
Abstract
Purpose
For digestive tract cancers, the bilirubin threshold for administration of systemic chemotherapy can be 5 or 2 mg/dL (85.5 or 34.2 μmol/L) depending upon the regimen. We examined the ability of percutaneous biliary drainage (PBD) in patients with malignant biliary obstruction to achieve these clinically relevant endpoints.
Methods
106 consecutive patients with malignant biliary obstruction and a baseline serum bilirubin >2 mg/dL underwent PBD. Time to achieve a bilirubin of 5 mg/dL (85.5 μmol/L), 2 mg/dL (34.2 μmol/L), and survival was estimated by Kaplan–Meier analysis. Potential technical and clinical prognostic factors were subjected to univariate and multivariate analysis. Categorical variables were analyzed by the log rank test. Hazard ratios were calculated for continuous variables.
Results
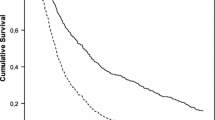
Median survival was 100 days (range 1–3771 days). Among 88 patients with a pre-drainage bilirubin >5 mg/dL, 62% achieved a serum bilirubin ≤5 mg/dL within 30 days and 84% within 60 days, median 21 days. Among 106 patients with a pre-drainage bilirubin >2 mg/dL, 37% achieved a serum bilirubin ≤2 mg/dL by 30 days and 70% within 60 days, median 43 days. None of the technical or clinical factors evaluated, including pre-drainage bilirubin, were significant predictors of time to achieve a bilirubin ≤2 mg/dL (p = 0.51). Size and type of biliary device were the only technical variables found to affect time to bilirubin of 5 mg/dL (p = 0.016).
Conclusion
PBD of malignant obstruction achieves clinically relevant reduction in serum bilirubin in the majority of patients within 1–2 months, irrespective of the pre-drainage serum bilirubin, sufficient to allow administration of systemic chemotherapy. However, the decision to undergo this procedure for this indication alone must be considered in the context of patients’ prognosis and treatment goals.



Similar content being viewed by others


References
King PD (2001) Hepatotoxicity of chemotherapy. Oncologist 6:162–176
Floyd J, Mirza I, Sachs B, Perry MC (2006) Hepatotoxicity of chemotherapy. Semin Oncol 33:50–67
Eklund JW, Trifilio S, Mulcahy MF (2005) Chemotherapy dosing in the setting of liver dysfunction. Oncology (Williston Park) 19:1057–1063
Donelli MG, Zucchetti M, Munzone E, et al. (1998) Pharmacokinetics of anticancer agents in patients with impaired liver function. Eur J Cancer 34:33–46
Venook AP, Egorin MJ, Rosner GL, et al. (2000) Phase 1 and pharmacokinetic trial of gemcitabine in patients with hepatic and renal dysfunction: Cancer and Leukemia Group B 9565. J Clin Oncol 18:2780–2787
Thornton RH, Ulrich R, Hsu M, et al. (2012) Outcomes of patients undergoing percutaneous biliary drainage to reduce bilirubin for administration of chemotherapy. J Vasc Interv Radiol 23:89–95
Adler DG, Baron TH, Davila RE, et al. (2005) ASGE guideline: the role of ERCP in diseases of the biliary tract and the pancreas. Gastrointest Endosc 62:1–8
Weston BR, Ross WA, Wolff RA, et al. (2008) Rate of bilirubin regression after stenting in malignant biliary obstruction for the initiation of chemotherapy. Cancer 112(11):2417–2423
Speer AR, Russell CG, Hatfield AW, et al. (1987) Randomised trial of endoscopic versus percutaneous stent insertion in malignant obstructive jaundice. Lancet 330:57–62
Pinol V, Castellis A, Bordas JM, et al. (2002) Percutaneous self-expanding metal stents versus endoscopic polyethylene endoprostheses for treating malignant biliary obstruction: randomized clinical trial. Radiology 225:27–34
Walter T, Ho CS, Horgan AM, et al. (2013) Endoscopic or percutaneous biliary drainage for Klatskin tumors? J Vasc Interv Radiol 24:113–121
Guidi MA, Curvale C, Viscardi J, et al. (2015) Hilar bile duct tumors: endoscopic or percutaneous drainage? A prospective analysis. Rev Esp Enferm Dig 107:488–494
Mahgerefteh S, Hubert A, Klimov A, Bloom AI (2015) Clinical impact of percutaneous transhepatic insertion of metal biliary endoprostheses for palliation of jaundice and facilitation of chemotherapy. Am J Clin Oncol 38:489–494
Kwang MK, Park JW, Lee JK, et al. (2015) A comparison of preoperative biliary drainage methods for perihilar cholangiocarcinoma: endoscopic versus percutaneous transhepatic biliary drainage. Gut Liver 9(6):791
Saad W, Wallace MJ, Wojak JC, Kundu S, Cardella JF (2010) Quality improvement guidelines for percutaneous transhepatic cholangiography, biliary drainage, and percutaneous cholecystostomy. J Vasc Interv Radiol 21:789–795
Acknowledgments
Supported in part (RM) by Abramson Cancer Center Support Grant (P30-CA016520).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of Interests
All authors declare no conflicts of interest related to the content of this work.
Rights and permissions
About this article

Cite this article
Levy, J.L., Sudheendra, D., Dagli, M. et al. Percutaneous biliary drainage effectively lowers serum bilirubin to permit chemotherapy treatment. Abdom Radiol 41, 317–323 (2016). https://doi.org/10.1007/s00261-015-0580-z
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00261-015-0580-z