
Abstract
Background
A percutaneous minimally invasive fetoscopic approach was attempted for closure of a spina bifida aperta in two fetuses with L5 lesions. The goal was to obviate the need for postnatal neurosurgery to manage this condition.
Methods and Results
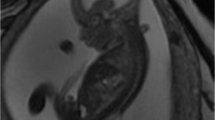
The percutaneous fetoscopic procedures were performed by a two-layer approach at respectively 22 ± 2 and 22 ± 4 weeks of gestation. The fetuses were delivered respectively at 32 ± 6 and 32 + 3 weeks of gestation. Their neural cords were completely covered although in small areas skin closure was incomplete. Postnatally, complete skin closure occurred beneath an occlusive draping within 2 to 3 weeks such that neurosurgical intervention was not required. Both neonates showed reversal of hindbrain herniation, near-normal leg function, and satisfactory bladder and bowel function. For one of the two fetuses, ventriculoperitoneal shunt insertion was not required.
Conclusions
Percutaneous minimally invasive fetoscopic patch closure of spina bifida aperta offers a substantially less maternal trauma than open fetal surgical repair and currently may even obviate the need for postnatal neurosurgical repair. With a little further improvement in surgical techniques and a better understanding of incorporating surgical patches into the fetus, complete skin closure seems possible in the near future.


Similar content being viewed by others

References
Kohl T, Große Hartlage M, Kienitz D, Westphal M, Buller T, Achenbach S, Gembruch U, Brentrup A (2003) Percutaneous fetoscopic patch coverage of experimental lumbosacral full-thickness skin lesions in sheep: a minimally invasive technique aimed at minimizing maternal trauma from fetal surgery for myelomeningocele. Surg Endosc 17:1218–1223
Kohl T, Hering R, Heep A, Schaller C, Meyer B, Greive C, Bizjak G, Buller T, Van de Vondel P, Gogarten W, Bartmann P, Knöpfle G, Gembruch U (2006) Percutaneous fetoscopic patch coverage of spina bifida aperta in the human: early clinical experience and potential. Fetal Diagn Ther 21:185–193
Walsh DS, Adzick NS, Sutton LN, Johnson MP (2001) The rationale for in utero repair of myelomeningocele. Fetal Diagn Ther 16:312–322
Sutton LN, Adzick NS, Bilaniuk LT, Johnson MP, Crombleholme TM, Flake AW (1999) Improvement in hindbrain herniation demonstrated by serial fetal magnetic resonance imaging following fetal surgery for myelomeningocele. JAMA 282:1826–1831
Tulipan N, Hernanz-Schulman M, Lowe HJ, Bruner JP (1999) Intrauterine myelomeningocele repair reverses preexisting hindbrain herniation. Pediatr Neurosurg 31:137–142
Johnson MP, Sutton LN, Rintoul N, Crombleholme TM, Flake AW, Howell LJ, Hedrick HL, Wilson RD, Adzick NS (2003) Fetal myelomeningocele repair: short-term clinical outcomes. Am J Obstet Gynecol 189:482–487
Tulipan N, Sutton LN, Bruner JP, Cohen BM, Johnson M, Adzick NS (2003) The effect of intrauterine myelomeningocele repair on the incidence of shunt-dependent hydrocephalus. Pediatr Neurosurg 38:27–33
Bruner JP, Tulipan N, Reed G, Davis GH, Bennet K, Luker KS, Dabrowiak ME (2004) Intrauterine repair of spina bifida: preoperative predictors of shunt-dependent hydrocephalus. Am J Obstet Gynecol 190:1305–1312
Copeland ML, Bruner JP, Richards WO, Sundell HW, Tulipan NB (1993) A model for in utero endoscopic treatment of myelomeningocele. Neurosurgery 33:542–544
Bruner JP, Tulipan NE, Richards WO (1997) Endoscopic coverage of fetal open myelomeningocele in utero. Am J Obstet Gynecol 176:256–257
Bruner JP, Tulipan NB, Richards WO, Walsh WF, Boehm FH, Vrabcak EK (2000) In utero repair of myelomeningocele: a comparison of endoscopy and hysterotomy. Fetal Diagn Ther 15:83–88
Farmer DL, von Koch CS, Warwick JP, Danielpour M, Gupta N, Lee H, Harrison MR (2003) In utero repair of myelomeningocele. Arch Surg 138:872–878
Kohl T, Szabo Z, Suda K, Quinn TM, Petrossian E, Harrison MR, Hanley FL (1997) Percutaneous fetal access and uterine closure for fetoscopic surgery: lessons learned from 16 consecutive procedures in pregnant sheep. Surg Endosc 11:819–824
Kohl T, Witteler R, Strümper D, Gogarten W, Asfour B, Reckers J, Merschhoff G, Marcus AE, Weyand M, Van Aken H, Vogt J, Scheld HH (2000) Operative techniques and strategies for minimally invasive fetoscopic fetal cardiac interventions in sheep. Surg Endosc 14:424–430
Kohl T, Reckers J, Strümper D, Große Hartlage D, Gogarten W, Gembruch U, Vogt J, Van Aken H, Scheld HH, Paulus W, Rickert CH (2004) Amniotic air insufflation during minimally invasive fetoscopic fetal cardiac interventions is safe for the fetal brain in sheep. J Thorac Cardiovasc Surg 128:467–471
Kohl T, Hering R, Van de Vondel P, Tchatcheva K, Berg C, Bartmann P, Heep A, Franz A, Müller A, Gembruch U (2006) Analysis of the step-wise clinical introduction of experimental percutaneous fetoscopic surgical techniques for upcoming minimally-invasive fetal cardiac interventions. Surg Endosc 20:1134–1143
Hering R, Wenningmann I, Tchatcheva K, Stressig R, Gembruch U, Kohl T (2008) A protocol for safe general maternofetal anesthesia during minimally invasive fetal surgery. Ultraschall Med 29:90
Kohl T, Weinbach J, Tchatcheva K, Stressig R, Van de Vondel P, Gembruch U (2008) Early clinical experience with partial amniotic carbon dioxide insufflation (PACI) during fetoscopic surgery in human fetuses. Ultraschall Med 29:90
Acknowledgments
The development of the minimally invasive fetoscopic technique has been supported by educational and research grants Ko 1484/1-1, Ko 1484/2-1, Ko 1484/3-1, Ko 1484/3-2, Ko 1484/3-3 of the Deutsche Forschungsgemeinschaft (DFG), Bonn, Germany.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Kohl, T., Tchatcheva, K., Merz, W. et al. Percutaneous fetoscopic patch closure of human spina bifida aperta: advances in fetal surgical techniques may obviate the need for early postnatal neurosurgical intervention. Surg Endosc 23, 890–895 (2009). https://doi.org/10.1007/s00464-008-0153-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-008-0153-0