
Abstract
Introduction
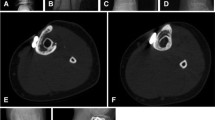
Combining massive bone allograft and vascularized fibula in intercalary reconstruction following resection of bone tumors represents a complex reconstructive procedure that requires specialists in microvascular surgery as well as orthopedic surgery. The purpose of our study was to examine the outcomes using this surgical technique in patients with bone tumors in terms of oncologic results, complications related to surgery, Musculoskeletal Tumor Society (MSTS) scores and duration of surgery.
Materials and methods
We analyzed 81 patients with femoral or tibial sarcomas who underwent intercalary resection and microsurgical reconstruction with massive bone allograft and vascularized fibula. There were 56 boys and 25 girls with a mean age of 13.4 years at the time of surgery. The patients’ medical records were reviewed for clinical and functional outcomes as well as postoperative complications. The study group was comprised of 33 patients who underwent reconstruction of the femur with massive bone allograft and free vascularized fibula and 48 patients who underwent reconstruction of the tibia with massive bone allograft and free or pedicle vascularized fibula. The mean length of resection was 15.9 cm (8–31 cm). The functional evaluation of the patients was done at the end of the follow-up using MSTS score for the lower limb. All patients had at least a 2-year follow-up.
Results
The overall limb salvage rate was 94%, although many patients required re-operation after the procedure. Complications occurred in 24 patients, 18 of which underwent additional surgical procedures. They included fractures of the massive bone allograft-vascularized fibula construct with or without implant failure (19) and deep infection (5). After surgical or conservative treatment, all the fractures successfully healed. The overall MSTS functional score was good to excellent in 91% of patients.
Conclusions
The combination of massive bone allograft and vascularized fibula seems to be a reasonable option for reconstruction of diaphyseal defects following intercalary resection of bone tumors. Although there was a high rate of complications and therefore re-operations, the biology of vascularized fibula was able to save the reconstruction in most of the cases that had complications.

Similar content being viewed by others


References
Muramatsu K, Hashimoto T, Tominaga Y, Taguchi T (2014) Vascularized bone graft for oncological reconstruction of the extremities: review of the biological advantages. Anticancer Res 34:2701–2707
Ghert M, Colterjohn N, Manfrini M (2007) The use of free vascularized fibular grafts in skeletal reconstruction for bone tumors in children. J Am Acad Orthop Surg 15:577–587
Donati D, D’Arenzo R, Ercolani C, Boriani S (1995) Infection in limb salvage surgery for bone tumors. Eur J Orthop Surg Traumatol Orthop Traumatol 5:71–74. https://doi.org/10.1007/BF02716222
Lesenský J, Mavrogenis AF, Igoumenou VG et al (2017) Complex surgery for locally advanced bone and soft tissue sarcomas of the shoulder girdle. Eur J Orthop Surg Traumatol Orthop Traumatol 27:777–786. https://doi.org/10.1007/s00590-017-1999-4
Lesensky J, Prince DE (2017) Distraction osteogenesis reconstruction of large segmental bone defects after primary tumor resection: pitfalls and benefits. Eur J Orthop Surg Traumatol Orthop Traumatol 27:715–727. https://doi.org/10.1007/s00590-017-1998-5
Staats K, Panotopoulos J, Tiefenboeck TM et al (2017) Computer navigation-assisted surgery for musculoskeletal tumors: a closer look into the learning curve. Eur J Orthop Surg Traumatol Orthop Traumatol 27:851–858. https://doi.org/10.1007/s00590-017-2004-y
Panagopoulos GN, Mavrogenis AF, Mauffrey C et al (2017) Intercalary reconstructions after bone tumor resections: a review of treatments. Eur J Orthop Surg Traumatol Orthop Traumatol 27:737–746. https://doi.org/10.1007/s00590-017-1985-x
Valente G, Taddei F, Roncari A et al (2017) Bone adaptation of a biologically reconstructed femur after Ewing sarcoma: long-term morphological and densitometric evolution. Skeletal Radiol 46:1271–1276. https://doi.org/10.1007/s00256-017-2661-2
Houdek MT, Wagner ER, Stans AA et al (2016) What Is the outcome of allograft and intramedullary free fibula (Capanna technique) in pediatric and adolescent patients with bone tumors? Clin Orthop 474:660–668. https://doi.org/10.1007/s11999-015-4204-2
Innocenti M, Abed YY, Beltrami G et al (2009) Biological reconstruction after resection of bone tumors of the proximal tibia using allograft shell and intramedullary free vascularized fibular graft: long-term results. Microsurgery 29:361–372. https://doi.org/10.1002/micr.20668
Ceruso M, Taddei F, Bigazzi P, Manfrini M (2008) Vascularised fibula graft inlaid in a massive bone allograft: considerations on the bio-mechanical behaviour of the combined graft in segmental bone reconstructions after sarcoma resection. Injury 39(Suppl 3):S68–S74. https://doi.org/10.1016/j.injury.2008.05.014
Longhi A, Errani C, De Paolis M et al (2006) Primary bone osteosarcoma in the pediatric age: state of the art. Cancer Treat Rev 32:423–436. https://doi.org/10.1016/j.ctrv.2006.05.005
Capanna R, Campanacci DA, Belot N et al (2007) A new reconstructive technique for intercalary defects of long bones: the association of massive allograft with vascularized fibular autograft. Long-term results and comparison with alternative techniques. Orthop Clin North Am 38:51–60. https://doi.org/10.1016/j.ocl.2006.10.008
Chang DW, Weber KL (2005) Use of a vascularized fibula bone flap and intercalary allograft for diaphyseal reconstruction after resection of primary extremity bone sarcomas. Plast Reconstr Surg 116:1918–1925
Muscolo DL, Ayerza MA, Aponte-Tinao L et al (2004) Intercalary femur and tibia segmental allografts provide an acceptable alternative in reconstructing tumor resections. Clin Orthop 426:97–102
Bus MPA, Dijkstra PDS, van de Sande MAJ et al (2014) Intercalary allograft reconstructions following resection of primary bone tumors: a nationwide multicenter study. J Bone Joint Surg Am 96:e26. https://doi.org/10.2106/JBJS.M.00655
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
All authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Errani, C., Ceruso, M., Donati, D.M. et al. Microsurgical reconstruction with vascularized fibula and massive bone allograft for bone tumors. Eur J Orthop Surg Traumatol 29, 307–311 (2019). https://doi.org/10.1007/s00590-018-2360-2
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s00590-018-2360-2