
Abstract
Background
Obesity and gastroesophageal reflux disease (GERD) are commonly associated diseases. Bariatric surgery has been shown to have various impacts on esophageal function and GERD. Our aim was to evaluate changes in symptoms, endoscopic findings, bolus passage and esophageal function in patients after primary gastric bypass surgery as compared to patients converted from gastric banding to gastric bypass.
Methods
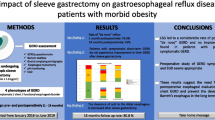
Obese patients scheduled for laparoscopic Roux-en-Y gastric bypass (naïve-to-bypass) and patients who previously underwent gastric banding and were considered for conversion from gastric banding to gastric bypass (band-to-bypass) were included. Patients rated esophageal and epigastric symptoms (100 point VAS) and underwent upper endoscopy, impedance–manometry, and modified “timed barium swallow” before/after surgery.
Results
Data from 66 naïve-to-bypass patients (51/66, 77 % females, mean age 41.2 ± 11.1 years) and 68 band-to-bypass patients (53/68, 78 % females, mean age 43.8 ± 10.0 years) were available for analysis. Esophageal symptoms, esophagitis, esophageal motility abnormalities and impaired esophageal bolus transit were more common in patients that underwent gastric banding compared to those that underwent gastric bypass. The majority of symptoms, lesions and abnormalities induced by gastric banding were decreased by conversion to gastric bypass. Esophagitis was present in 28/68 (41 %) and 13/47 (28 %) patients in the band-to-bypass group, pre- versus postoperatively, respectively, (p < 0.05). The percentage of swallows with normal bolus transit increased following transformation from gastric band to gastric bypass (57.9 ± 4.1 and 83.6 ± 3.4 %, respectively, p < 0.01).
Conclusions
From an esophageal perspective, gastric bypass surgery induces less motility disorders and esophageal symptoms and should be therefore favored over gastric banding in difficult to treat obese patients at risk of repeated bariatric surgery.




Similar content being viewed by others


Abbreviations
- BMI:
-
Body mass index
- BTT:
-
Bolus transit time
- DEA:
-
Distal esophageal amplitude
- EFT:
-
Esophageal function testing
- GERD:
-
Gastroesophageal reflux disease
- GI:
-
Gastrointestinal
- HPZ:
-
High-pressure zone
- LA:
-
Los Angeles classification
- LASGB:
-
Laparoscopic adjustable silicone gastric banding
- LES:
-
Lower esophageal sphincter
- LRYGBP:
-
Laparoscopic Roux-en-Y gastric bypass
- LVBG:
-
Laparoscopic vertical banded gastroplasty
- MII-EM:
-
Combined impedance–manometry
- PPIs:
-
Proton pump inhibitors
References
Ogden CL, Carroll MD, Curtin LR, McDowell MA, Tabak CJ, Flegal KM (2006) Prevalence of overweight and obesity in the United States, 1999–2004. JAMA 295:1549–1555
El-Serag HB, Graham DY, Satia JA, Rabeneck L (2005) Obesity is an independent risk factor for GERD symptoms and erosive esophagitis. Am J Gastroenterol 100:1243–1250
Jacobson BC, Somers SC, Fuchs CS, Kelly CP, Camargo CA Jr (2006) Body-mass index and symptoms of gastroesophageal reflux in women. N Engl J Med 354:2340–2348
Vaezi MF, Baker ME, Achkar E, Richter JE (2002) Timed barium oesophagram: better predictor of longterm success after pneumatic dilation in achalasia than symptom assessment. Gut 50:765–770
Spechler SJ, Castell DO (2001) Classification of oesophageal motility abnormalities. Gut 49:145–151
Tutuian R, Vela MF, Balaji NS, Wise JL, Murray JA, Peters JH, Shay SS, Castell DO (2003) Esophageal function testing with combined multichannel intraluminal impedance and manometry: multicenter study in healthy volunteers. Clin Gastroenterol Hepatol 1:174–182
Naef M, Mouton WG, Naef U, van der Weg B, Maddern GJ, Wagner HE (2011) Esophageal dysmotility disorders after laparoscopic gastric banding—an underestimated complication. Ann Surg 253:285–290
de Jong JR, Besselink MG, van Ramshorst B, Gooszen HG, Smout AJ (2010) Effects of adjustable gastric banding on gastroesophageal reflux and esophageal motility: a systematic review. Obes Rev 11:297–305
Dixon JB, O’Brien PE (1999) Gastroesophageal reflux in obesity: the effect of lap-band placement. Obes Surg 9:527–531
Rebecchi F, Rocchietto S, Giaccone C, Talha A, Morino M (2011) Gastroesophageal reflux disease and esophageal motility in morbidly obese patients submitted to laparoscopic adjustable silicone gastric banding or laparoscopic vertical banded gastroplasty. Surg Endosc 25:795–803
Perry Y, Courcoulas AP, Fernando HC, Buenaventura PO, McCaughan JS, Luketich JD (2004) Laparoscopic Roux-en-Y gastric bypass for recalcitrant gastroesophageal reflux disease in morbidly obese patients. JSLS 8:19–23
Acknowledgments
We like to specifically acknowledge the hard work of our study nurse Patrizia Künzler with regard to patient and data management.
Funding
This study was funded by the Research Council of the University of Zurich and registered at ClinicalTrials.gov (NCT00680030).
Author’s contribution
Jan Borovicka and Radu Tutuian equally contributed to the study design, planned the study protocol. Both of them also performed data analysis and wrote the manuscript. Radu Tutuian obtained funding from the study from the Research Foundation of the University Hospital of Zurich/University of Zurich. Claudia Krieger-Gruebel, Boudewijn van der Weg, Michael Christian Sulz, and Philipp Bisang performed the procedures and analyzed the data. Martin Thurnheer performed all gastric bypass surgeries. Bernd Schultes and Jean-Pierre Gutzwiler performed data analysis and approved the final draft. Daniel Pohl wrote the study protocol. Michael Fried and Christa Meyenberger critically reviewed the analysis and approved the final draft. All authors have read and approved the final version of the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Disclosures
Radu Tutuian contributes to educational programs of Sandhill Scientific Inc. and Medical Measurements Systems (MMS) International. Travel support and speaker honoraria were received from Allmiral, AbbVie, Abbott, UCB in the past 2 years. Jan Borovicka, Claudia Krieger-Gruebel, Boudewijn van der Weg, Michael Christian Sulz, Philipp Bisang, Martin Thurnheer, Bernd Schultes, Jean-Pierre Gutzwiler, Daniel Pohl, Michael Fried, and Christa Meyenberger have no conflicts of interests that are relevant to the manuscript.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
About this article

Cite this article
Borovicka, J., Krieger-Grübel, C., van der Weg, B. et al. Effect of morbid obesity, gastric banding and gastric bypass on esophageal symptoms, mucosa and function. Surg Endosc 31, 552–560 (2017). https://doi.org/10.1007/s00464-016-4996-5
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00464-016-4996-5