density by DXA and HR pQCT can discriminate fracture status in men and women with stages 3 to 5 chronic kidney disease. Osteoporos Int 23, 2805–2813 (2012). https://doi.org/10.1007/s00198-012-1908-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00198-012-1908-y