
Abstract
Purpose
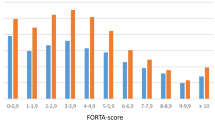
The feasibility of applying the Fit fOR The Aged (FORTA) list, a drug classification combining positive and negative labeling of drugs, should be studied in geriatric patients and medication quality and clinical endpoints measured. FORTA labels range from A (indispensable), B (beneficial), C (questionable) to D (avoid).
Methods
A prospective randomized controlled pilot trial was performed in hospitalized geriatric patients in whom the FORTA instrument or standard care was applied. Patients were randomly admitted to an intervention and a control ward. Changes of FORTA label distributions between admission and discharge, over- and under-prescription rates, clinical endpoints including the number of falls during the hospitalization, and Barthel Index (BI) at admission and discharge were measured.
Results
Polypharmacy persisted in both groups. At discharge, a higher rate of A drugs was prescribed in the intervention group (58 patients, median age 84 years) vs. standard care (56 patients, median age 83 years, p < 0.02), and both over- and under-prescriptions were significantly lower in the FORTA than in the control group (p < 0.03). Two (3.4 %) intervention, but 12 (21.4 %) control, patients fell at least once (p < 0.001). The fall rate per 1,000 patient years was 1.5 ± 8.3 in the intervention and 10.6 ± 25.4 in the control group (p < 0.004).
Conclusions
This pilot study shows that the application of the FORTA list is feasible in geriatric patients. In this small study, the medication quality improved in the intervention group, but polypharmacy persisted in both groups. The fall rate was significantly lower in the intervention group. These encouraging results must be interpreted carefully.


Similar content being viewed by others


References
Kaufman DW, Kelly JP, Rosenberg L, Anderson TE, Mitchell AA (2002) Recent patterns of medication use in the ambulatory adult population of the United States: the Slone Survey. JAMA 287:337–344
Varallo FR, Capucho HC, Planeta CS, Mastroianni Pde C (2011) Safety assessment of potentially inappropriate medications (PIMs) use in older people and the factors associated with hospital admission. J Pharm Pharmaceut Sci 14:283–290
American Geriatrics Society 2012 Beers Criteria Update Expert Panel (2012) American Geriatrics Society updated Beers Criteria for potentially inappropriate medication use in older adults. J Am Geriatr Soc 60:616–631
Gallagher P, O’Mahony D (2007) STOPP (Screening Tool of Older Person’s potentially inappropriate Prescriptions): application to acutely ill elderly patients and comparison with Beer’s criteria. Age Ageing 37:673–679
Holt S, Schmiedl S, Thürmann PA (2010) Potentially inappropriate medications in the elderly: the Priscus list. Dtsch Arztebl Int 107:543–551
Siebert S, Elkeles B, Hempel G, Kruse J, Smollich M (2013) The PRISCUS list in clinical routine. Practicability and comparison to international PIM lists. Z Gerontol Geriatr 46:35–47
Dormann H, Sonst A, Müller F et al (2013) Adverse drug events in older patients admitted as an emergency—the role of potentially inappropriate medication in elderly people (PRISCUS). Dtsch Arztebl Int 110:213–219
Hanlon JT, Schmader KE, Samsa GP et al (1992) A method for assessing drug therapy appropriateness. J Clin Epidemiol 45:1045–1051
Page RL, Ruscin JM (2006) The risk of adverse drug events and hospital-related morbidity and mortality among older adults with potentially inappropriate medication use. Am J Geriatr Pharmacother 4:297–305
Gallagher PF, O’Connor MN, O’Mahony D (2011) Prevention of potentially inappropriate prescribing for elderly patients: a randomized controlled trial using STOPP/START criteria. Clin Pharmacol Ther 89:845–854
Gallagher P, Ryan C, Byrne S, Kennedy J, O’Mahony D (2008) STOPP (Screening Tool of Older Person’s Prescriptions) and START (Screening Tool to Alert Doctors to Right Treatment). Consensus validation. Int J Clin Pharmacol Ther 46:72–83
Lam MPS, Cheung BMY (2012) The use of STOPP/START criteria as a screening tool for assessing the appropriateness of medications in the elderly population. Expert Rev Clin Pharmacol 5:187–197
Hill-Taylor B, Sketris I, Hayden J, Byrne S, O’Sullivan D, Christie R (2013) Application of the STOPP/START criteria: a systematic review of the prevalence of potentially inappropriate prescribing in older adults, and evidence of clinical, humanistic and economic impact. J Clin Pharm Ther 38:360–372
Ryan C, O’Mahony D, O’Donovan DO, O’Grady E, Weedle P, Kennedy J, Byrne S (2013) A comparison of the application of STOPP/START to patients’ drug lists with and without clinical information. Int J Clin Pharm 35:230–235
Wehling M (2009) Multimorbidity and polypharmacy: how to reduce the harmful drug load and yet add needed drugs in the elderly? Proposal of a new drug classification: fit for the aged. J Am Geriatr Soc 57:560–561
Kuhn-Thiel AM, Weiß C, Wehling M; The FORTA authors/expert panel members (2014) Consensus validation of the FORTA (Fit fOR The Aged) List: a clinical tool for increasing the appropriateness of pharmacotherapy in the elderly. Drugs Aging 31:131–140.
Wehling M (2013) Drug therapy for the elderly. Springer Publishers, Vienna, Austria
Frohnhofen H, Michalek C, Wehling M (2011) Assessment of drug treatment in geriatrics with the new FORTA criteria—preliminary clinical experience. Dtsch Med Wochenschr 136:1417–1421
Charlson ME, Pompei P, Ales KL, MacKenzie CR (1987) A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis 40:373–383
Wehling M, Burkhardt H (2011) Arzneitherapie für Ältere, 2nd edn. Springer, Heidelberg, Germany
Gnjidic D, Bell JS, Hilmer SN, Lönnroos E, Sulkava R, Hartikainen S (2012) Drug Burden Index associated with function in community-dwelling older people in Finland: a cross-sectional study. Ann Med 44:458–467
Tinetti ME, Speechley M, Ginger SF (1988) Risk factors for falls among elderly persons living in the community. N Engl J Med 319:1701–1707
Stel VS, Smit JH, Pluijm SMF, Lips P (2004) Consequences of falling in older men and women and risk factors for health service use and functional decline. Age Ageing 33:58–65
US Congress, Office of Technology Assessment (1994) Hip fracture outcomes in people 50 and over—background paper, OTA-BP-H120. US Government Printing Office, Washington
Ziere G, Dieleman JP, Hofman A, Pols HA, van der Cammen TJ, Stricker BH (2006) Polypharmacy and falls in the middle age and elderly population. Br J Clin Pharmacol 61:218–223
von Renteln-Kruse W, Krause T (2004) Fall events in geriatric hospital in-patients. Results of prospective recording over a 3 year period. Z Gerontol Geriatr 37:9–14
He J, Dunton N, Staggs V (2012) Unit-level time trends in inpatient fall rates of US hospitals. Med Care 50:801–807
van der Velde N, Stricker BH, Pols HA, van der Cammen TJ (2006) Risk of falls after withdrawal of fall-risk-increasing drugs: a prospective cohort study. Br J Clin Pharmacol 63:232–237
Pugh D, Pugh J, Mead GE (2011) Attitudes of physicians regarding anticoagulation for atrial fibrillation: a systematic review. Age Ageing 40:675–683
Author information
Authors and Affiliations
Corresponding author
Electronic supplementary material
Below is the link to the electronic supplementary material.
ESM 1
(DOCX 18 kb)
Rights and permissions
About this article

Cite this article
Michalek, C., Wehling, M., Schlitzer, J. et al. Effects of “Fit fOR The Aged” (FORTA) on pharmacotherapy and clinical endpoints—a pilot randomized controlled study. Eur J Clin Pharmacol 70, 1261–1267 (2014). https://doi.org/10.1007/s00228-014-1731-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00228-014-1731-9