
Abstract
Purpose
This study aims to assess the influence of ECG-gated acquisition on workflow and to compare image quality and diagnostic certainty for retrospectively ECG-gated and nongated multidetector computed tomography of the chest in the emergency suite.
Materials and methods
Thirty-two consecutive patients were referred for both an ECG-gated and a nongated CT to rule out traumatic thoracic injury (n=15) or acute aortic dissection (n=17). The time from the start of the transportation from the emergency suite to the CT room until the start of the CT scan was recorded. Using a scoring system, the image quality of axial images and multiplanar reformats, the presence of disease, and the subjective diagnostic certainty were assessed with regard to the vascular structures, the bone structures, and the lung parenchyma.
Results
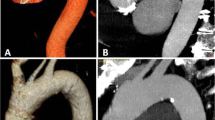
The time needed for transportation and patient preparation was 12.1±1.7 min (8.1–14.5 min). The motion artifacts of the thoracic aorta and the supra-aortic vessels were significantly reduced in the ECG-gated data acquisition compared with the nongated technique (P<0.001). Subjective diagnostic certainty for assessment of the aorta was significantly better using ECG gating. The image quality of the lung parenchyma (P<0.005), the spine (P<0.005), and the ribs (P<0.002) was inferior in the ECG-gated data sets but did not compromise the detection rate of traumatic lesions and fractures.
Conclusion
Performing ECG gating in the emergency room did not slow down the diagnostic workup. ECG-gated acquisition performed better in the assessment of the aorta, but image quality for lung and bone structures was slightly reduced. Further studies are required to assess the influence of the imaging technique on the diagnostic outcome.







Similar content being viewed by others

References
Rieger M, Sparr H, Esterhammer R et al (2002) Modern CT diagnosis of acute thoracic and abdominal trauma. Radiologe 42:556–563
Feczko JD, Lynch L, Pless JE, Clark MA, McClain J, Hawley DA (1992) An autopsy case review of 142 nonpenetrating (blunt) injuries of the aorta. J Trauma 33:846–849
Wintermark M, Wicky S, Schnyder P (2002) Imaging of acute traumatic injuries of the thoracic aorta. Eur Radiol 12:431–442
Khan IA, Nair CK (2002) Clinical, diagnostic, and management perspectives of aortic dissection. Chest 122:311–328
Hagan PG, Nienaber CA, Isselbacher EM et al (2000) The International Registry of Acute Aortic Dissection (IRAD): new insights into an old disease. JAMA 283:897–903
Mirvis SE, Shanmuganathan K, Miller BH, White CS, Turney SZ (1996) Traumatic aortic injury: diagnosis with contrast-enhanced thoracic CT—five-year experience at a major trauma center. Radiology 200:413–422
Gavant ML, Flick P, Menke P, Gold RE (1996) CT aortography of thoracic aortic rupture. AJR Am J Roentgenol 166:955–961
Fishman JE (2000) Imaging of blunt aortic and great vessel trauma. J Thorac Imaging 15:97–103
Roos JE, Willmann JK, Weishaupt D, Lachat M, Marincek B, Hilfiker PR (2002) Thoracic aorta: motion artifact reduction with retrospective and prospective electrocardiography-assisted multi-detector row CT. Radiology 222:271–277
Ohnesorge B, Flohr T, Becker C et al (2000) Cardiac imaging by means of electrocardiographically gated multisection spiral CT: initial experience. Radiology 217:564–571
Kachelriess M, Ulzheimer S, Kalender WA (2000) ECG-correlated image reconstruction from subsecond multi-slice spiral CT scans of the heart. Med Phys 27:1881–1902
Vogl TJ, Abolmaali ND, Diebold T et al (2002) Techniques for the detection of coronary atherosclerosis: multi-detector row CT coronary angiography. Radiology 223:212–220
Kalender WA, Schmidt B, Zankl M, Schmidt M (1999) A PC program for estimating organ dose and effective dose values in computed tomography. Eur Radiol 9:555–562
McLaughlin JS, Shama Z, Hirsch E, Khazei AH, Attar S, Cowley A (1969) Cardiovascular dynamics in human shock. Am Surg 35:166–176
Roos JE, Hilfiker P, Platz A et al (2004) MDCT in emergency radiology: is a standardized chest or abdominal protocol sufficient for evaluation of thoracic and lumbar spine trauma? AJR Am J Roentgenol 183:959–968
Nieman K, Rensing BJ, van Geuns RJ et al (2002) Non-invasive coronary angiography with multislice spiral computed tomography: impact of heart rate. Heart 88:470–474
Ben-Menachem Y (1993) Rupture of the thoracic aorta by broadside impacts in road traffic and other collisions: further angiographic observations and preliminary autopsy findings. J Trauma 35:363–367
Creasy JD, Chiles C, Routh WD, Dyer RB (1997) Overview of traumatic injury of the thoracic aorta. Radiographics 17:27–45
Cheng I, McLellan BA, Joyner C, Christakis G (2000) Aortic root trauma: serious injuries requiring early recognition and management. J Trauma 48:525–529
Bashar AH, Kazui T, Washiyama N et al (2002) Stanford type a aortic dissection after blunt chest trauma: case report with a reflection on the mechanism of injury. J Trauma 52:380–381
Ono M, Yagyu K, Furuse A, Kotsuka Y, Kubota H (1998) A case of Stanford type A acute aortic dissection caused by blunt chest trauma. J Trauma 44:543–544
Perchinsky M, Gin K, Mayo JR (1998) Trauma-associated dissection of the thoracic aorta. J Trauma 45:626–629
Gammie JS, Katz WE, Swanson ER, Peitzman AB (1996) Acute aortic dissection after blunt chest trauma. J Trauma 40:126–127
Acknowledgements
This research has been supported by the NCCR CO-ME of the Swiss National Science Foundation. We thank Ulrich Helfenstein, MD, and Burkhardt Seifert, PhD, for their contributions to the statistical analyses.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Schertler, T., Glücker, T., Wildermuth, S. et al. Comparison of retrospectively ECG-gated and nongated MDCT of the chest in an emergency setting regarding workflow, image quality, and diagnostic certainty. Emerg Radiol 12, 19–29 (2005). https://doi.org/10.1007/s10140-005-0435-y
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s10140-005-0435-y