
Abstract
Background
It was the aim of this prospective study to evaluate the outcome of laparoscopic surgery for diverticular disease.
Methods
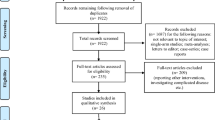
All patients who underwent elective laparoscopic colectomy for diverticular disease within a 10-year period were prospectively entered into a PC database registry. Indications for laparoscopic surgery were acute complicated diverticulitis (Hinchey stages I and IIa), chronically recurrent diverticulitis, sigmoid stenosis or outlet obstruction caused by chronic diverticulitis. Surgical procedures (sigmoid and anterior resection, left colectomy and resection rectopexy) included intracorporeal dissection and colorectal anastomosis. Parameters studied included age, gender, stage of disease, procedure, duration of surgery, intraoperative technical variables, transfusion requirements, conversion rate, total complication rate including major (requiring re-operation), minor (conservative treatment) and late-onset (post-discharge) complication rates, stay on ICU, hospitalisation, mortality, and recurrence. For objective evaluation, only laparoscopically completed procedures were analysed. Comparative outcome analysis was performed with respect to stage of disease and experience.
Results
A total of 396 patients underwent laparoscopic colectomy. Conversion rate was 6.8% (n=27), so that laparoscopic completion rate was 93.2% (n=369). Most common reasons for conversion were directly related to the inflammatory process, abscess or fistulas. The most common procedure was sigmoid resection (n=279), followed by anterior resection (n=36) and left colectomy (n=29). Total complication rate was 18.4% (n=68). Major complication rate was 7.6% (n=28), whereas the most common complication requiring re-operation was haemorrhage in 3.3% (n=12). Anastomotic leakage occurred in 1.6% (n=6). Minor complications were noted in 10.7% (n=40), late-onset complications occurred in 2.7% (n=10). Mortality was 0.5% (n=2). Mean duration of surgery was 193 (range 75–400) min, return to normal diet was completed after 6.8 (range 3–19) days. Mean hospital stay was 11.8 (range 4–71) days. No recurrence of diverticulitis occurred.
Conclusion
Laparoscopic surgery for diverticular disease is safe, feasible and effective. Therefore, laparoscopic colectomy has replaced open resection as standard surgery for recurrent and complicated diverticulitis at our institution.
Similar content being viewed by others


References
Bruch HP, Herold A, Schiedeck T, Schwandner O (1999) Laparoscopic surgery for rectal prolapse and outlet obstruction. Dis Colon Rectum 42:1189–1194
Bruch HP, Schiedeck THK, Schwandner O (1999) Laparoscopic colorectal surgery: a five-year experience. Dig Surg 16:45–54
Schiedeck TH, Schwandner O, Bruch HP (1998) Laparoscopic sigmoid resection in diverticulitis (in German). Chirurg 69:846–853
Gervaz P, Pikarsky A, Utech M, Secic M, Efron J, Belin B, Jain A, Wexner SD (2001) Converted laparoscopic colorectal surgery. Surg Endosc 15:827–832
Le Moine MC, Fabre JM, Vacher C, Navarro F, Picot MC, Domergue J (2003) Factors and consequences of conversion in laparoscopic sigmoidectomy for diverticular disease. Br J Surg 90:232–236
Marusch F, Gastinger I, Schneider C, Scheidbach H, Konradt J, Bruch HP, Koehler L, Baerlehner E, Koeckerling F, Laparoscopic Colorectal Surgery Study Group (LCSSG) (2001) Importance of conversion for results obtained with laparoscopic colorectal surgery. Dis Colon Rectum 44:207–214
Schwandner O, Schiedeck THK, Bruch HP (1999) The role of conversion in laparoscopic colorectal surgery: do predictive factors exist? Surg Endosc 13:151–156
Germer CT, Buhr HJ (2002) Sigmoid diverticulitis. Surgical indications and timing (in German). Chirurg 73:681–689
Koehler L, Sauerland S, Neugebauer E (1999) Diagnosis and treatment of diverticular disease: results of a consensus development conference. The Scientific Committee of the European Association for Endoscopic Surgery. Surg Endosc 13:430–436
Makela J, Vuolio S, Kiviniemi H, Laitinen S (1998) Natural history of diverticular disease: when to operate? Dis Colon Rectum 41:1523–1528
Poulin EC, Schlachta CM, Mamazza J, Seshadri PA (2000) Should enteric fistulas from Crohn’s disease or diverticulitis be treated laparoscopically or by open surgery? A matched cohort study. Dis Colon Rectum 43:621–626
Hinchey EJ, Schaal PG, Richards GK (1978) Treatment of perforated diverticular disease of the colon. Adv Surg 12:85–109
Chautems RC, Ambrosetti P, Ludwig A, Mermillod B, Morel P, Soravia C (2002) Long-term follow-up after first acute episode of sigmoid diverticulitis: is surgery mandatory? A prospective study of 118 patients. Dis Colon Rectum 45:962–966
Makela J, Kiviniemi H, Laitinen S (2002) Prevalence of perforated sigmoid diverticulitis is increasing. Dis Colon Rectum 45:955–961
Bergamaschi R, Arnaud JP (1998) Anastomosis level and specimen length in surgery for uncomplicated diverticulitis of the sigmoid. Surg Endosc 12:1149–1151
Thaler K, Baig MK, Berho M, Weiss EG, Nogueras JJ, Arnaud JP, Wexner SD, Bergamaschi R (2003) Determinants of recurrence after sigmoid resection for uncomplicated diverticulitis. Dis Colon Rectum 46:385–388
Berthou JC, Charbonneau P (1999) Elective laparoscopic management of sigmoid diverticulitis. Results in a series of 110 patients. Surg Endosc 13:457–460
Bouillot JL, Aouad K, Badawy A, Alamowitch B, Alexandre JH (1998) Elective laparoscopic-assisted colectomy for diverticular disease. A prospective study in 50 patients. Surg Endosc 12:1393–1396
Bruce CJ, Coller JA, Murray JJ, Schoetz DJ Jr, Roberts PL, Rusir LC (1996) Laparoscopic resection for diverticular disease. Dis Colon Rectum 39 [Suppl]:S1–6
Eijsbouts QA, Cuesta MA, de Brauw LM, Sietses C (1997) Elective laparoscopic-assisted sigmoid resection for diverticular disease. Surg Endosc 11:750–753
Franklin MEJ, Dorman JP, Jacobs M, Plasencia G (1997) Is laparoscopic surgery applicable to complicated colonic diverticular disease? Surg Endosc 11:1021–1025
Koeckerling F, Schneider C, Reymond MA, Scheidbach H, Scheuerlein H, Konradt J, Bruch HP, Zornig C, Koehler L, Baerlehner E, Kuthe A, Szinicz G, Richter HA, Hohenberger W, Laparoscopic Colorectal Surgery Study Group (1999) Laparoscopic resection of sigmoid diverticulitis. Results of a multicenter study. Surg Endosc 13:567–571
Koehler L, Rixen D, Troidl H (1998) Laparoscopic colorectal resection for diverticulitis. Int J Colorectal Dis 13:43–47
Sher ME, Agachan F, Bortul M, Nogueras JJ, Weiss EG, Wexner SD (1997) Laparoscopic surgery for diverticulitis. Surg Endosc 11:264–267
Sirisier F (1999) Laparoscopic-assisted colectomy for diverticular sigmoiditis. A single-surgeon prospective study of 65 patients. Surg Endosc 13:811–813
Smadja C, Sbai Idrissi M, Tahrat M, Vons C, Bobocescu E, Baillet P, Franco D (1999) Elective laparoscopic sigmoid colectomy for diverticulitis. Results of a prospective study. Surg Endosc 13:645–648
Stevenson ARL, Stitz R, Lumley J, Fielding G (1998) Laparoscopically assisted anterior resection for diverticular disease: follow-up of 100 consecutive patients. Ann Surg 227:335–342
Vargas HD, Ramirez RT, Hoffman GC, Hubbard GW, Gould RJ, Wohlgemuth SD, Ruffin WK, Hatter JE, Kolm P (2000) Defining the role of laparoscopic-assisted sigmoid colectomy for diverticulitis. Dis Colon Rectum 43:1726–1731
Bergamaschi R, Tuech JJ, Cervi C, Arnaud JP (2000) Re-establish pneumoperitoneum in laparoscopic-assisted sigmoid resection? Randomized trial. Dis Colon Rectum 43:771–774
Bergamaschi R, Tuech JJ, Pessaux P, Arnaud JP (2000) Intracorporeal vs laparoscopic-assisted resection for uncomplicated diverticulitis of the sigmoid. Surg Endosc 14:520–523
Bouillot JL, Berthou JC, Champault G, Meyer C, Arnaud JP, Samama G, Collet D, Bressler P, Gainant A, Delaitre B (2002) Elective laparoscopic colonic resection for diverticular disease. Results of a multicenter study in 179 patients. Surg Endosc 16:1320–1323
Liberman MA, Phillips EH, Carroll BJ, Fallas M, Rosenthal R (1996) Laparoscopic colectomy vs traditional colectomy for diverticulitis. Outcome and costs. Surg Endosc 10:15–18
Menenakos E, Hahnloser D, Nassiopoulos K, Chanson C, Sinclair V, Petropoulos P (2003) Laparoscopic surgery for fistulas that complicate diverticular disease. Langenbecks Arch Surg 388:189–193
Senagore AJ, Duepree HJ, Delaney CP, Brady KM, Fazio VW (2003) Results of a standardized technique and postoperative care plan for laparoscopic sigmoid colectomy: a 30-month experience. Dis Colon Rectum 46:503–509
Senagore AJ, Duepree HJ, Delaney CP, Dissanaike S, Brady KM, Fazio VW (2002) Cost structure of laparoscopic and open sigmoid colectomy for diverticular disease: similarities and differences. Dis Colon Rectum 45:485–490
Dwivedi A, Chahin F, Agrawal S, Chau WY, Tootla A, Tootla F, Silva YJ (2002) Laparoscopic colectomy vs open colectomy for sigmoid diverticular disease. Dis Colon Rectum 45:1309–1314
Faynsod M, Stamos MJ, Arnell T, Borden C, Udani S, Vargas H (2000) A case–control study of laparoscopic vs open sigmoid colectomy for diverticulitis. Am Surg 66:841–843
Lawrence DM, Pasquale MD, Wasser TE (2003) Laparoscopic versus open sigmoid colectomy for diverticulitis. Am Surg 69:499–503
Trebuchet G, Lechaux D, Lecalve JL (2002) Laparoscopic left colon resection for diverticular disease. Surg Endosc 16:18–21
Tuech JJ, Regenet N, Hennekinne S, Pessaux P, Bergamaschi R, Arnaud JP (2001) Laparoscopic colectomy for sigmoid diverticulitis in obese and nonobese patients: a prospective comparative study. Surg Endosc 15:1427–1430
Tuech JJ, Pessaux P, Rouge C, Regenet N, Bergamaschi R, Arnaud JP (2000) Laparoscopic vs open colectomy for sigmoid diverticulitis: a prospective study in the elderly. Surg Endosc 14:1031–1033
Acknowledgements
The authors thank Mrs. C. Killaitis for processing the prospective PC database registry and for statistical evaluation. The work was supported by a grant from Stiftung Coloplast, Hamburg, Germany.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schwandner, O., Farke, S., Fischer, F. et al. Laparoscopic colectomy for recurrent and complicated diverticulitis: a prospective study of 396 patients. Langenbecks Arch Surg 389, 97–103 (2004). https://doi.org/10.1007/s00423-003-0454-7
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00423-003-0454-7